-
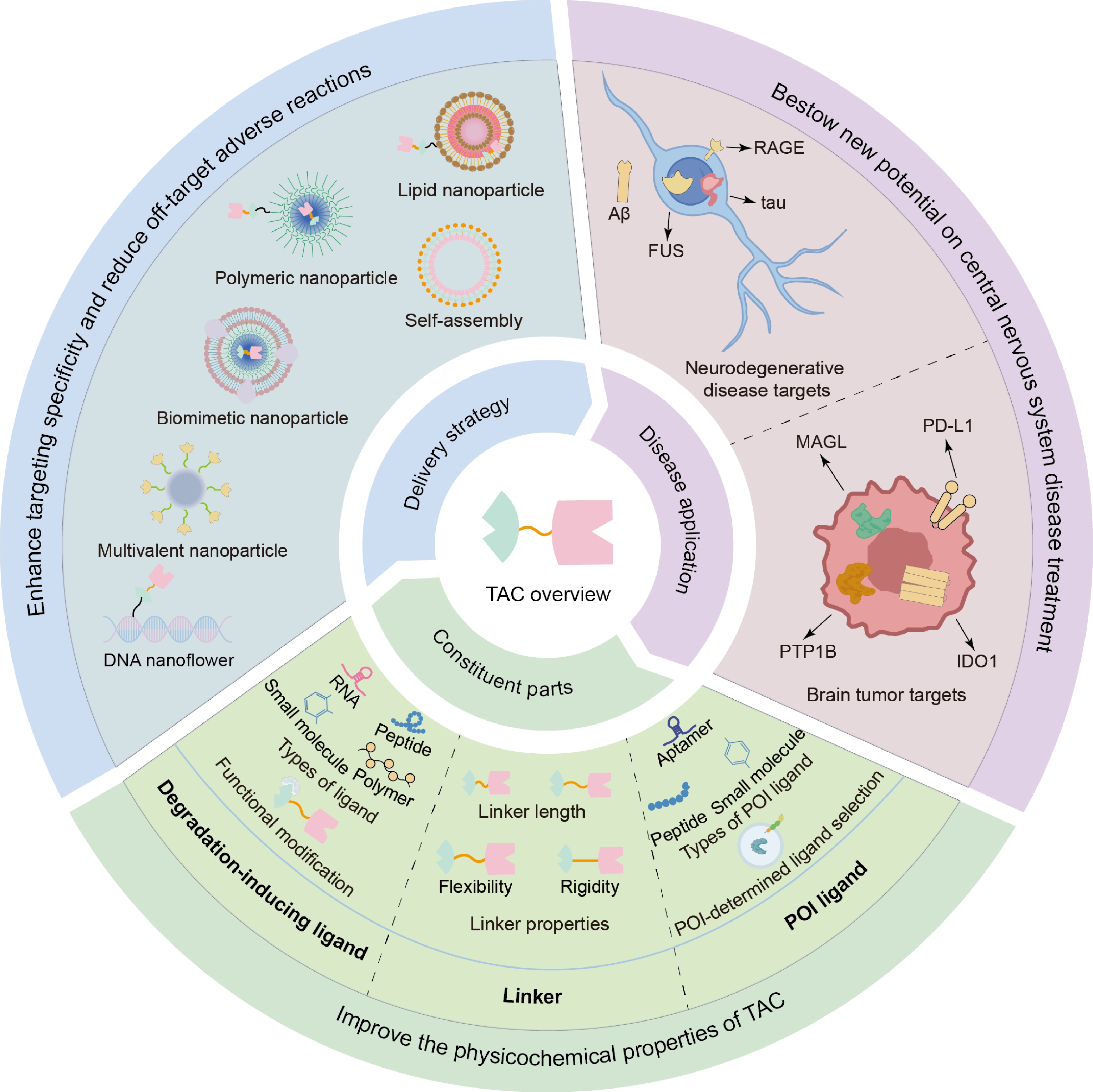
Figure 1.
Schematic descriptions of TAC technology, from molecular components, therapeutic applications, to delivery strategies.
