-
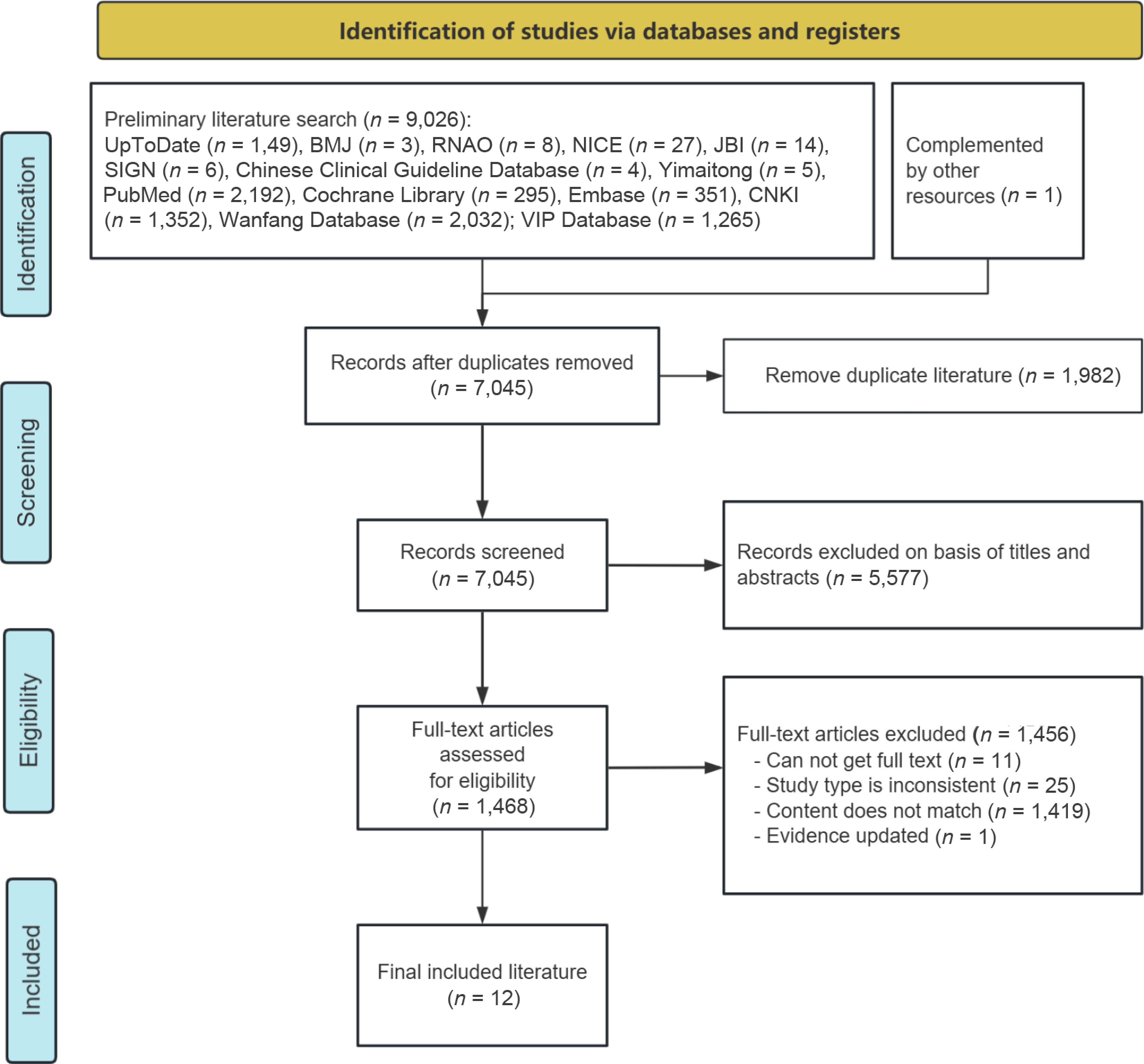
Figure 1.
Flow chart of literature retrieval and screening.
