-
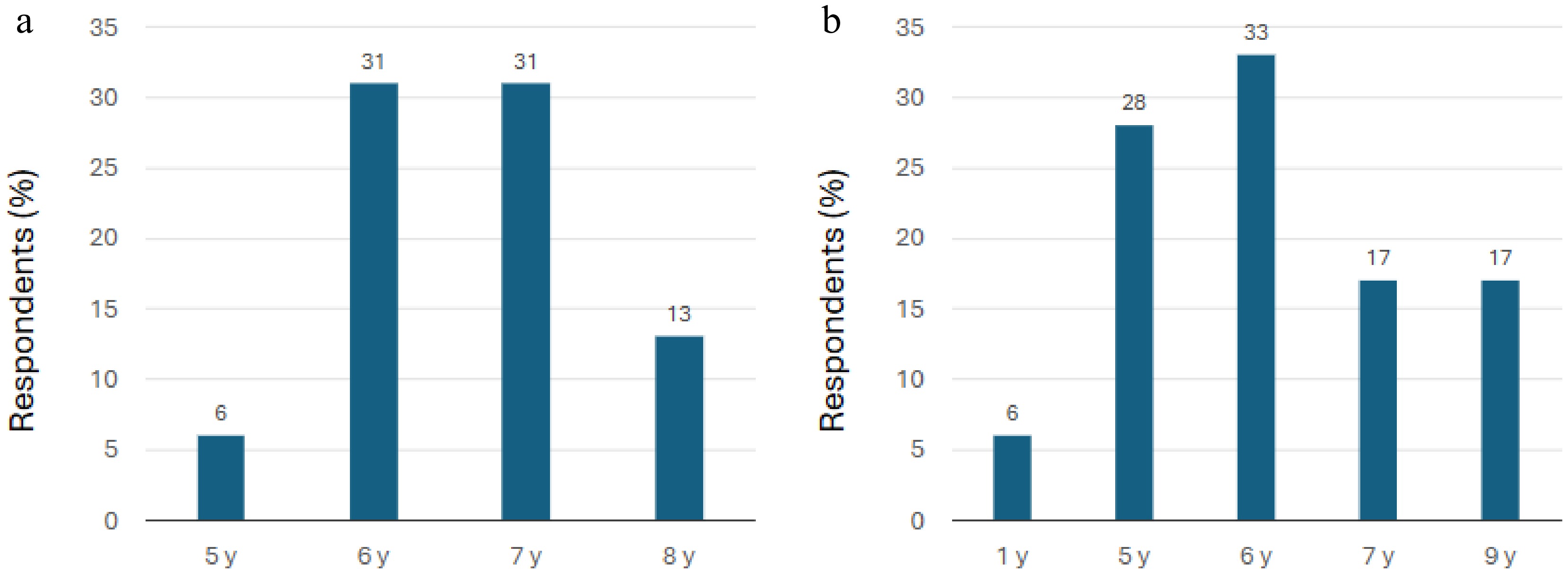
Figure 1.
Youngest ages at which ECPs participating in the survey prescribe myopia control contact lenses. (a) EECP group (n = 16). (b) GECP group (n = 18). Note: The x-axis values are only representative of the responses to the relevant question, which required free text responses (see Table 1) and not the selection of ages within a defined continuous age range. EECP, expert eye care professionals; GECP, general eye care professionals; y, years.