-
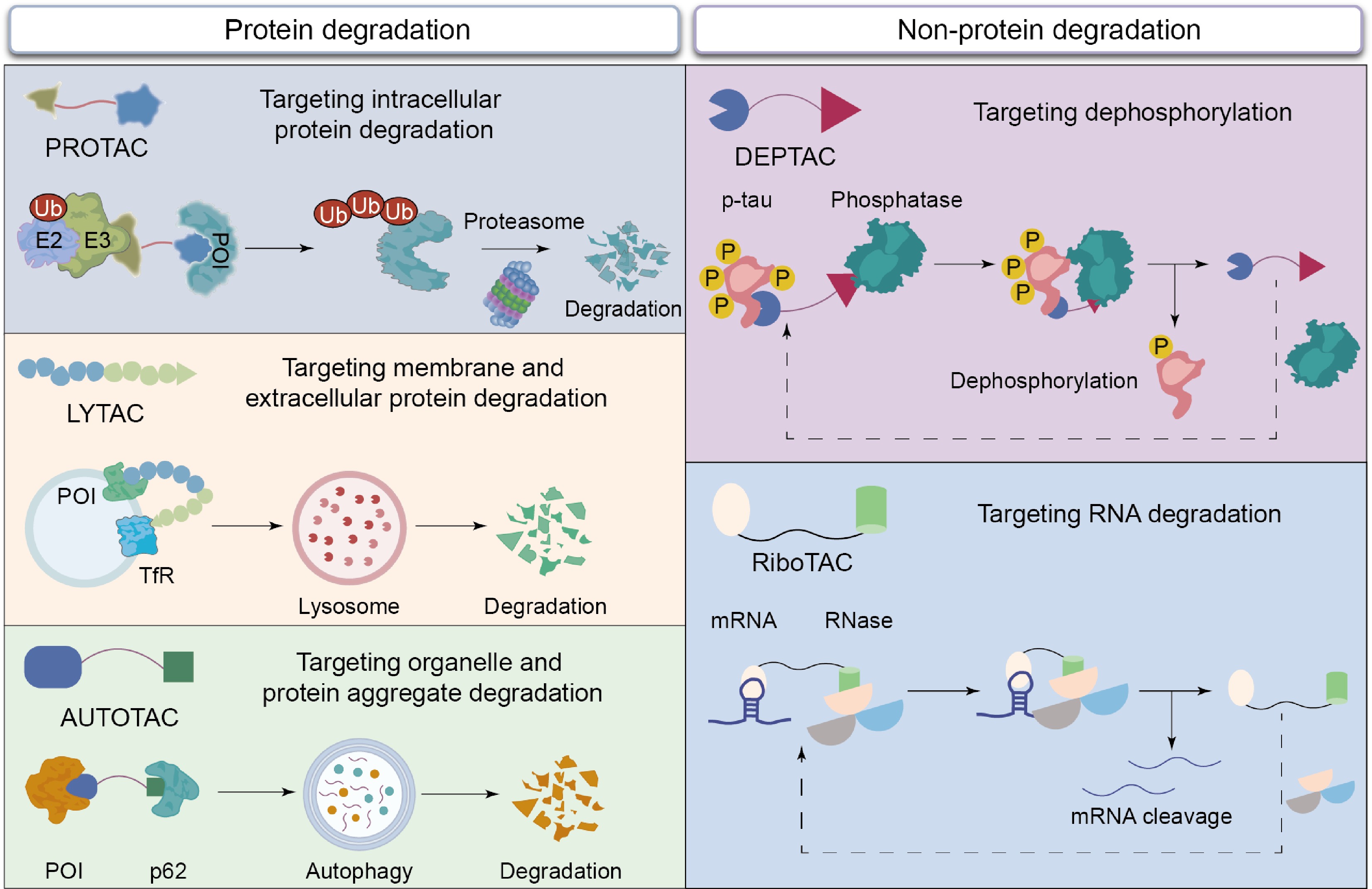
Figure 2.
The action mechanisms of different TAC molecules, including PROTAC, LYTAC, AUTOTAC, RiboTAC, and DEPTAC, for targeting degradation of intracellular protein, membrane and extracellular protein, protein