-
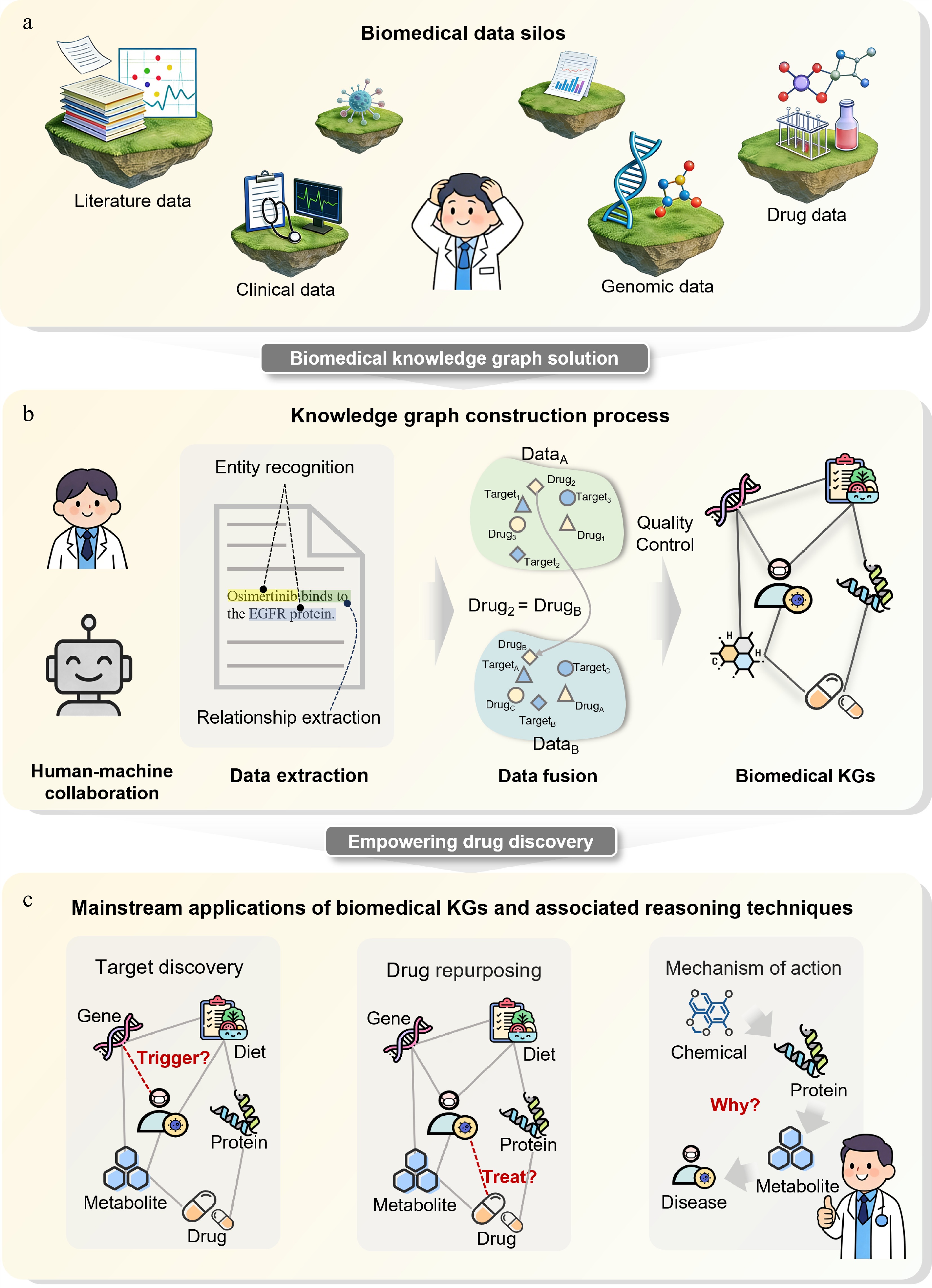
Figure 1.