-
Author Year Country Article type Article source Research theme Mortensen et al.[16] 2014 Norway, Sweden, France, Switzerland, Italy, Canada, UK Guideline Yimaitong Consensus guidelines for enhanced recovery after gastrectomy Irani et al.[27] 2023 The United States Guideline PubMed Clinical practice guidelines for enhanced recovery after colon and rectal surgery from the American society of colon and rectal surgeons and the society of American gastrointestinal and endoscopic surgeons Chen et al.[28] 2018 China Guideline Yimaitong Chinese consensus and clinical guidelines for enhanced recovery after surgery (2018 edition) Liu et al.[29] 2018 China RCT CNKI Implementation of quantitative ambulation schemes in enhanced recovery after surgery for gastric cancer patients Ni et al.[30] 2023 China RCT CNKI The application of enhanced recovery after surgery nursing pathway in laparoscopic radical gastrectomy for gastric cancer Lee et al.[31] 2025 Korea RCT PubMed Effectiveness of ERAS program on postoperative recovery after gastric cancer surgery: a randomized clinical trial He et al.[32] 2022 China RCT Cochrane Library Fast-track surgery nursing intervention in CRC patients with laparotomy and laparoscopic surgery Gao et al.[33] 2020 China RCT Cochrane Library Effect of fast-track surgery nursing on postoperative rehabilitation of patients undergoing laparoscopic radical gastrectomy Association[34] 2017 China Expert consensus Yimaitong Expert consensus on enhanced recovery after gastrectomy for gastric cancer (2016 edition) Surgery[35] 2016 China Expert consensus Yimaitong Chinese expert consensus on enhanced recovery after surgery in perioperative management (2016 edition) Tian et al.[36] 2024 China Systematic review PubMed The efficacy and safety of enhanced recovery after surgery (ERAS) Program in laparoscopic distal gastrectomy: a systematic review and meta-analysis of randomized controlled trials Hu et al.[37] 2021 China Quasi-experimental study CNKI Application of best evidence for early postoperative ambulation in gastric cancer patients Note: RCT, randomized controlled trial. Table 1.
General characteristics of the included articles (n = 12).
-
Guideline Standardized scores in various domains (%) ≥ 60% ≥ 30% Quality evaluation Scope and purpose Stakeholder involvement Rigour of development Clarity of presentation Applicability Editorial independence Mortensen et al.[16] 86.08% 83.33% 72.92% 88.83% 75% 66.67% 6 6 A Irani et al.[27] 91.67% 61.17% 93.79% 88.89% 41.67% 75% 5 6 B Chen[28] 91.67% 88.89% 90.63% 91.67% 33.33% 66.67% 5 6 B Table 2.
Quality evaluation results of clinical guidelines (n = 3).
-
Items Association[34] Surgery[35] 1. Is the source of the opinion clearly identified? Yes Yes 2. Does the source of opinion have standing in the field of expertise? Yes Yes 3. Are the interests of the relevant population the central focus of the opinion? Yes Yes 4. Is the stated position the result of an analytical process, and is there logic in the opinion expressed? Yes Yes 5. Is there reference to the extant literature? Yes Yes 6. Is any incongruence with the literature/sources logically defended? Yes Yes Table 3.
Quality evaluation results of expert consensus (n = 2).
-
Items Liu et al.[29] Ni et al.[30] Lee et al.[31] He et al.[32] Gao et al.[33] 1. Was true randomization used for assignment of participants to treatment groups? Yes Yes Yes Yes Yes 2. Was allocation to treatment groups concealed? Unclear Unclear Yes Unclear Unclear 3. Were treatment groups similar at the baseline? Yes Yes Yes Yes Yes 4. Were participants blind to treatment assignment? Unclear Unclear Unclear Unclear Unclear 5. Were those delivering the treatment blind to treatment assignment? Unclear Unclear No Unclear Unclear 6. Were treatment groups treated identically other than the intervention of interest? Yes Yes Yes Yes Unclear 7. Were outcome assessors blind to treatment assignment? Unclear Unclear Yes Unclear Unclear 8. Were outcomes measured in the same way for treatment groups? Yes Yes Yes Yes Yes 9. Were outcomes measured in a reliable way? Yes Yes Yes Yes Yes 10. Was follow-up complete and, if not, were differences between groups in terms of their follow-up adequately described and analyzed? Yes Yes Yes Yes Yes 11. Were participants analyzed in the groups to which they were randomized? Yes Yes Yes Yes Yes 12. Was appropriate statistical analysis used? Yes Yes Yes Yes Yes 13. Was the trial design appropriate and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial? Yes Yes Yes Yes Yes Table 4.