aggregate, RNA, and dephosphorylation.
-
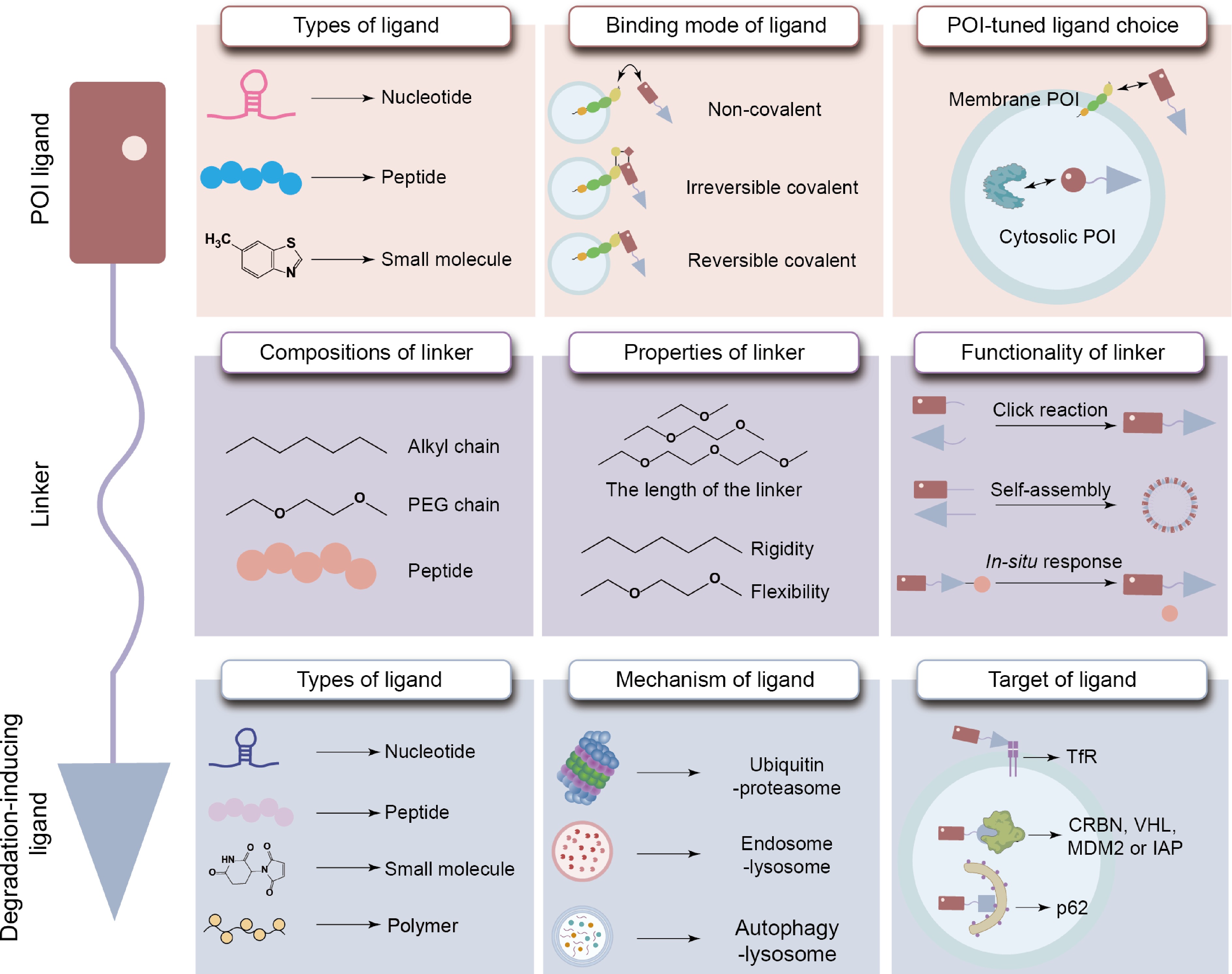
Figure 3.
Properties of the POI ligand, degradation-inducing ligand, and linker within TAC molecules.
-
-
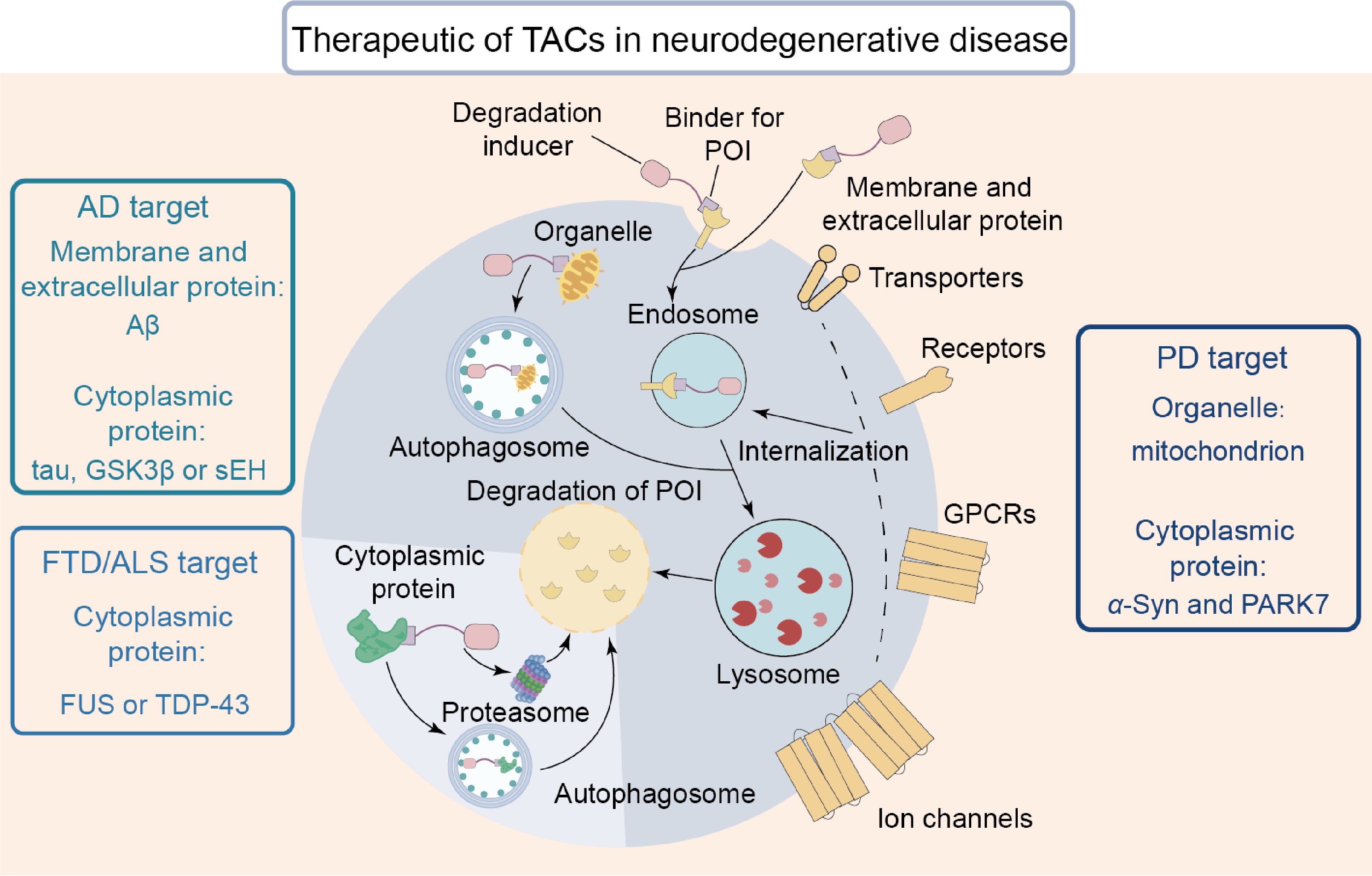
Figure 5.
