









-
The prevalence of myopia is escalating to epidemic levels[1,2]. It has been estimated that it will affect 47% of adolescents and 40%–50% of the world's overall population by 2050[1,3]. In Asia, the prevalence can be as high as 50%, even reaching 95% in some countries[1,4−8].
Several evidence-based treatment options are now available for treating myopia in children, globally and in Asia. These include optical interventions such as myopia control soft contact lenses (MCSCLs), orthokeratology (ortho-k) lenses, myopia control spectacles, pharmacological interventions, red light therapy, and behavioral interventions, some of which may not be approved for use in all countries in the Asia-Pacific (APAC) region[1,9−13].
Awareness of myopia as a treatable condition and the proactive engagement of eye care professionals (ECPs) in managing myopia is increasing. However, a global survey of clinical practice patterns among ECPs managing myopia in children in 2022 demonstrated a continued preference towards spectacles, both single-vision and myopia control types[14]. A similar trend was observable among ECPs in Asia, with the top two prescribed modalities being single-vision spectacles (32.3%) and myopia control spectacles (16.8%)[14]. Ortho-k lenses, refractive corrective lenses, MCSCLs, single-vision soft contact lenses, and multifocal soft contact lenses showed prescription frequencies of 14.6%, 3.8%, 3.5%, 3.2%, and 2.2%, respectively[14]. Pharmaceutical treatments, progressive additional lenses, combination therapy, and bifocals were also among the modalities prescribed, at frequencies of 8.7%, 6.5%, 5.3%, and 3.2%, respectively[14].
In the absence of standardized treatment guidelines, many ECPs often rely on familiar practices and products such as single-vision spectacles. Moreover, the diverse practices and professional perspectives within ophthalmology and optometry often lead to variations in prescription, reflecting the importance of a common consensus across the eye care professions[9,14,15]. To combat the growing prevalence of myopia, ECPs must become adept at offering a comprehensive range of evidence-based myopia control treatment options to cater to every child's specific needs. For example, studies have shown that one in four children forget to bring their spectacles to school, and the wearing time of spectacles can impact treatment efficacy by approximately 50%[11,16,17]. Hence, it is important to consider treatment adherence and lifestyle factors when prescribing myopia control treatments[17]. Children wearing soft contact lenses show improvements in self-perception and self-esteem compared with those wearing spectacles[18]. In fact, MCSCLs were the first contact lenses to be approved by the United States Food and Drug Administration for slowing the progression of myopia in children between the ages of 8 and 12 years[19]. A similar impact on quality of life is seen in children using ortho-k lenses[20,21]. Hence, it may be worthwhile to expand on the use of these contact lens-based treatment modalities for myopia control.
Developing a simplified treatment algorithm that is based on real-world insights from the APAC region will serve as a starting point to help ECPs in this region to control childhood myopia more confidently, ensuring better patient outcomes. This position statement presents ways of integrating established evidence-based contact lens modalities, namely MCSCLs and ortho-k lenses, into clinical practice for myopia control.
-
An in-person advisory board meeting titled "Roundtable Meeting to Standardize Clinical Application of Myopia Control Contact Lenses' held at Kuala Lumpur, Malaysia in July 2024 convened a panel of ECPs from the APAC region. The discussions were led by Dr. Foo Li Lian and supported by Dr. Kate Gifford. The objectives of the meeting were the following:
(1) Assessment of regional clinical practice patterns in managing childhood myopia, focusing on soft contact lenses and ortho-k lenses.
(2) Highlighting the patient journey's milestones through diagnosis, treatment, and follow-up.
(3) Achieving a consensus for standardization of treatment protocols.
Prior to the in-person meeting, an online questionnaire (Table 1) was distributed via SurveyMonkey (Palo Alto, California, USA) to a pre-selected cohort of optometrists and ophthalmologists (n = 34) across Chinese Taipei (China), Hong Kong SAR (China), Japan, Malaysia, Singapore, and South Korea, enquiring about the prevalent clinical practices pertaining to prescribing MCSCLs and ortho-k lenses to children with myopia. The survey participants were stratified into two groups, namely expert eye care professionals (EECPs) and general eye care professionals (GECPs). EECPs are ECPs who are recognized as thought leaders in the field of eye care. Their expertise includes clinical experience, contributions to academic literature, or leadership roles in professional organizations. GECPs are qualified ECPs who provide routine clinical services. The GECP group participated in the survey only, whereas the EECP group participated in the survey and the subsequent in-person roundtable discussion, and co-authored this position statement. The participants in both groups were selected to reflect a balanced representation of the two ECP categories.
Table 1. Survey questionnaire.
What is the youngest and oldest patient you have fitted with myopia control contact lenses? No answer options provided.