Quality evaluation results of randomized controlled trials (n = 5).
-
Items Tian et al.[36] 1. Is the review question clearly and explicitly stated? Yes 2. Were the inclusion criteria appropriate for the review question? Yes 3. Was the search strategy appropriate? Yes 4. Were the sources and resources used to search for studies adequate? Yes 5. Were the criteria for appraising studies appropriate? Yes 6. Was critical appraisal conducted by two or more reviewers independently? Yes 7. Were there methods to minimize errors in data extraction? Yes 8. Were the methods used to combine studies appropriate? Yes 9. Was the likelihood of publication bias assessed? Yes 10. Were recommendations for policy and/or practice supported by the reported data? Yes 11. Were the specific directives for new research appropriate? Yes Table 5.
Quality evaluation results of systematic review (n = 1).
-
Items Hu et al.[37] 1. Is it clear in the study what is the 'cause' and what is the 'effect' (i.e., there is no confusion about which variable comes first)? Yes 2. Were the participants included in any comparisons similar? Yes 3. Were the participants included in any comparisons receiving similar treatment/care, other than the exposure or intervention of interest? Yes 4. Was there a control group? Yes 5. Were there multiple measurements of the outcome both pre, and post the intervention/exposure? Yes 6. Was follow up complete and if not, were differences between groups in terms of their follow up adequately described and analyzed? Yes 7. Were the outcomes of participants included in any comparisons measured in the same way? Yes 8. Were outcomes measured in a reliable way? Yes 9. Was appropriate statistical analysis used? Yes Table 6.
Quality evaluation results of quasi-experimental study (n = 1).
-
Category Content of evidence Evidence Level Recommendation grade Preoperative education 1. Nurses took the initiative to communicate with patients enthusiastically upon the patients' admission, and informed patients of relevant precautions through health manuals, videos, posters, and words, so as to make patients ready for the operation psychologically, with optimism and good mentality[33]. 1 A 2. For different patients, cards, multimedia, exhibition boards, and other forms were used to introduce the perioperative process of anesthesia, surgery, and postoperative treatment, so as to relieve their anxiety, fear, and tension, making patients aware of their important role in this plan, and obtain the understanding and cooperation of patients and their families, including early postoperative feeding and early ambulation[28]. 5 A 3. Health care workers should introduce the anesthesia and operation process to patients and their families in detail by oral or written form before the operation. Inform the purpose and main items of the ERAS program to relieve patients ' tension and anxiety. Strive for the understanding and cooperation of patients and their families to promote rapid postoperative recovery[34,35]. 5 A Postoperative pain management 4. The postoperative pain intensity in patients was evaluated using either the Visual Analog Scale (VAS) or the Numerical Rating Scale (NRS)[31,33]. 1 A 5. If the pain score was less than 3, distract the patient's attention by chatting, listening to music, cold compress, hot compress, and other forms to relieve the pain. If the pain score was greater than 3, followed the doctor's advice to give analgesic treatment. For patients with a pain score of 7 or higher, 50 µg of IV fentanyl was administered as the first-line rescue analgesic[31,33]. 1 B 6. Multimodal analgesia is recommended. The important principle of analgesia is that non-steroidal anti-inflammatory drugs (NSAIDs) are the basic drugs for postoperative analgesia, and the application of opioids should be minimized[34,35]. 5 B 7. For patients undergoing laparoscopic gastric surgery, transversus abdominis plane nerve block and local infiltration of incision can be selected for analgesia[28]. 5 B Postoperative drainage tube management 8. No routine use of nasogastric tube during operation. If necessary, it should be retained during operation and removed within 24 h after operation[28,34,35]. 