By inducing the degradation of POIs, TAC serves as an effective approach for treating NDs. These POIs include membrane proteins, cytoplasmic aggregates, and damaged organelles.
-
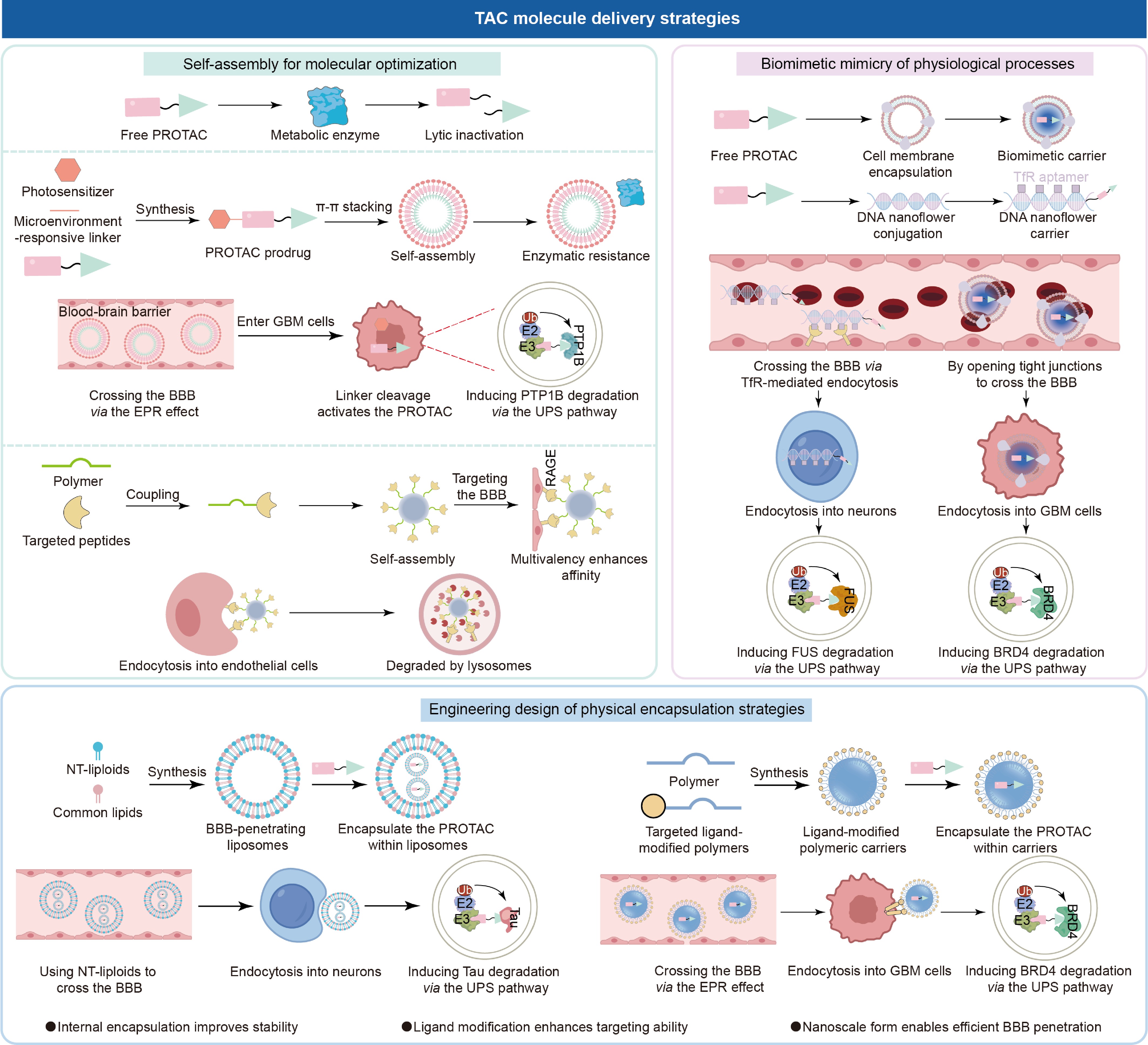
Figure 6.
Nano-delivery carriers offer a solution to the questions of TAC therapy. These carriers use self-assembly methods to improve molecular properties, employ biomimetic materials to mimic physiological processes, and improve therapeutic efficacy through engineered design.