The respondents added their own responses.How do you fit your patients with myopia control contact lenses? • Soft contact lenses: Trial lens fit*
• Soft contact lenses: Dispensed according to the patient's refractive error
• Ortho-k: Trial lens fit
• Ortho-k: Empirical – manual calculation and dispensed according to the patient's topography and refractive errorƚ
• Ortho-k: Empirical – digital software calculating the parameters for first fit according to the topography and refractive errorǂWhat would you deem as an acceptable best-corrected visual acuity outcome for children using myopia control contact lenses? • 6/6 only
• 6/7.5 or better
• 6/9 or better
• 6/12 or betterWhat would you check in terms of fit assessment? (Please select all that apply.) • Soft contact lenses: Slit-lamp examination
• Soft contact lenses: Over-refraction
• Ortho-k: Slit-lamp examination
• Ortho-k: Fluorescein pattern evaluation
• Ortho-k: Over-refraction
• Ortho-k: Corneal topography
• Other (please specify whether this is for soft contact lenses and/or ortho-k)If you have selected soft contact lenses, please indicate what you would routinely check or assess. • Comfort
• Vision
• Centration and cornea coverage
• Edge alignment to conjunctiva
• Primary gaze post-blink movement
• Push-up test recoveryIf you have selected ortho-k lenses, please indicate what you would routinely check or assess. • Comfort
• Vision
• Fluorescein pattern evaluation with the lens onMonitoring soft contact lenses: What would be your follow-up regime for the first year and subsequent years in children using MCSCLs?
What are the parameters you use to monitor your patients with MCSCLs for myopia progression during follow-up visits?• First year: Axial length: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• First year: Refraction: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• Subsequent years: Axial length: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 year
• Subsequent years: Refraction: 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, 1 yearMonitoring ortho-k lenses: What would be your follow-up regime for the first year and subsequent years in children using ortho-k lenses?
What are the parameters you use to monitor your patients with ortho-k lenses for myopia progression during follow-up visits?• First year: Axial length at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• First year: Refraction at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• Subsequent years: Axial length at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 year
• Subsequent years: Refraction at 1 day, 3 days, 5 days, 1 week, 2 weeks, 3 weeks, 1 month, 3 months, 6 months, 9 months, and 1 yearFor children 9 years and below: What would you consider as an acceptable myopia control treatment effect, based on myopia's stability of refraction or over-refraction in 1 year? • Zero progression
• ≤ 0.50 D progression
• ≤ 0.75 D progression
• ≤ 1.00 D progression
• > 1.00 D progressionFor children 9 years and below: What would you consider as an acceptable myopia control treatment effect, based on myopia stability in terms of axial length in 1 year? • ≤ 0.05 mm increase
• ≤ 0.10 mm increase
• ≤ 0.20 mm increase
• ≤ 0.30 mm increase
• > 0.30 mm increaseFor children 10 years and above: What would you consider as an acceptable myopia control treatment effect, based on myopia stability of refraction/over-refraction in 1 year? • Zero progression
• ≤ 0.50 D progression
• ≤ 0.75 D progression
• ≤ 1.00 D progression
• > 1.00 D progressionFor children 10 years and above: What would you consider as an acceptable myopia control treatment effect, based on myopia stability of axial length in 1 year? • ≤ 0.05 mm increase
• ≤ 0.10 mm increase
• ≤ 0.20 mm increase
• ≤ 0.30 mm increase
• > 0.30 mm increaseCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to age. • Any age
• 12 years old and below
• 13–15 years old
• 15–18 years old
• Beyond 18 years oldCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to myopia stability of refraction/over-refraction. • Zero progression over 1 year
• ≤ 0.50 D progression over 1 year
• ≤ 0.75 D progression over 1 year
• ≤ 1.00 D progression over 1 year
• > 1.00 D progression over 1 yearCeasing myopia control lens wear: When would you consider it reasonable to stop the use of myopia control contact lenses? Please select according to myopia stability of axial length. • ≤ 0.05 mm increase over 1 year
• ≤ 0.10 mm increase over 1 year
• ≤ 0.20 mm increase over 1 year
• ≤ 0.30 mm increase over 1 year
• > 0.30 mm increase over 1 year* Trial lenses are fitted on the patient's eye to assess fit and performance. Adjustments can be made before finalizing the prescription. ƚ Manual calculation and dispensed according to patient's topography and refractive error. No trial lenses are used. ǂ Advanced software simulates the lens's performance, based on corneal topography and refractive data, calculating the parameters for the first fit. MCSCLs, myopia control soft contact lenses; ortho-k, orthokeratology. The questionnaire was designed to understand ECPs' practices in managing myopia using contact lenses, with an emphasis on key parameters such as the patient's age, fitting assessments, monitoring protocols, combination therapy with atropine, follow-up schedules, and criteria for cessation of treatment. ECPs participating in the online survey provided informed consent for the anonymized sharing of the survey's results for discussion during the in-person advisory board meeting and for inclusion in the resulting publication.
At the in-person meeting, the EECP group reviewed and deliberated on the survey's outcomes. This discussion included an analysis of the practice preferences highlighted by the survey, culminating in a consensus on the most appropriate practices for recommendation. To facilitate this process, online polling was conducted using Slido software (Vajnorská, Slovakia).
Data analysis
-
The percentage of respondents for a particular response to a question in the online survey was determined for the GECP and EECP groups. Slido software was used to record the responses to consensus statements during the in-person advisory board meeting of the EECPs. The relatively small sample size precluded meaningful inferential statistical analysis; accordingly, the survey's results and responses to the consensus statements have not been evaluated for statistical significance and are presented descriptively.