Biomedical knowledge graphs break down data silos and promote drug discovery. (a) Biomedical data silos. Different data sources are isolated; real-world data, including literature, clinical records, genomic data, and drug-related information are heterogeneous and fragmented, hindering cross-semantic and cross-hierarchical integration. (b) Knowledge graph construction pipeline. Human-machine collaboration is used to extract entities and relationships from multi-source data, followed by integration and quality control to form a biomedical knowledge graph. (c) Major applications of biomedical knowledge graphs. Knowledge graph-based reasoning enables drug target discovery, drug repositioning, and mechanistic interpretation.
-
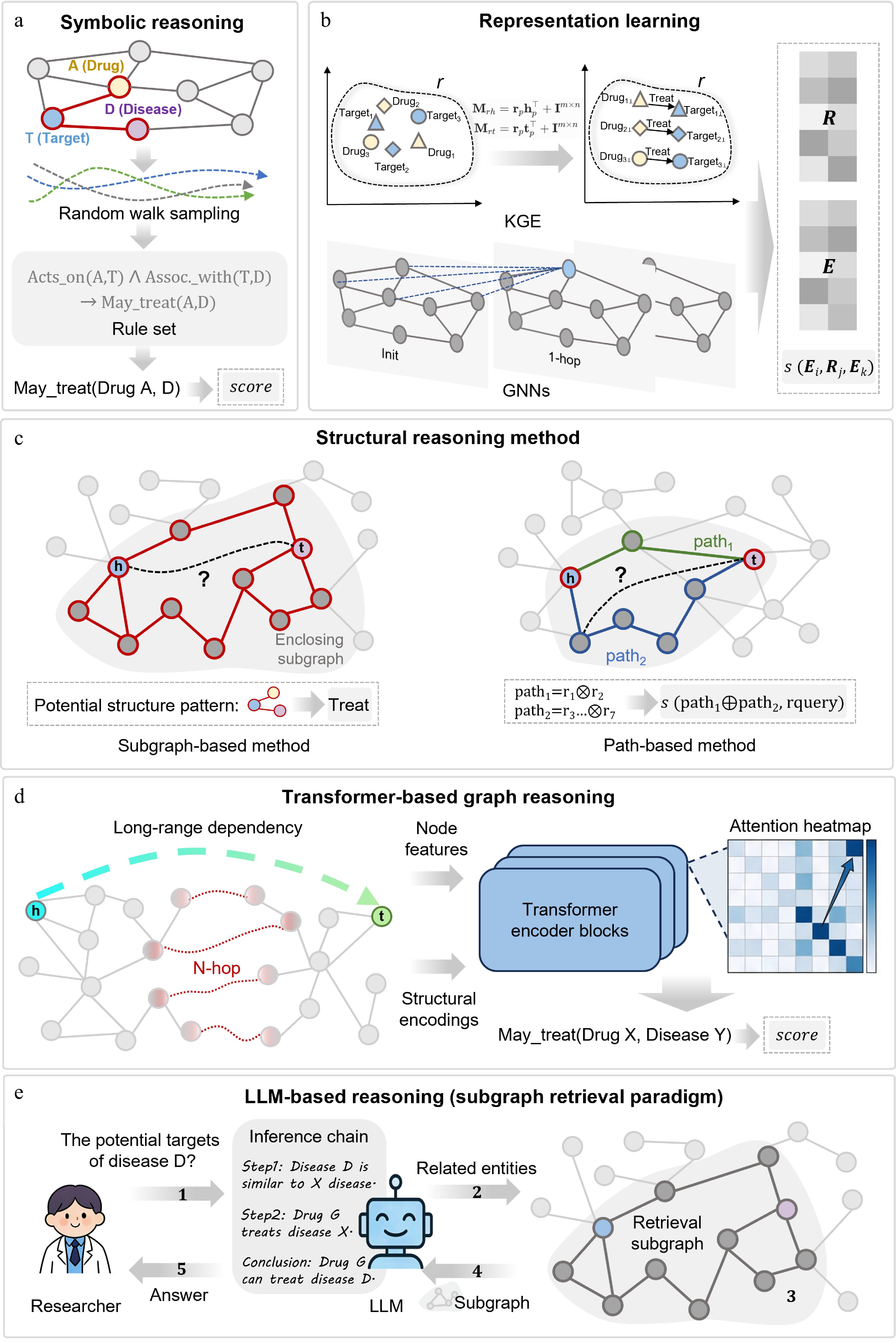
Figure 2.