-
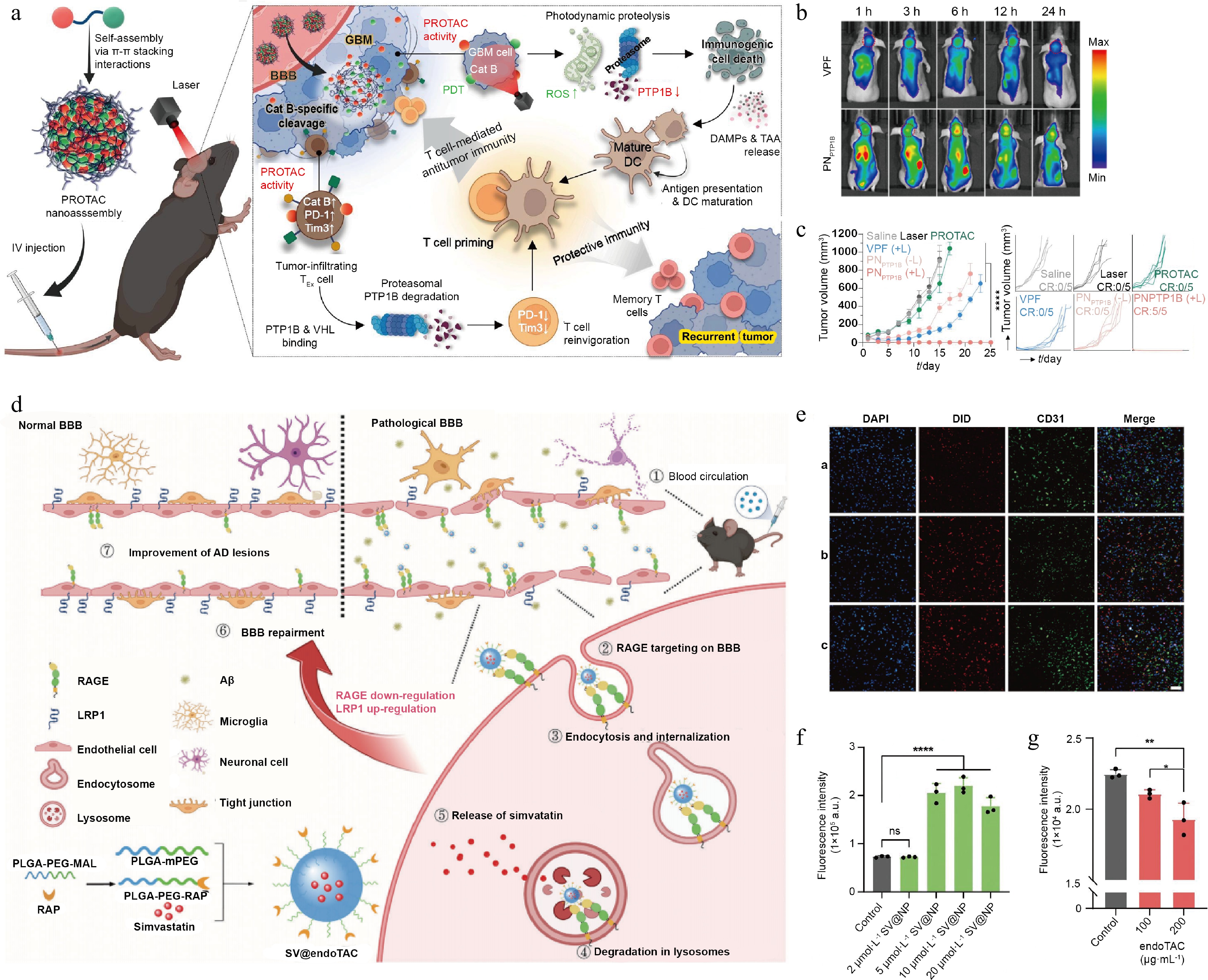
Figure 7.
Characterization of TAC-based self-assembling nanoplatforms and their performance. (a) Design strategy of endoTAC and its mechanistic role in AD therapy. (b) Intracellular distribution of nanoparticles in brain vascular endothelial cells. (c) Flow cytometric analysis of FITC-Aβ uptake in bEnd.3 cells following 24-h co-incubation with SV@NP. (d) Flow cytometry was used to analyze FITC-Aβ uptake in RAGE-overexpressing bEnd.3 cells after 24 h of co-culture with endoTAC. Reprinted with permission from Ref.[5]. Copyright 2024 Wiley.