-
The EECP group consisted of eight optometrists and eight ophthalmologists from Chinese Taipei (China) (three ophthalmologists), Hong Kong SAR (China) (one optometrist), Japan (one ophthalmologist), Malaysia (four optometrists), Singapore (two optometrists, two ophthalmologists), and South Korea (one optometrist, two ophthalmologists). The GECP group comprised 13 optometrists and five ophthalmologists, from Chinese Taipei (China) (two ophthalmologists), Hong Kong SAR (China) (three optometrists), Japan (two ophthalmologists), Malaysia (three optometrists), Singapore (seven optometrists), and South Korea (one ophthalmologist).
Of the EECP group, 69% and of the GECP group, 67% had private practices but the remaining had public or a combination of public and private practices.
The prescribing pattern showed that most of the EECPs and GECPs prescribed both MCSCLs (EECP, 94%; GECP, 94%) and ortho-k lenses (EECP, 88%; GECP, 83%). Moreover, 56% of the EECP group, and 78% of respondents from the GECP group selected that they also practiced other myopia treatment options.
Patient selection according to age
-
Respondents were asked to select the youngest and oldest ages that they would treat with myopia control contact lenses (MCSCLs and ortho-k lenses). The youngest ages most reported by the EECP group were 6 years (31%) and 7 years (31%), respectively (Fig. 1a), whereas the GECP group reported 5 years (28%) and 6 years (33%) (Fig. 1b).
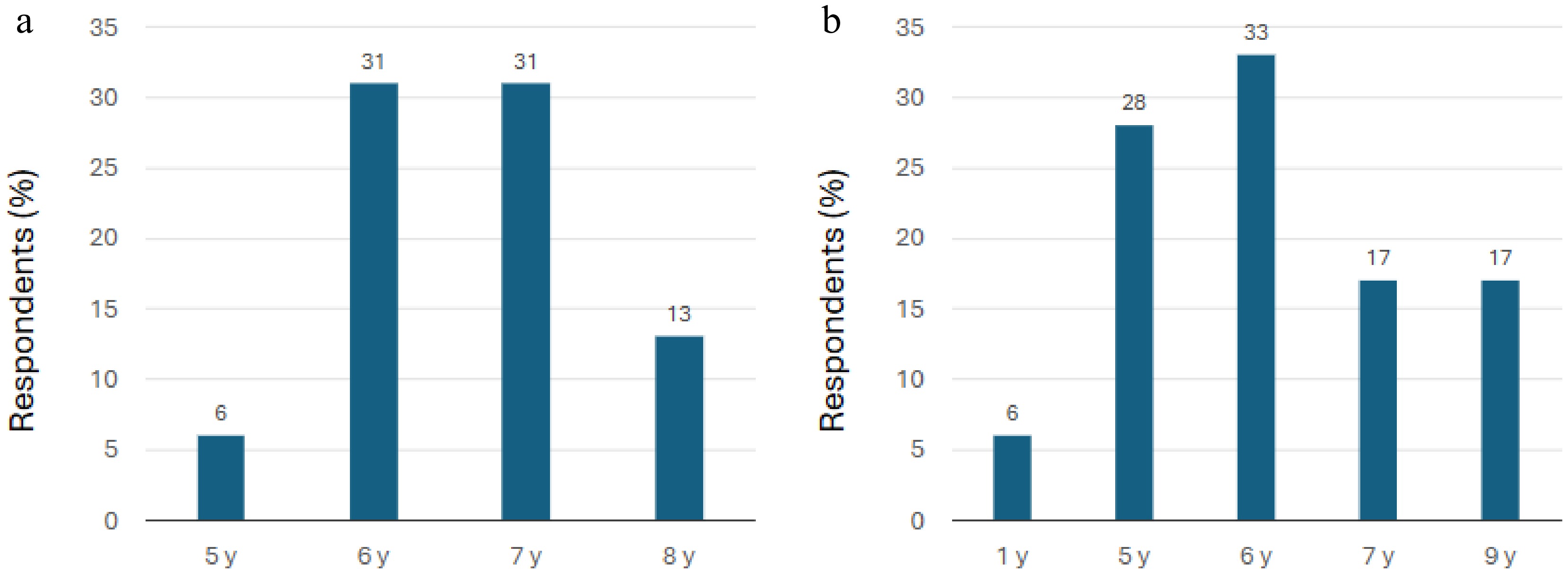
Figure 1.
Youngest ages at which ECPs participating in the survey prescribe myopia control contact lenses. (a) EECP group (n = 16). (b) GECP group (n = 18). Note: The x-axis values are only representative of the responses to the relevant question, which required free text responses (see Table 1) and not the selection of ages within a defined continuous age range. EECP, expert eye care professionals; GECP, general eye care professionals; y, years.
The most frequently reported oldest ages in the EECP group were 16 years (25%), 14 years (13%), 15 years (13%), and 18 years (13%), whereas in the GECP group, they were 15 years (19%), 16 years (14%), and 20 years (14%) (Fig. 2).