Mainstream knowledge graph reasoning paradigms for target and drug discovery. (a) Symbolic reasoning. Performs inference via random walk sampling and first-order logic rules with high interpretability. (b) Representation learning. Maps entities and relations to low-dimensional vector spaces via KGE or GNNs and scores triples. (c) Path and structural reasoning. Infers links by mining enclosing subgraphs or multi-hop path patterns. (d) Transformer-based graph reasoning. Integrates node features and structural encoding into self-attention to capture long-range dependencies. (e) LLM-KG integrated reasoning. Retrieves structured subgraphs as context to guide LLMs for traceable logical inference. Structure-derived features such as pockets, residues, conformational states, variants, and ligand poses can serve as multimodal evidence layers across these paradigms.
-
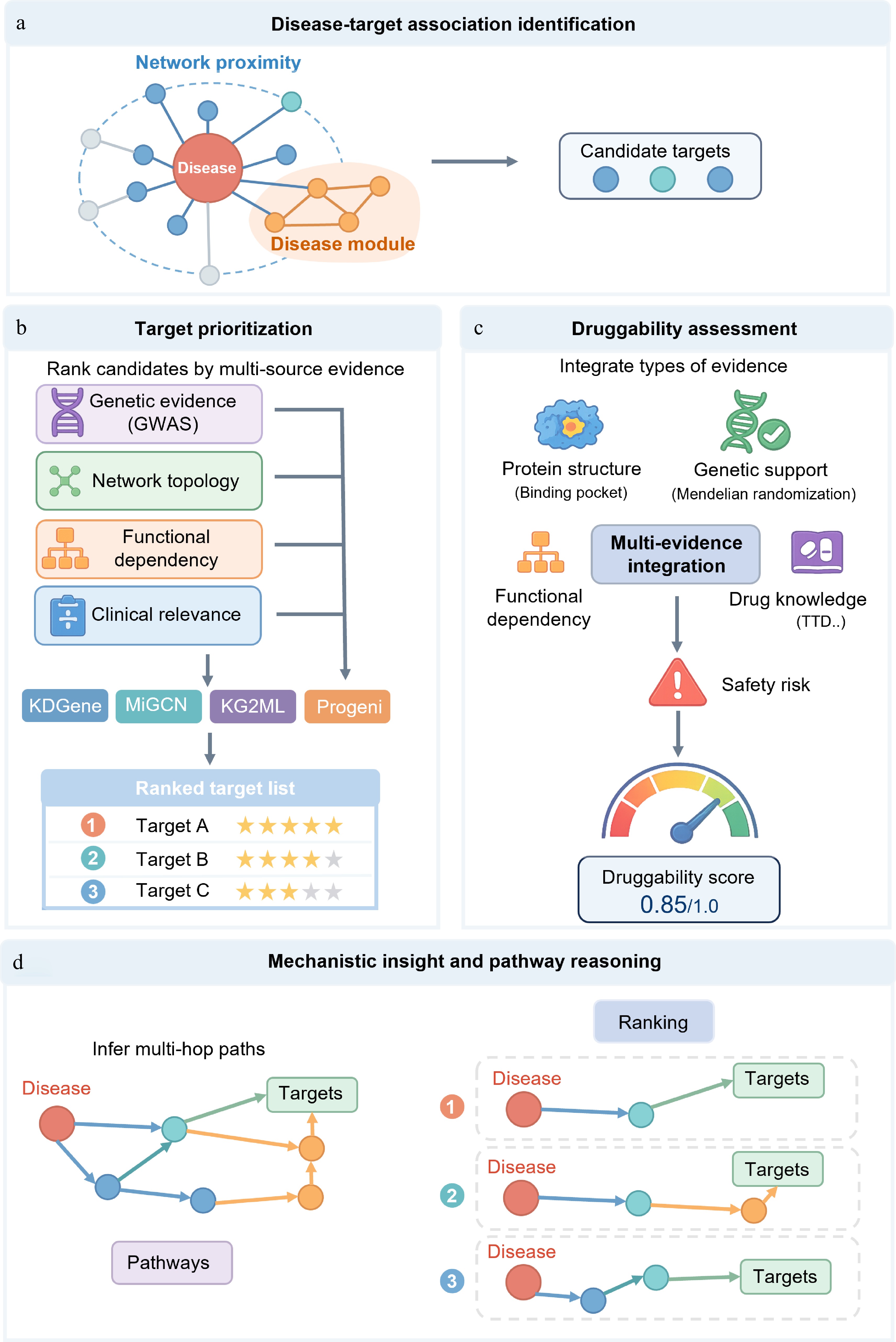
Figure 3.
A knowledge graph-based framework for disease-related target discovery, prioritization, druggability assessment, and mechanism analysis. (a) Identification of disease-related targets. Candidate targets associated with disease-related molecules are identified