-
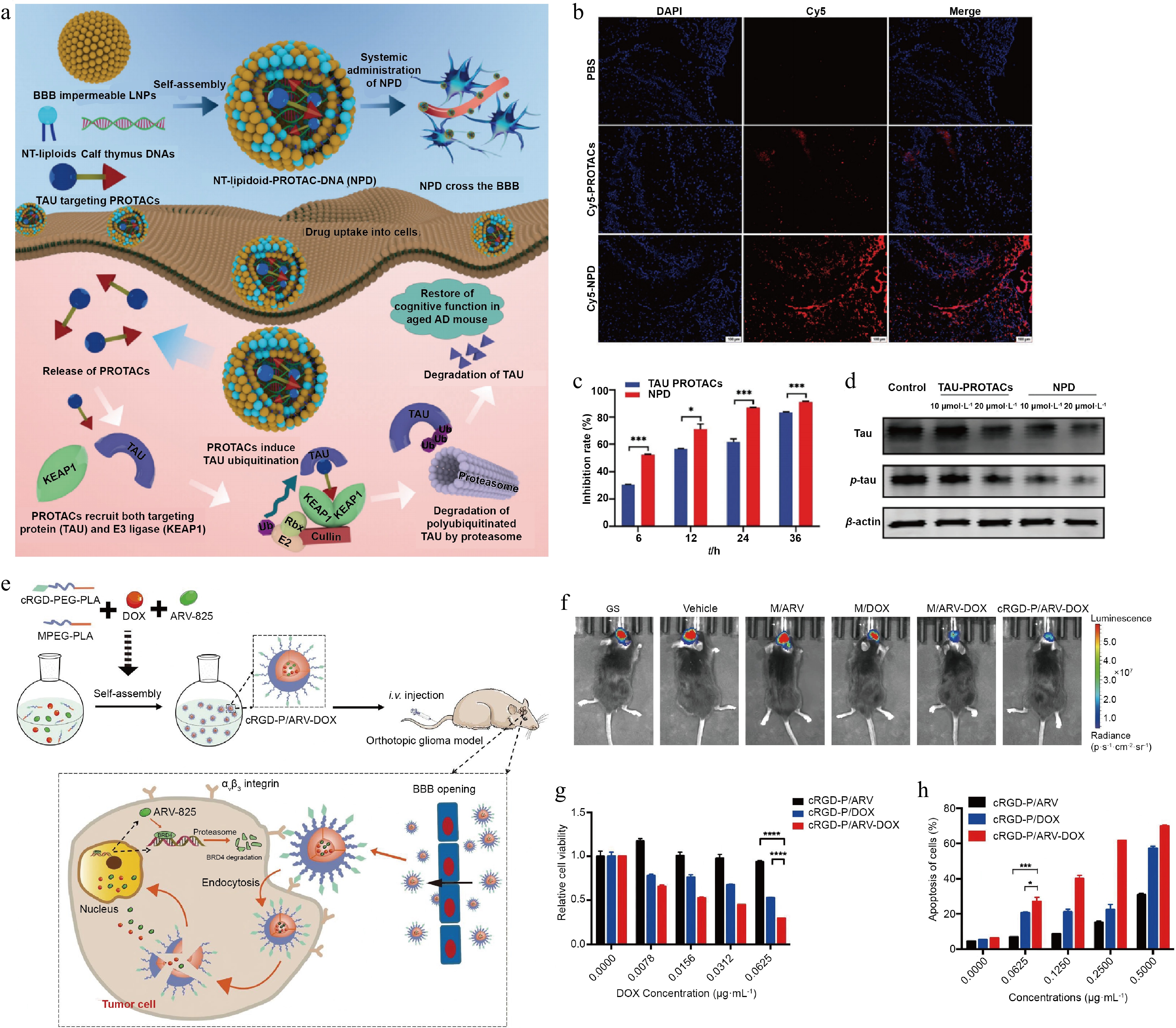
Figure 8.
Design and experimental confirmation of TAC delivery via liposomes and polymer carriers. (a) Design of the liposome-based delivery platform and its mechanism of action in AD treatment. (b) Representative fluorescence images of coronal brain sections from C57 mice, showing Cy5-labeled PROTAC (red) and nuclear staining (blue). (c) Quantitative flow cytometric analysis of fluorescence intensity in TAU-EGFP-overexpressing N2a cells following PROTAC treatment at specified time points. (d) Western blot analysis was performed to assess the extent of tau protein degradation. Reprinted with permission from Ref.[119]. Copyright 2024 Wiley. (e) Design of the polymer delivery carrier and its mechanism of action. (f) Representative in vivo bioluminescence imaging of tumor-bearing mice after treatment. (g) Cytotoxicity of cRGD-P/ARV, cRGD-P/DOX, and cRGD-P/ARV-DOX in GL261 cells after 24-h incubation was assessed using the MTT assay at concentrations ranging from 0 to 0.0625 μg·mL−1. (h) Flow cytometric analysis of apoptosis in GL261 cells using Annexin V/PI double staining. Reprinted with permission from Ref.[120]. Copyright 2022 Elsevier.