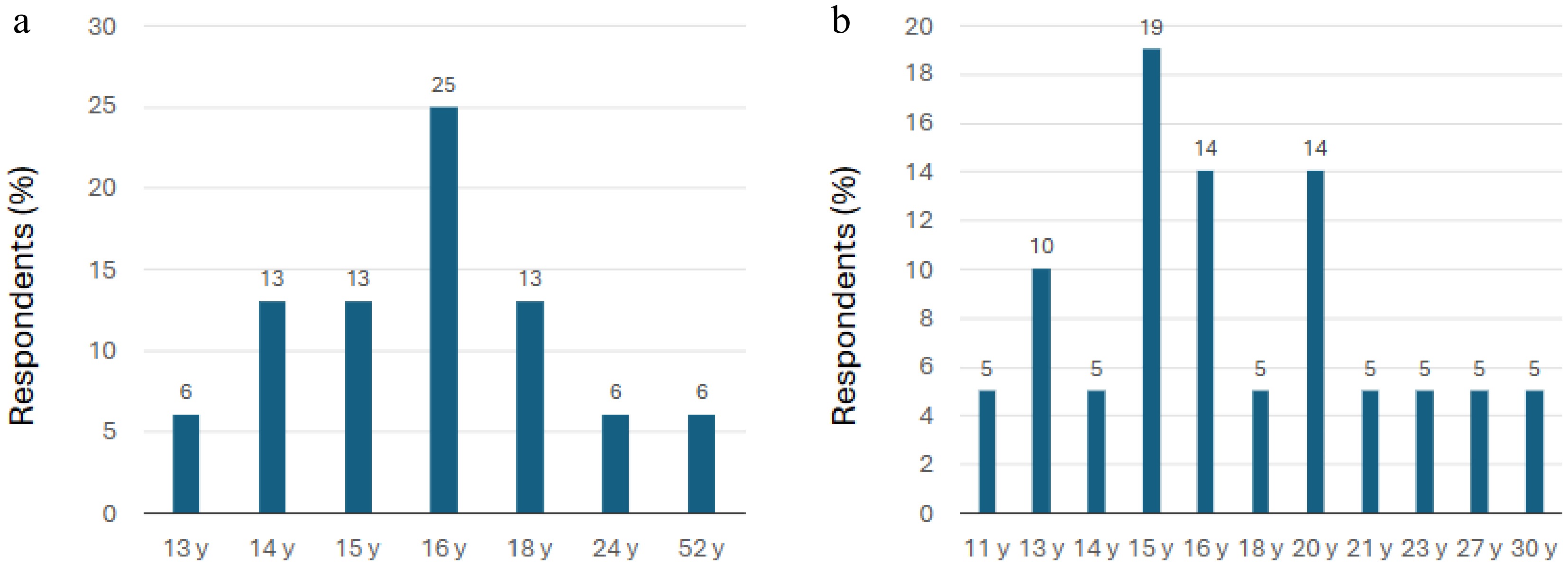
Figure 2.
Oldest ages at which ECPs participating in the survey prescribe myopia control contact lenses. (a) EECP group (n = 16). (b) GECP group (n = 18). Note: The x-axis values are only representative of the responses to the relevant question, which required free text responses (see Table 1) and not the selection of ages within a defined continuous age range. EECP, expert eye care professionals; GECP, general eye care professionals; y, year.
During the qualitative roundtable meeting, the EECP panel agreed on the following, wherever local guidelines and regulations permit:
(1) Myopia control contact lenses can be fitted for patients as young as 5 years old.
(2) Myopia control contact lenses can be fitted up to early adulthood in patients in their 20s.
Fitting protocol
MCSCLs
Fitting procedures
-
The majority of respondents from both groups selected: 'Trial lens fit' (69% of EECPs, 62.5% of GECPs) for soft contact lenses. 'Dispensing according to the patient's refractive error' was selected by 25% of EECPs and 38% of GECPs respondents. The refractive error was to be calculated with the trial lens on. Trial lens fit was defined as the lens fitted on the patient's eye to assess fit and performance, with adjustments made before finalizing the prescription.
During the qualitative roundtable discussion, the EECP group agreed on the following:
Trial lens fitting is the recommended method for fitting MCSCLs.
Fit and vision assessment
-
The majority of respondents from both groups reported slit-lamp examination (94% of EECP, 88% of GECP) and over-refraction (75% of EECP, 69% of GECP) as the key assessments for the fit of soft contact lenses.
During the discussion, the group agreed on the following:
Slit lamp examination and over-refraction are the key fit assessments for MCSCLs.
Ortho-k lenses
Fitting procedures
-
Most respondents from both groups suggested 'Trial lens fit' (56% of EECPs, 50% of GECPs) and 'Empirical calculation – manual calculation and dispense as per the patient's topography error' (56% of EECPs, 50% of GECPs) as key approaches to fitting ortho-k lenses. Of the GECP group, 62.5% respondents also selected 'Empirical calculation – Digital software calculating the parameters for first fit according to the topography and refractive error'. Empirical manual calculation was defined as dispensing according to the patient's topography and refractive error without the use of trial lenses. Empirical calculation with digital software was defined as the use of advanced software to simulate the lens's performance, based on corneal topography and refractive data to calculate the parameters for the first lens fit.