using network proximity, disease module expansion, and multi-relational knowledge graph representation learning. (b) Target prioritization. Candidate targets are ranked by integrating genetic evidence, network topology, functional dependencies, and clinical relevance. (c) Druggability assessment. The development potential of targets is evaluated by combining structural suitability, genetic support, functional networks, existing drug knowledge, and safety risks. (d) Mechanism elucidation and pathway inference. Infer and rank multi-hop pathways connecting diseases to candidate targets within the context of disease-related networks and pathways to reveal potential molecular mechanisms.
-
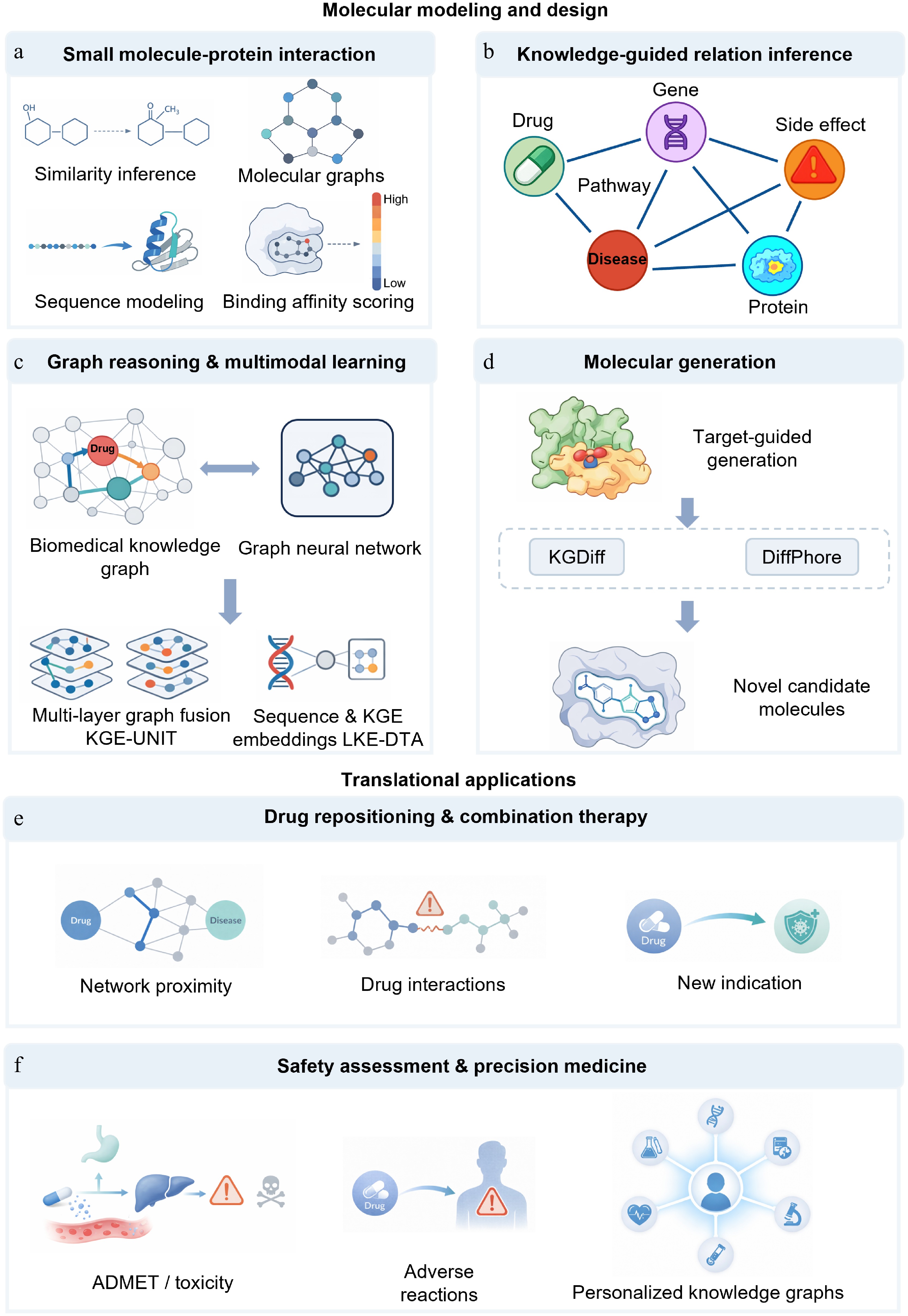
Figure 4.
Knowledge graph-based prediction of small-molecule-target interactions, molecular design, and translational applications. (a) Prediction of small-molecule–protein interactions. This has evolved from predictions based on chemical similarity and ligand-protein pairs to deep learning-based affinity prediction using molecular graph and protein sequence features. (b) Knowledge-guided relationship inference. Integrating heterogeneous entities such as drugs, proteins, diseases, pathways, genes, and side effects into a knowledge graph enables models to shift from local pairwise judgments to relationship inference within a biomedical context. (c) Graph reasoning and multimodal learning. With the introduction of graph reasoning, multi-task knowledge sharing, and multimodal representation, drug-target identification has evolved from simple relationship completion to joint modeling within complex biological contexts. (d) Molecular generation. Knowledge graphs are not only used for candidate screening but also provide conditional guidance for molecular generation and lead optimization, shifting design from rule-driven to information-driven approaches. (e) Drug repurposing and combination therapy. Knowledge graphs support drug reuse, synergistic effect prediction, and drug interaction modeling, extending candidate discovery to system-level inference based on multi-source evidence and contextual constraints. (f) Safety assessment and precision medicine. Knowledge graphs can integrate ADMET, toxicity, adverse reactions, and patient multimodal data for safety risk assessment and precision medicine analysis.
