-
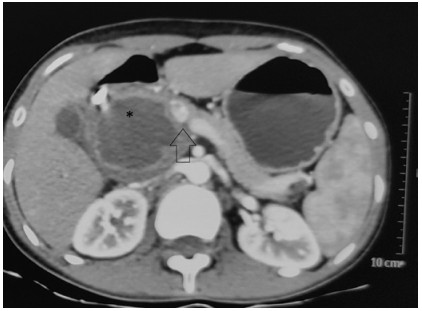
Figure 1.
Pancreatic protocol CT showing solid pseudopapillary lesion seen in the head of pancreas (* mark), (arrow) showing the close abutment of the lesion with portomesenteric and SV junction (Ishikawa type Ⅱ venous invasion).
-
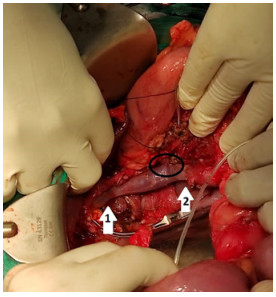
Figure 2.
Post-pancreatoduodenectomy showing proximal anastomosis (arrow 1) of PV with IJV graft and distal anastomosis (arrow 2) with SMV with IJV graft. The SV is shown (circle) implanted into the IJV graft in anatomical position.
-
Method/graft used Indication Advantages Disadvantages Direct venorrhaphy ISGPS type 1, Ishikawa Ⅰ/Ⅱ Simple, less time consuming May cause narrowing of venous caliber. May lead to PVT, may at times have compromised venous margins Partial venous excision with/without peritoneal patch ISGPS type 2, Ishikawa Ⅱ/Ⅲ Simple, less time consuming May cause narrowing of venous caliber. May lead to PVT, may at times have compromised venous margins Segmental venous resection with primary venous reconstruction ISGPS type 3, Ishikawa Ⅱ, Ⅲ, Ⅳ Better oncological margins Comparatively increased operating time & chances of PVT Interposed graft with IJV ISGPS type 4, Ishikawa Ⅲ, Ⅳ, Ⅴ Better oncological margins, tension-free repair, can cover larger venous defects Chances of PVT due to added anastomotic sites, increased operating time and blood loss
Needs a separate neck dissection which can rarely cause donor site complications.
Comparatively less overall complication rateInterposed graft with external iliac vein ISGPS type 4, Ishikawa Ⅲ, Ⅳ, Ⅴ Better oncological margins, tension free repair, can cover larger venous defects, graft harvesting from same incision Chances of PVT due to added anastomotic sites, increased operating time and blood loss. Increased donor site complications & DVT Interposed graft with saphenous vein (paneled) ISGPS type 4, Ishikawa Ⅲ, Ⅳ, Ⅴ Can cover larger defects Needs separate incision, larger anastomotic site high chances of PVT, technically very difficult, longer operating time and increased blood loss Interposed graft with left renal vein ISGPS type 4, Ishikawa Ⅲ, Ⅳ, Ⅴ Can cover longer defects, harvested via same incision Donor site complications like thrombosis or renal congestion Interposed graft with PTFE ISGPS type 4, Ishikawa Ⅲ, Ⅳ, Ⅴ Can cover larger area of defect, added incision or dissection not needed Higher chances of PVT, high blood loss notes, high risk of infection PVT, portal vein thrombosis; PTFE, polytetrafluoroethylene. Table 1.
Different methods and interposition grafts used for venous reconstruction
Figures
(2)
Tables
(1)