After discussion, experts agreed to include digital software as one of the key recommended methods.
The group came to the following conclusion:
Trial lens fitting, empirical manual calculation, and digital software to dispense according to the patient's topography and refractive error are the main options for lens design in fitting ortho-k contact lenses.
Fit and vision assessment
-
The majority of respondents from both groups suggested slit lamp examination (81% of EECPs, 94% of GECPs), over-refraction (69% of EECPs, 75% of GECPs), corneal topography (75% each for both EECPs and GECPs), and fluorescein pattern evaluation (81% of EECPs, 87% of GECPs) as key assessments for fitting ortho-k lenses. However, an EECP commented that over-refraction may not be useful for fitting an ortho-k lens, as it does not predict how the cornea will respond to the lens. However, regional differences were evident, as observed in the survey and the subsequent discussion.
Slit-lamp examination, corneal topography, and fluorescein pattern evaluation are the key parameters for assessing the fit of ortho-k lenses. Over-refraction assessment can be used according to the ECP's preference.
Visual acuity
-
The majority of respondents from both groups chose '6/7.5 or better' (50% of EECPs, 63% of GECPs) as the acceptable best-corrected visual acuity (monocular) in the surveys, with 13% of the EECPs and 19% of the GECPs choosing '6/9 or better'. During the discussion, most experts agreed that visual acuity of 6/9 or better could be considered as an acceptable outcome for patients using myopia control contact lenses. However, it should be clear that achieving 6/6 best-corrected visual acuity should be the goal.
Hence, the group reached the following conclusion:
Acceptable corrected visual acuity outcome for children using myopia control contact lenses can be 6/9 or better (monocular), although achieving 6/6 best corrected visual acuity should be the goal.
Monitoring and follow-up schedule
MCSCLs
Monitoring
-
When asked about their preferred assessment criteria for patients regarding the use of MCSCLs, the majority of the respondents from both groups chose comfort (100% of EECPs, 67% of GECPs), vision (93% of EECPs, 100% of GECPs), centration and cornea coverage (80% of EECPs, 87% of GECPs), and primary gaze post-blink movement (80% of EECPs, 73% of GECPs). Note that vision can be subjective or objective, depending on the ECP's preferred practice. The other options, 'edge alignment to conjunctiva' and 'push-up test recovery', were selected by 60% and 47% in the EECP group, and 40% for both in the GECP group, respectively. Hence, it was imperative to discuss their inclusion in the preferred monitoring assessments. Experts from Hong Kong SAR (China) noted that edge alignment to the conjunctiva and push-up test recovery might not be necessary and are thus not typically performed in their practices in Hong Kong SAR (China). In contrast, experts from Taipei (China) and Singapore indicated that they conduct both tests. One expert emphasized the importance of performing these tests to ensure the satisfaction of both the patient and the parents with the overall process. Following this discussion, most experts concurred that both parameters could be included in the assessments.
Hence, the group reached the following conclusion:
Comfort, vision, centration, and primary gaze lens position are the key parameters that should be assessed in patients prescribed MCSCLs. Edge alignment to the conjunctiva and push-up test recovery could also be included in the assessment.
Follow-up schedule
-
The survey responses for the follow-up regime preferences for wearing MCSCLs are shown in Table 2. Similar proportions of respondents in both groups of ECPs reported following up in the first year of myopia control lens use, measuring axial length and refraction at 3 months, 6 months, and 1 year. However, at 9 months, 28.6% of EECPs and 26.7% of GECPs reported scheduling appointments for measuring axial length, and 30.7% of EECPs and 33.3% of GECPs scheduled appointments for testing refraction. Moreover, 14% and 15% of the EECP group, and 33% and 46.7% of respondents from the GECP group recommended a follow-up visit for assessing axial length and refraction at 1 month. During the discussion, experts agreed that a 1-month follow-up visit in the first year is beneficial to assess the patient's adaptation to the lens. It was also agreed that the 9-month visit can be recommended; however, the 1-month visit should be limited to the first year of treatment, with a focus on refraction as the main assessment, along with other assessments that are necessary to determine the treatment's suitability. Some experts noted that these assessments might not be critical, as long as the child reports acceptable vision quality.
Table 2. Survey responses regarding the recommended follow-up schedule for the first year and subsequent years in children using MCSCLs.
Responses 1 month 3 months 6 months 9 months 1 year EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) First year: Axial length 14.3 33.3 57.0 60.0 78.6 60.0 28.6 26.7 57 40.0 First year: Refraction 15.4 46.7 76.9 73.3 76.9 66.7 30.7 33.3 61.5 53.3 Subsequent years: Axial length 0 0 42.8 42.8 92.8 78.6 21.4 28.6 57.0 57.0 Subsequent years: Refraction 0 0 53.8 46.7 84.6 93.3 23.1 33.3 61.5 60.0 EECPs, expert eye care professionals; GECPs, general eye care professionals. Hence, the group reached the following conclusion:
For children wearing MCSCLs, the recommended follow-up schedule in the first year is 3 months, 6 months, and 12 months with refraction and axial length measured as assessments. Vision, eye health, adaptation, and compliance assessments are also recommended. A 1-month follow-up can be recommended to ensure the treatment's suitability and a 9-month visit can also be considered.