-
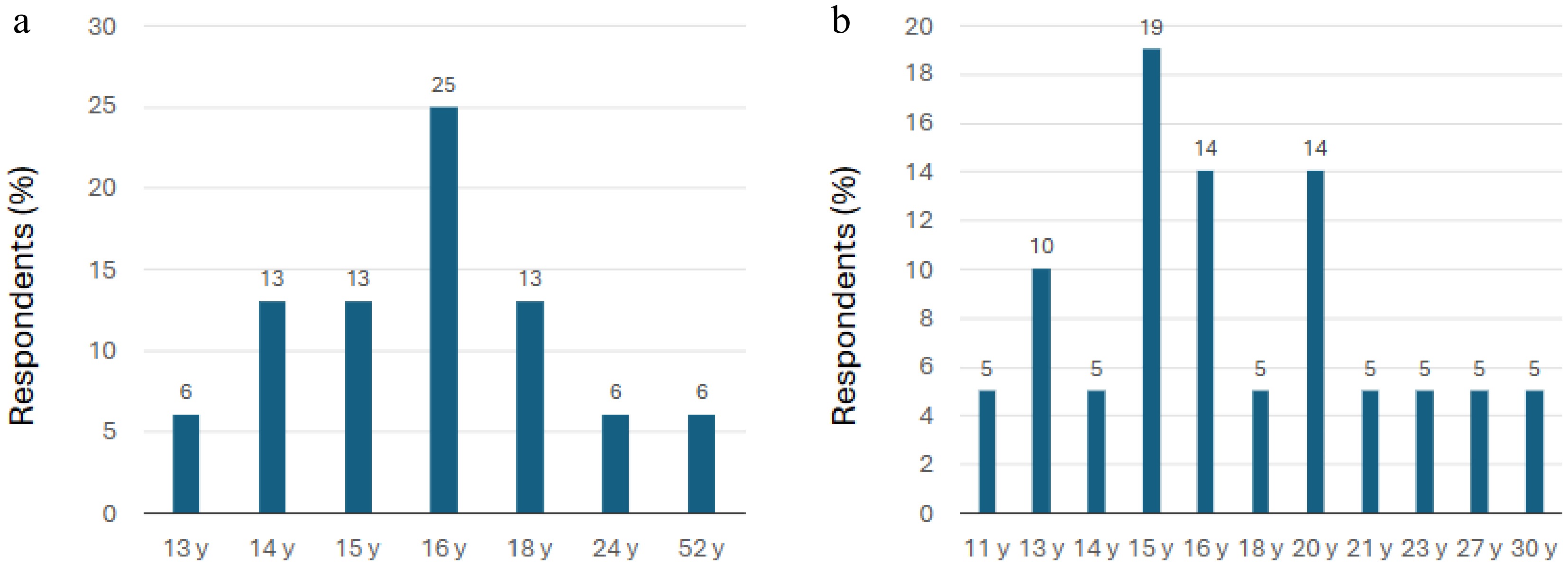
Figure 2.
Oldest ages at which ECPs participating in the survey prescribe myopia control contact lenses. (a) EECP group (n = 16). (b) GECP group (n = 18). Note: The x-axis values are only representative of the responses to the relevant question, which required free text responses (see Table 1) and not the selection of ages within a defined continuous age range. EECP, expert eye care professionals; GECP, general eye care professionals; y, year.
-
What is the youngest and oldest patient you have fitted with myopia control contact lenses? No answer options provided.
The respondents added their own responses.How do you fit your patients with myopia control contact lenses? • Soft contact lenses: Trial lens fit*
• Soft contact lenses: Dispensed according to the patient's refractive error
• Ortho-k: Trial lens fit
• Ortho-k: Empirical – manual calculation and dispensed according to the patient's topography and refractive errorƚ
• Ortho-k: Empirical – digital software calculating the parameters for first fit according to the topography and refractive errorǂWhat would you deem as an acceptable best-corrected visual acuity outcome for children using myopia control contact lenses? • 6/6 only
• 6/7.5 or better
• 6/9 or better
• 6/12 or betterWhat would you check in terms of fit assessment? (Please select all that apply.) • Soft contact lenses: Slit-lamp examination
• Soft contact lenses: Over-refraction
• Ortho-k: Slit-lamp examination
• Ortho-k: Fluorescein pattern evaluation
• Ortho-k: Over-refraction
• Ortho-k: Corneal topography
• Other (please specify whether this is for soft contact lenses and/or ortho-k)If you have selected soft contact lenses, please indicate what you would routinely check or assess. • Comfort
• Vision
• Centration and cornea coverage
• Edge alignment to conjunctiva
• Primary gaze post-blink movement
• Push-up test recoveryIf you have selected ortho-k lenses, please indicate what you would routinely check or assess. • Comfort
• Vision
• Fluorescein pattern evaluation with the lens onMonitoring soft contact lenses: What would be your follow-up regime for the first year and subsequent years in children using MCSCLs?