-
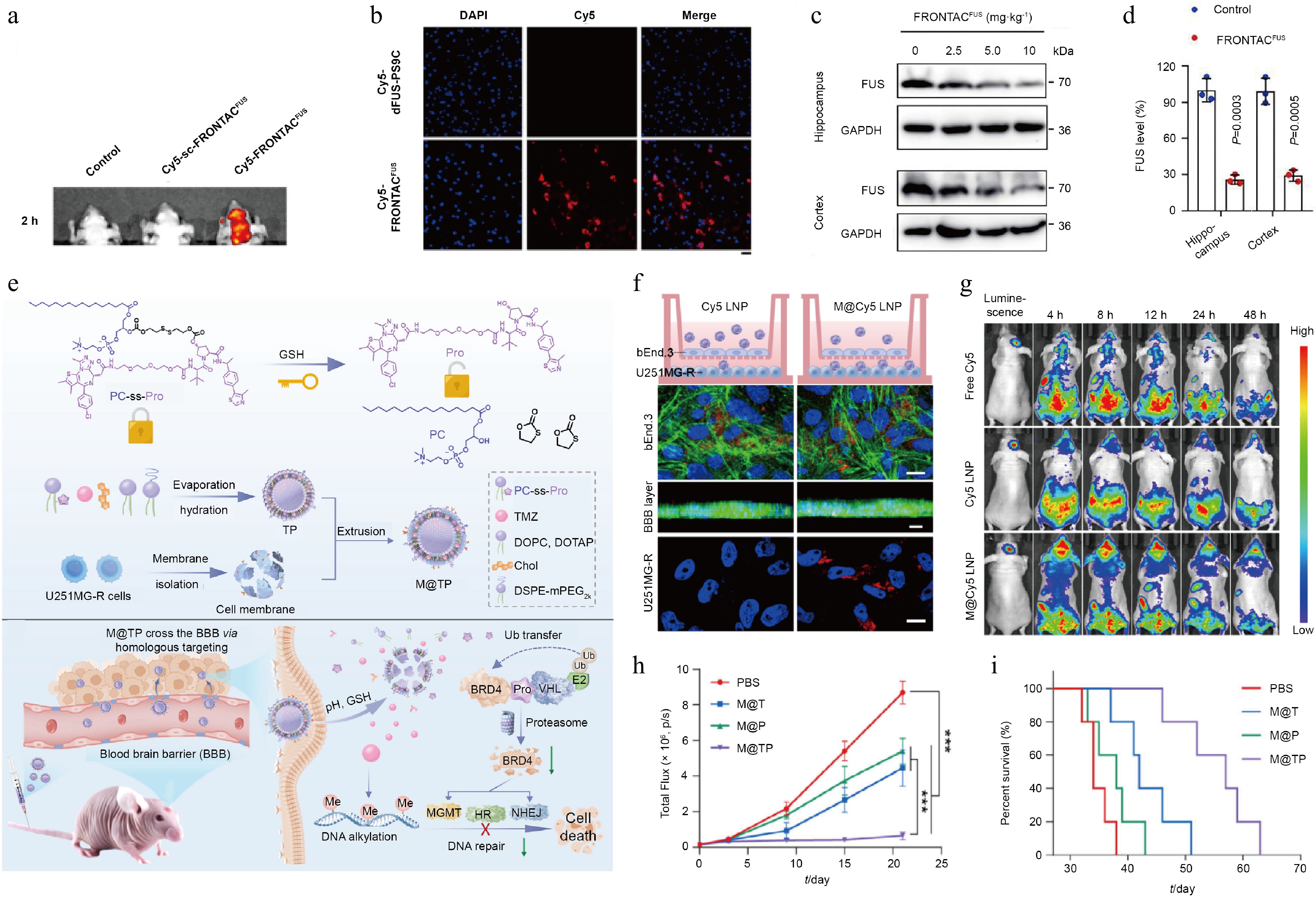
Figure 9.
Characterization of TAC-based biomimetic carrier delivery platforms and their experimental confirmation. (a) In vivo and ex vivo fluorescence imaging of mice following tail vein injection of PBS, sc-FRONTACFUS, and FRONTACFUS. (b) Fluorescence imaging of brain tissue sections from mice administered Cy5-labeled dFUS-PS9C or Cy5-labeled FRONTACFUS via tail vein. (c) Immunoblot analysis of FUS level in hippocampal and cortical tissues from mice administered escalating doses of FRONTACFUS via tail vein injection. (d) Quantitative comparison of Western blot data analyzing differences in FUS degradation in hippocampal and cortical tissues following tail vein injection of NF control vs 10 mg·kg−1 FRONTACFUS. Reprinted with permission from Ref.[92]. Copyright 2025 Springer Nature. (e) Mechanism of action of the TAC biomimetic cell membrane delivery platform. (f) In vitro evaluation of the BBB penetration capacity of Cy5 LNP and M@Cy5 LNP using the Transwell assay. (g) In vivo distribution of free Cy5, Cy5 LNP, and M@Cy5 LNP measured at specified time points following tail vein injection in mice with orthotopic U251MG glioma. (h) Quantitative analysis of tumor bioluminescence signals in each treatment group. (i) Kaplan–Meier survival analysis for mice in each treatment group. Reprinted with permission from Ref.[129]. Copyright 2025 Wiley.