Ortho-k lenses
Monitoring
-
When asked about their preferred assessment criteria for patients wearing ortho-k lenses, the majority of respondents from both groups chose comfort (100% of EECPs, 75% of GECPs), vision (87% of EECPs, 100% of GECPs), and evaluating the fluorescein pattern with the lens on (87% of EECPs, 100% of GECPs). The experts noted that monitoring corneal health is especially important during ortho-k lens treatment.
During the discussion, the group agreed on the following:
Comfort and vision are the two key parameters recommended as assessments for routine follow-up in those using ortho-k lenses. Evaluating the fluorescein pattern with the lenses on can also be included. Ocular health testing is especially important in patients using ortho-k lenses.
Follow-up schedule
-
Similar to those for wearing MCSCLs, the survey responses for the follow-up regime preferences for ortho-k lenses are shown in Table 3. Similar proportions of respondents in both groups of ECPs reported following up in the first year of myopia control lens use, measuring axial length and refraction at 3 months, 6 months, and 1 year. However, around 30% of both EECPs and GECPs recommended scheduling appointments at 9 months for axial length and refraction for ortho-k lens patients. For the 1-month follow-up visit during the first year, 14.3% of EECPs recommended a follow-up for assessing axial length and 15.4% for assessing refraction, whereas 28.6% and 37.5% of GECPs recommended these assessments, respectively. During the discussion, it was agreed that the 9-month visit can be recommended for both assessments. However, the 1-month visit was recommended only for the first year of treatment. During the discussion, it was decided that there may not be any need for assessing refraction at this visit, but the panel was divided on this. However, an corneal topography assessment at this visit was considered to be a key measure to guide further treatment.
Table 3. Survey responses on the recommended follow-up schedule for the first year and subsequent years in children using ortho-k lenses.
Responses 1 month 3 months 6 months 9 months 1 year EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) EECPs (%) GECPs (%) First year: Axial length 14.3 28.6 57.0 64.3 78.6 64.3 28.6 28.6 57.0 50.0 First year: Refraction 15.4 37.5 76.9 81.3 76.9 56.2 30.7 31.3 61.5 50.0 Subsequent years: Axial length 0 6.7 42.8 46.7 92.8 73.3 21.4 26.7 57 53.3 Subsequent years: Refraction 0 0 53.8 53.3 84.6 80.0 23.0 26.7 61.5 46.7 EECPs, expert eye care professionals; GECPs, general eye care professionals. Hence, the group reached the following conclusion:
For children wearing ortho-k lenses, the recommended follow-up schedule in the first year is 1 day, 1 month, 3 months, and 6 months, with refraction and axial length measured as assessments. A 9-month visit can also be considered to assess axial length (refraction optional). Corneal topography is recommended for every follow-up visit.
Treatment outcomes
Spherical equivalent
-
For children aged 9 years old and below, the majority of the EECPs (86%) and GECPs (56%) chose acceptable treatment control based on myopia stability of refraction/over-refraction over 1 year as ≤ 0.50 D progression. However, 14% of EECPs and 25% of GECPs also chose ≤ 0.75 D progression as an acceptable effect.
For children 10 years old and above, the majority of the EECPs (100%) and GECPs (75%) defined an acceptable treatment control effect as a progression of ≤ 0.50 D.
It is worth noting that myopia progression target of 0.50 D per year is a stringent one. The mean progression for Asian children aged 7–8 years can be just over 1.00 D per year[22]. Hence, for a target of 0.50 D per year, there is a need to slow down myopia's progression by more than 50% in the children whose progression rate is higher than the mean of 1.00 D. It is important to have reasonable expectations of the mypoia-control treatment and base them on an understanding of the patient's history and adherence to treatment.
During the discussion, the group agreed on the following:
The aim for the effect of a myopia control treatment for children, regardless of age, should be progression of ≤ 0.50 D over 1 year.
It should be noted that spherical equivalent is commonly obtained via noncycloplegic refraction in children.
Axial length
-
For children 9 years old and below, 21% of the EECPs and 69% of the GECPs defined the acceptable treatment control effect based on myopia stability over 1 year as an increase in axial length of ≤ 0.20 mm. However, 36% of EECPs and only 6% of GECPs chosen an increase of ≤ 0.30 mm as an acceptable effect.
During the discussion, the group agreed on the following:
For children 9 years old and below, the acceptable benchmark for axial progression over 1 year is less than 0.20–0.30 mm over 1 year.
For children 10 years old and above, 43% of the EECPs and 44% of the GECPs defined the acceptable treatment control effect based on myopia stability over 1 year as an increase in axial length of ≤ 0.20 mm. However, 21% of the EECPs and 44% of the GECPs chose an increase of ≤ 0.10 mm as an acceptable effect and 36% of EECPs voted for an increase of ≤ 0.05 mm to be acceptable.
During the discussion, the group agreed on the following:
For children 10 years old and above, the acceptable benchmark for an increase in axial length is ≤ 0.20 mm over 1 year.