What are the parameters you use to monitor your patients with MCSCLs for myopia progression during follow-up visits?• First year: Axial length: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• First year: Refraction: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• Subsequent years: Axial length: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• Subsequent years: Refraction: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 yearMonitoring ortho-k lenses: What would be your follow-up regime for the first year and subsequent years in children using ortho-k lenses?
What are the parameters you use to monitor your patients with ortho-k lenses for myopia progression during follow-up visits?• First year: Axial length at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• First year: Refraction at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• Subsequent years: Axial length at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• Subsequent years: Refraction at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 yearFor children 9 years and below: What would you consider as an acceptable myopia control treatment effect, based on myopia's stability of refraction or over-refraction in 1 year? • Zero progression
• ≤ 0.50 D progression
• ≤ 0.75 D progression
• ≤ 1.00 D progression
• > 1.00 D progressionFor children 9 years and below: What would you consider as an acceptable myopia control treatment effect, based on myopia stability in terms of axial length in 1 year? • ≤ 0.05 mm increase
• ≤ 0.10 mm increase
• ≤ 0.20 mm increase
• ≤ 0.30 mm increase
• > 0.30 mm increaseFor children 10 years and above: What would you consider as an acceptable myopia control treatment effect, based on myopia stability of refraction/over-refraction in 1 year? • Zero progression
• ≤ 0.50 D progression
• ≤ 0.75 D progression
• ≤ 1.00 D progression
• > 1.00 D progressionFor children 10 years and above: What would you consider as an acceptable myopia control treatment effect, based on myopia stability of axial length in 1 year? • ≤ 0.05 mm increase
• ≤ 0.10 mm increase
• ≤ 0.20 mm increase
• ≤ 0.30 mm increase
• > 0.30 mm increaseCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to age. • Any age
• 12 years old and below
• 13–15 years old
• 15–18 years old
• Beyond 18 years oldCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to myopia stability of refraction/over-refraction. • Zero progression over 1 year
• ≤ 0.50 D progression over 1 year
• ≤ 0.75 D progression over 1 year
• ≤ 1.00 D progression over 1 year
• > 1.00 D progression over 1 yearCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to myopia stability of axial length. • ≤ 0.05 mm increase over 1 year
• ≤ 0.10 mm increase over 1 year
• ≤ 0.20 mm increase over 1 year
• ≤ 0.30 mm increase over 1 year
• > 0.30 mm increase over 1 year* Trial lenses are fitted on the patient's eye to assess fit and performance. Adjustments can be made before finalizing the prescription. ƚ Manual calculation and dispensed according to patient's topography and refractive error. No trial lenses are used. ǂ Advanced software simulates the lens's performance, based on corneal topography and refractive data, calculating the parameters for the first fit. MCSCLs, myopia control soft contact lenses; ortho-k, orthokeratology. Table 1.
Survey questionnaire.
-
Responses 1 month 3 months 6 months 9 months 1 year EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) First year: Axial length 14.3 33.3 57.0 60.0 78.6 60.0 28.6 26.7 57 40.0 First year: Refraction 15.4 46.7 76.9 73.3 76.9 66.7 30.7 33.3 61.5 53.3 Subsequent years: Axial length 0 0 42.8 42.8 92.8 78.6 21.4 28.6 57.0 57.0 Subsequent years: Refraction 0 0 53.8 46.7 84.6 93.3 23.1 33.3 61.5 60.0 EECPs, expert eye care professionals; GECPs, general eye care professionals. Table 2.