-
Types of TAC Characteristics Key challenges in the application of CNS diseases Future design strategies PROTAC Inducing the efficient degradation of intracellular soluble POI Proteasome pore size is only 13 Å, restricting entry of protein aggregates[46];
Neuronal proteasome impairment in AD affects UPS pathway activity[47];
Neurons express lower VHL and related E3 ligases than peripheral tissues, increasing susceptibility to off-target toxicityIntervening on protein monomers or oligomers in the early stages of the disease;
Incorporate additional proteasome repair elements during design to restore proteasome activity;
Development of PROTACs targeting E3 ligases specifically expressed in neurons, such as TRIM28LYTAC Inducing lysosomal degradation of membrane-bound and extracellular POIs via the endocytic system Structures frequently contain antibodies or glycopeptides, readily causing strong immune responses[45];
Impaired lysosomal acidification in AD severely impairs protein degradation efficiency[48];
Lysosomal transport receptors such as CI-M6PR are widely expressed in various tissues, posing a risk of nonspecific uptake[49]Replace antibodies or peptide ligands with small chemical molecules to mitigate immune responses;
Co-delivery with drugs used to treat lysosomal acidification disorders;
Identification of endocytic receptors overexpressed in CNS lesion sites via single-cell sequencing and subsequent design of targeting ligandsAUTOTAC Driving the autophagic degradation of cytoplasmic protein aggregates It may affect the cellular autophagy pathway, leading to excessive autophagy and damaging healthy neurons[45];
p62 levels are upregulated or depleted under pathological conditions in ND[50]Administer the drug in pulses to prevent excessive autophagy;
Design of an autophagy ligand that is independent of p62 levelsDEPTAC Using a phosphatase to promote the dephosphorylation of the overphosphorylated POI PP2A expression is downregulated in the affected brain regions[51];
It can only remove the phosphorylated groups from the toxic protein, but cannot eliminate the protein backboneDesigning ligands to recruit phosphatases specifically enriched in neurons;
Combining dephosphorylation and protein degradation functions to develop DEPTAC-degradation chimerasRiboTAC Eliminate POI at the source by using ribonuclease L to catalyze mRNA cleavage Widespread expression of RNA-binding proteins carries a high risk of off-target degradation By employing a bispecific antisense oligonucleotide approach, target specificity is further enhanced Abbreviation: CI-M6PR, cation-independent mannose-6-phosphate receptor. Table 1.
The characteristics and limitations of different TACs, as well as the challenges encountered when applying them to CNS disorders.
-
Degradation-induced targets TAC Clinical phases (date) POI targets Indications CRBN Dezandrodeg[53,54] III (2025, 3) AR Prostate cancer ARV-766[55] II (2025, 10) AR Prostate cancer KT-474[56,57] II (2023, 11) IRAK4 Atopic dermatitis, hidradenitis suppurativa BMS-986458[58] II (2023, 10) BCL6 Relapsed/refractory non-Hodgkin lymphoma, BCL Zelebrudomide[59] I (2021, 4) BTK
IKZF1
IKZF3BCL, MZL, WM, LPL/IC, FL, CLL, DLBCL, SMZL, MCL, SLL, central nervous system tumor Zaloblideg I (2024, 9) BCL6 NHL, AITL, BCL, DLBCL CFT8919[60] I (2025, 2) EGFR NSCLC UBE3 Vepdegestrant III (2023, 3) ESR1 Breast cancer, MBC, HR+/HER2- breast cancer ARD-266 I (2025, 9) AR CRPC ARV-102 I (2024, 2) LRRK2 PSP, Parkinson's disease, neurodegenerative disease TQB3019[61] I (2025, 1) BTK Advanced malignant cancer VHL PRT3789[52,62] II (2025, 3) SMARCA2 Advanced and metastatic solid tumor, esophageal cancer, NSCLC ASP4396[63] I (2024, 4) KRAS G12D Solid tumor ASP3082[64] I (2025, 4) KRAS G12D Solid tumor SQSTM1 ATC-202 I (2025, 4) TTR Familial amyloid polyneuropathy ATC-104 I (2024, 4) TDP-43 Amyotrophic lateral sclerosis Others (undisclosed) Catadegbrutinib[52,65,66] III (2025, 5) BTK B cell malignancy, NHL, MCL, Chronic spontaneous urticaria, relapsed cancer, refractory cancer, CLL, SLL, MZL, FL GT-20029 II (2024, 3) AR Alopecia, acne vulgaris PT0253 I (2024, 12) KRAS G12D Solid tumor AXT-1003[67] I (2024, 6) EZH2 Relapsed/refractory non-Hodgkin lymphoma, NHL, advanced solid tumor Abbreviations: ESR1, estrogen receptor 1; MBC, metastatic breast cancer; HR+/HER2- breast cancer, hormone receptor positive/human epidermal growth factor receptor 2 negative breast cancer; AR, androgen receptor; BTK, Bruton tyrosine kinase; NHL, non-Hodgkin lymphoma; MCL, mantle cell lymphoma; CLL, chronic lymphocytic leukemia; SLL, small lymphocytic lymphoma; MZL, marginal zone lymphoma; FL, follicular lymphoma; IRAK4, interleukin 1 receptor associated kinase 4; SMARCA2, SWI/SNF related, matrix associated, actin dependent regulator of chromatin, subfamily A, member 2; NSCLC, non-small cell lung cancer; BCL6, B-cell lymphoma 6 protein; BCL, B-cell lymphoma; CRPC, castration-resistant prostate cancer; IKZF1, IKAROS family zinc finger 1; IKZF3, IKAROS family zinc finger 3; WM, Waldenström macroglobulinemia; LPL/IC, lymphoplasmacytic lymphoma/immunocytoma; DLBCL, diffuse large B-cell lymphoma; SMZL, splenic marginal zone lymphoma; LRRK2, leucine-rich repeat kinase 2; PSP, progressive supranuclear palsy; AITL, angioimmunoblastic T-cell lymphoma; EGFR, epidermal growth factor receptor; EZH2, enhancer of zeste homolog 2; TTR, transthyretin; SQSTM1, sequestosome 1; TDP-43, TAR DNA-binding protein 43. Table 2.
TAC therapies in clinical disease treatment, with degradation-induced targets, candidate molecules, clinical phases, POI targets, and indications.
Figures
(9)
Tables
(2)