Termination of treatment
Age
-
Regarding age, 50% of the EECP group and 44% of respondentsfrom the GECP group agreed that myopia control contact lenses should be continued beyond 18 years of age. However, 43% of EECPs and 44% of GECPs selected 15–18 years as a reasonable age to stop the use of myopia control contact lenses. One expert remarked that it would be ideal to continue for up to 18 years of age before slowly starting to cease the treatment.
During the discussion, the group agreed on the following:
The appropriate age to discontinue the use of myopia control contact lenses is generally considered to be 18 years and above.
Spherical equivalent
-
Half of the EECPs (50%) and most of the GECPs (82%) agreed that the acceptable treatment control effect based on myopia stability of refraction/over-refraction over 1 year is a progression of ≤ 0.50 D, whereas 50% of the EECPs believed that myopia control contact lens use should be continued until zero progression in refractive myopia is observed.
However, during the discussion, it was suggested that a limit of 0.25 D would be more acceptable. The experts remarked that although zero progression is ideal, the variability of subjective refraction can introduce fluctuations in the readings. Therefore, a range of 0.00–0.25 D is considered to be more realistic.
Hence, the group agreed on the following:
Controlling myopia contact lenses can be discontinued when the progression is between 0.00 and 0.25 D over 1 year.
Axial length
-
The majority of ECPs (71%) and GECPs (63%) agreed that an increase of ≤ 0.05 mm in axial length over 1 year is a reasonable criterion to discontinue the use of myopia control contact lenses. However, 21% of EECPs and 25% of GECPs chose an increase of ≤ 0.10 mm in axial length as an acceptable benchmark. During the discussion, it was pointed out that despite the majority agreeing to a ≤ 0.05-mm increase as an acceptable measurement to stop treatment, there is a margin of error when assessing the axial length of around this magnitude. It was mentioned that accuracy concerns can present themselves in resource-constrained environments[23]. Hence, the participants were asked to choose between ≤ 0.1 and ≤ 0.2 mm as acceptable limits, and ≤ 0.1 mm received the majority vote.
The group agreed on the following:
Controlling myopia using contact lenses can be stopped when the increase in axial length is ≤ 0.10 mm over 1 year.
Combination treatment
-
The potential for combination treatments in improving myopia control versus monotherapy with optical, pharmaceutical, or behavioral treatments was discussed. The survey attempted to understand the concentration of atropine commonly considered for use as a combination therapy with myopia control contact lenses.
The majority of EECPs (94%) and GECPs (72%) agreed that 0.01%–0.05% atropine is the recommended atropine dosage for combination with myopia control lenses. Only 19% of EECPs and 11% of GECPs chose "higher than 0.05%–0.5% atropine" as an option. It is important to note that 63% of EECPs and 28% of GECPs do not use atropine in combination with myopia control lenses. The group also recognized the current limitations in the evidence regarding combination treatments, with most published studies investigating 0.01% atropine in combination treatments; data on other concentrations are limited.
Hence, the group reached the following conclusion:
If used as a combination treatment with myopia control contact lenses, the acceptable dosage of atropine is 0.01%–0.05%.
Other clinical concerns
-
In addition to discussing the survey results, the EECP group discussed other clinical concerns regarding myopia control, such as low contrast acuity, which is commonly encountered by patients wearing MCSCLs, especially at night. The group noted that some patients complain of glare and dispersion of light. Similar challenges are encountered with ortho-k lenses. There was also a discussion regarding the incidence of such challenges with the usage of ortho-k lenses with a small optical zone, especially by children with larger pupils and/or in combination with atropine. One of the experts remarked that handling these patient concerns involves discussing the benefits of the treatment, which exceed the minor adverse effects. Redesigning the ortho-k lens with an increased optic zone can be considered for patients with serious visual complaints. For soft contact lenses, an alternative treatment approach may need to be adopted if the patient is not convinced of the benefits of the treatment.
The need for clear communication between the ECP and both the patient and the parent/caregiver was highlighted during the discussion. Communicating the need for myopia treatment and setting and managing treatment expectations was deemed to be an important aspect of clinical practice. It was noted that communication is crucial during the fitting process to assess comfort, vision, and acceptance and subsequently during the follow-up visits to ascertain tolerability and enhance adherence.
-
As highlighted in the introduction, the adoption of evidence-based, advanced myopia control solutions such as MCSCLs or ortho-k lenses, remains suboptimal in the APAC region. Although some studies have been conducted to understand myopia management practices globally and among European ECPs, knowledge of the prescribing patterns in childhood myopia among ECPs in the APAC region is limited[14,24]. Moreover, expert opinions or consensus recommendations in prescribing myopia control solutions are lacking at the regional level, although country-level recommendations may be available[25]. As evident from this article, several factors need to be considered to achieve favorable outcomes with MCSCLs or ortho-k lenses for controlling myopia. The lack of standardized regional or local guidelines in prescribing MCSCLs or ortho-k lenses hinders consistency in prescribing practices related to the age of prescription, fit assessment, monitoring efficacy, and treatment cessation. This lack of consistency may lead to variable outcomes that can compromise patients' experience and trust, further inhibiting the adoption of these potent solutions for controlling myopia.