Survey responses regarding the recommended follow-up schedule for the first year and subsequent years in children using MCSCLs.
-
Responses 1 month 3 months 6 months 9 months 1 year EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) First year: Axial length 14.3 28.6 57.0 64.3 78.6 64.3 28.6 28.6 57.0 50.0 First year: Refraction 15.4 37.5 76.9 81.3 76.9 56.2 30.7 31.3 61.5 50.0 Subsequent years: Axial length 0 6.7 42.8 46.7 92.8 73.3 21.4 26.7 57 53.3 Subsequent years: Refraction 0 0 53.8 53.3 84.6 80.0 23.0 26.7 61.5 46.7 EECPs, expert eye care professionals; GECPs, general eye care professionals. Table 3.
Survey responses on the recommended follow-up schedule for the first year and subsequent years in children using ortho-k lenses.
-
Patient selection: Age Myopia control contact lenses can be fitted for patients as young as 5 years old (in accordance with local guidelines and regulations). Myopia control contact lenses can be fitted up to early adulthood in patients in their 20s. Fitting protocol MCSCLs Trial lens fitting is the recommended method for fitting MCSCLs. Slit lamp examination and over-refraction are the key assessments of fit for MCSCLs. Ortho-k lenses Trial lens fitting, empirical manual calculation, and digital software using the patient's topography and refractive error are the main options for lens design in and fitting ortho-k contact lenses. Slit-lamp examination, corneal topography, and fluorescein pattern evaluation are the key parameters for assessing the fit of ortho-k lenses. Over-refraction can be assessed according to the ECP's preference. Visual acuity The acceptable corrected visual acuity outcome for children using myopia control contact lenses is 6/9 or better (monocular), although achieving 6/6 best corrected visual acuity should be the goal. Monitoring and follow-up schedule MCSCLs Comfort, vision, centration, and primary gaze lens position are the key parameters that should be assessed in patients prescribed MCSCLs. Edge alignment to the conjunctiva and push-up test recovery could also be included in the assessment. For children wearing MCSCLs, the recommended follow-up schedule in the first year is 3 months, 6 months, and 12 months, with refraction and axial length measurement as assessments. Vision, eye health, adaptation, and compliance assessments are also recommended. A 1-month follow-up can be recommended to ensure the treatment's suitability and a 9-month visit can also be considered. Ortho-k lenses Comfort and vision are the two key parameters recommended as assessments for routine follow-up with ortho-k lenses. An evaluation of the fluorescein pattern with the lens on can also be included. Ocular health is especially important to testt in patients using ortho-k lenses. For children wearing ortho-k lenses, the recommended follow-up schedule in the first year is 1 day, 1 month, 3 months, and 6 months, with refraction and axial length measurement as assessments. A 9-month visit can also be considered with an assessment of axial length (refraction optional). Corneal topography is recommended for every follow-up visit. Treatment outcomes The aim of myopia control treatment for children, regardless of age, should be a progression of ≤ 0.50 D over 1 year. For children 9 years old and below, the acceptable benchmark for an increase in axial length over 1 year is less than 0.20–0.30 mm. For children 10 years old and above, the acceptable benchmark for an increase in axial length over 1 year is ≤ 0.20 mm. Termination of treatment The appropriate age to discontinue the use of myopia control contact lenses is generally considered to be 18 years and above. Treatment with myopia control contact lenses can be discontinued when the progression is between 0.00 D and 0.25 D over 1 year. Treatment with myopia control contact lenses can be stopped when the increase in axial length is ≤ 0.10 mm over 1 year. Combination treatment If used as a combination treatment with myopia control contact lenses, the acceptable dosage of atropine is 0.01%–0.05%. ECP, eye care professional; MCSCL, myopia control soft contact lens; ortho-k, orthokeratology. Table 4.
Summary of consensus statements proposed by the EECP group.
Figures
(2)
Tables
(4)