-
Dataset/benchmark Model Paradigm MRR Hits@1 Hits@10 Hits@100 FB15k-237[82]: general
multi-relational KGC benchmarkNeural-LP[51] Symbolic reasoning 0.237 0.173 0.361 NR TransE[35] Representation learning 0.312 0.212 0.51 NR RotatE[55] 0.338 0.241 0.533 NR TuckER[83] 0.358 0.266 0.544 NR CompGCN[84] Path and structure-aware reasoning 0.355 0.264 0.535 NR NBFNet[61] 0.415 0.321 0.599 NR HittER[85] Transformer-based graph reasoning 0.373 0.279 0.558 NR KnowFormer[86] 0.43 0.343 0.608 NR SimKGC[87] Hybrid KG-LLM reasoning 0.338 0.252 0.511 NR SAT[88] 0.354 0.319 NR NR SRP-KGC[89] 0.431 0.353 0.585 NR Hetionet[90]: biomedical
KG filtered tail predictionAnyBURL[50] Symbolic reasoning 0.322 0.229 0.553 NR Noisy-or rule aggregation[91] 0.472 0.377 0.642 NR TransE[35] Representation learning 0.205 0.099 0.444 NR ComplEx[54] 0.25 0.152 0.47 NR RotatE[55] 0.257 0.185 0.403 NR CompGCN[84] Path and structure-aware reasoning 0.292 0.172 0.543 NR MINERVA[92] 0.37 0.264 0.593 NR PoLo[93] 0.43 0.337 0.641 NR HittERnc[85] Transformer-based graph reasoning 0.453 0.316 0.74 NR ogbl-ppa[81]: large-scale biological protein
association link
predictionCommon neighbor[94] Symbolic reasoning NR NR NR 0.2765 Resource allocation[95] NR NR NR 0.4933 Matrix factorization[81] Representation learning NR NR NR 0.3229 SEAL[96] Path and structure-aware reasoning NR NR NR 0.488 NGNN + SEAL[97] NR NR NR 0.5971 Neural common neighbor[98] NR NR NR 0.6119 GraphGPT[67] Transformer-based graph reasoning NR NR NR 0.7655 Table 1.
Representative quantitative benchmarks for knowledge graph reasoning paradigms.
-
Reasoning paradigm Core methodology Key applications in drug discovery Critical comparison in biomedical scenarios Symbolic reasoning Logical rule learning, differentiable rule reasoning, random walk path sampling Target identification, mechanism of action
analysis, high-confidence association predictionThese methods are most useful when transparent evidence chains and expert-auditable hypotheses are required. They can be competitive on biomedical link-prediction benchmarks, but their coverage may be limited in sparse or noisy KGs, and rule search can become expensive in large heterogeneous graphs. Representation learning Knowledge graph embedding (KGE), relation-aware message passing, attention-based feature aggregation Drug-target interaction prediction, disease-target association identification, molecular property
predictionThese models scale well to large biomedical KGs and provide strong graph-fitting baselines for candidate ranking. Their main limitations are limited mechanistic interpretability, sensitivity to negative sampling and random splits, possible hub-node or literature-density bias, and over-smoothing in deep GNNs. Path and structure-aware reasoning Explicit path enumeration, reinforcement learning for path search, subgraph inductive reasoning, neural implicit path modeling Multi-hop mechanistic inference, cold-start target/molecule prediction, drug repurposing path
miningThese models are attractive when the task requires interpretable multi-hop evidence or generalization to sparsely annotated diseases and drugs. Their reliability depends strongly on KG completeness, path quality, disease-split design and candidate-universe definition. Transformer-based graph reasoning Structural encoding + self-attention, spectral feature embedding, local convolution + global transformer, linear-complexity state space models Long-range target regulation prediction, cross-pathway association inference,
large-scale KG reasoningThese models are conceptually suitable when distant graph context, cross-pathway information or multi-source molecular features are expected to influence prediction. However, biomedical benchmark evidence is often task-specific rather than evaluated under a shared KG benchmark protocol, and performance may be inflated when similar drugs, homologous proteins or related diseases appear across train and test splits. Hybrid KG-LLM reasoning Retrieval-augmented generation, subgraph prompting, multi-agent collaborative reasoning, chain-of-thought graph reasoning Complex mechanism analysis, low-resource drug discovery, interpretable clinical translational reasoning These methods are promising for natural-language evidence synthesis and explanation-rich biomedical reasoning. However, their evaluation should include evidence of faithfulness, path validity, calibration, prompt robustness, and hallucination control rather than predictive accuracy alone. Table 2.
Practical comparison of KGR paradigms for target and drug discovery.
Figures
(4)
Tables
(2)