5 B 9. No routine indwelling intra-abdominal drain is required. After total gastrectomy and proximal gastrectomy, intra-abdominal drains can be retained while in other cases they should be removed 2−3 d after the operation[28]. 1 B 10. No special case, the urinary catheter should be removed 1−2 d after gastric surgery[16,28,31,34−36]. 5 B Pre-mobilization evaluation 11. If the vital signs are stable, the patients should get out of bed within 24 h after laparoscopic surgery[30,32]. 1 A 12.In the absence of nausea, dizziness, active bleeding, or unbearable incisional pain, the patient may be assisted to stand beside the bed for 5−10 min. Once no symptoms of orthostatic intolerance (including dizziness, palpitations, and blurred vision) are present, the patient may ambulate alongside the bed with assistance from a nurse or family member[29,33]. 1 A 13. If the pain score was less than 3 points, guide the patient to get out of bed correctly to protect the wound[30,37]. 1 A Early postoperative bed activity 14. After regaining consciousness postoperatively, patients may assume a semi-recumbent position or engage in appropriate in-bed activity; supine positioning without a pillow for 6 h is not required[28,34]. 5 A 15. After regaining consciousness from anesthesia, the patient is encouraged to mobilize in bed, and reposition every 2 h[30,32]. 1 A 16. Within 2 h after the operation, the abdominal belt was applied and the heel was raised by 15~20° with a small pillow. After the anesthesia, fully awake, and with normal vital signs, the head of the bed was raised by 30~45°. Assist the patient to carry out passive activities of both lower limbs. The massage included lower limb muscle massage, 3~5 min on each side, from the distal to the proximal massage, 3 times a day. Passive flexion and extension, internal and external rotation of ankle joint were performed, 15−20 times in each group, 3 groups per day[29]. 1 A 17. Two to 4 h after operation, patients were guided and assisted in abdominal breathing and lip contraction breathing[29]. 1 A 18. Four to 6 h after the operation, the head of the bed was raised by 45~60°, and the patient was assisted to turn over twice. Guide the patient to perform active muscle contraction and joint activities on the bed[29]. 1 B 19. Six to 12 h after operation, no fatigue or mild fatigue, and no active bleeding, the head of bed was raised to 90° sitting position for 3 min. If there is no obvious discomfort, assist to complete the bed-to-sit-up, three times. The sitting time was 10, 15, and 20 min respectively[29,30]. 1 B Early postoperative off-bed mobilization 20. On the day of surgery, the patients were allowed to sit on the edge of the bed and move if they desired[31]. 1 A 21. One day after operation, the patients began to get out of bed. Early and scheduled mobilization[16,28,34−36]. 1 A 22. One day after operation, the patient was allowed to get out of bed and move around for 1 to 2 h. Subsequently, they were allowed to get out of bed and move around for 4 to 6 h each day[28,30]. 1 B 23. The sequence of activities is: sitting up beside the bed for 3 min, standing beside the bed for 3 min, walking with support of the bed, and then walking away from the bed[30,37]. 1 A Early postoperative off-bed mobilization 24. Two days after operation, the patients were assisted to move in the corridor area of the ward[29,37]. 1 B 25. The walking distance was 25 to 50 m on the first day after operation, and gradually increased to 50 to 100 m when discharged[28,37]. 2 A 26. Daily check the patient 's activity completion. Establish a patient 's activity diary, and those who have not completed are urged to continue to complete[29]. 1 A Discharge criteria 27. (1) Tolerance of soft blended diet for 24 h, (2) safe ambulation until 600 m without assistance, (3) adequate pain control (NRS ≤ 3) with oral non-opioid analgesics, (4) the wound healed well, no infection, and (5) no abnormal physical findings or laboratory tests[27,28,31,34]. 1 B 28. There were no postoperative complications (e.g., anastomotic leak, bleeding, infection) and other basic diseases that needed to be treated. The patient could be discharged about 7 d after gastric surgery[28]. 5 B Table 7.
Evidence summary for EM after laparoscopic gastrectomy of gastric cancer.
Figures
(1)
Tables
(7)