This study combines insights derived from the real-world clinical practice of ECPs in the region with expert opinions from regional thought leaders in the myopia control landscape to propose consensus recommendations on the best practices in prescribing contact lenses for childhood myopia control. The results from the survey conducted among the larger group of ECPs in the APAC region, as well as discussions conducted by an expert panel of ECPs, are presented in this position statement. A summary of the consensus recommendations from the roundtable discussion is provided in Table 4.
Table 4. Summary of consensus statements proposed by the EECP group.
Patient selection: Age Myopia control contact lenses can be fitted for patients as young as 5 years old (in accordance with local guidelines and regulations). Myopia control contact lenses can be fitted up to early adulthood in patients in their 20s. Fitting protocol MCSCLs Trial lens fitting is the recommended method for fitting MCSCLs. Slit lamp examination and over-refraction are the key assessments of fit for MCSCLs. Ortho-k lenses Trial lens fitting, empirical manual calculation, and digital software using the patient's topography and refractive error are the main options for lens design in and fitting ortho-k contact lenses. Slit-lamp examination, corneal topography, and fluorescein pattern evaluation are the key parameters for assessing the fit of ortho-k lenses. Over-refraction can be assessed according to the ECP's preference. Visual acuity The acceptable corrected visual acuity outcome for children using myopia control contact lenses is 6/9 or better (monocular), although achieving 6/6 best corrected visual acuity should be the goal. Monitoring and follow-up schedule MCSCLs Comfort, vision, centration, and primary gaze lens position are the key parameters that should be assessed in patients prescribed MCSCLs. Edge alignment to the conjunctiva and push-up test recovery could also be included in the assessment. For children wearing MCSCLs, the recommended follow-up schedule in the first year is 3 months, 6 months, and 12 months, with refraction and axial length measurement as assessments. Vision, eye health, adaptation, and compliance assessments are also recommended. A 1-month follow-up can be recommended to ensure the treatment's suitability and a 9-month visit can also be considered. Ortho-k lenses Comfort and vision are the two key parameters recommended as assessments for routine follow-up with ortho-k lenses. An evaluation of the fluorescein pattern with the lens on can also be included. Ocular health is especially important to testt in patients using ortho-k lenses. For children wearing ortho-k lenses, the recommended follow-up schedule in the first year is 1 day, 1 month, 3 months, and 6 months, with refraction and axial length measurement as assessments. A 9-month visit can also be considered with an assessment of axial length (refraction optional). Corneal topography is recommended for every follow-up visit. Treatment outcomes The aim of myopia control treatment for children, regardless of age, should be a progression of ≤ 0.50 D over 1 year. For children 9 years old and below, the acceptable benchmark for an increase in axial length over 1 year is less than 0.20–0.30 mm. For children 10 years old and above, the acceptable benchmark for an increase in axial length over 1 year is ≤ 0.20 mm. Termination of treatment The appropriate age to discontinue the use of myopia control contact lenses is generally considered to be 18 years and above. Treatment with myopia control contact lenses can be discontinued when the progression is between 0.00 D and 0.25 D over 1 year. Treatment with myopia control contact lenses can be stopped when the increase in axial length is ≤ 0.10 mm over 1 year. Combination treatment If used as a combination treatment with myopia control contact lenses, the acceptable dosage of atropine is 0.01%–0.05%. ECP, eye care professional; MCSCL, myopia control soft contact lens; ortho-k, orthokeratology. Although the survey's results led to important insights potentially impacting clinical practice, particularly in the APAC region, these insights must be evaluated in the context of scientific evidence as well, as noted in the roundtable discussion. For example, 81% of EECPs and 87% of GECPs reported evaluating the fluorescein pattern as a key assessment parameter for ortho-k lenses, although it has been reported that fluorescein-based assessment does not offer significant benefits for fitting lenses[26]. However, in recognition of the prevalent practices in the region, the panel reached a consensus that evaluating fluorescein patterns may be considered a key parameter for assessing the fit of ortho-k lenses (Table 4).
In terms of visual acuity, the panel agreed that 6/9 or better vision is an acceptable outcome for myopia control contact lenses, although the goal should be 6/6. It is possible to achieve 6/6 vision with these lenses, as observed in a randomized clinical trial, in which children wearing MiSight® 1 day lenses for myopia control achieved 6/6 vision across all visits over a 6-year period[17,27].
For children wearing MCSCLs, the panel recommended follow-up visits at 3 months, 6 months, and 12 months within the first year, with a 1-month follow-up conducted to ensure the suitability of the treatment. Notably, the International Myopia Institute (IMI) Clinical Management Guidelines recommends a 1-month follow- up for all patients undergoing myopia control to assess the suitability of the treatment, regardless of the treatment type; a 3-month follow-up is suggested for patients on atropine or ortho-k lenses, then a 6-month follow up in the first year and every 6 months thereafter[15]. An additional follow-up at 9 months could also be considered. For children wearing ortho-k lenses, the IMI guidelines recommend follow-up at 1 day, 1 week, 1 month, 3 months, and 6 months in the first year, and then every 6 months thereafter[15]. In alignment with these guidelines and the prevalent clinical practice as per the survey's results, the panel recommended follow-ups at 1 day, 1 month, 3 months, and 6 months in the first year to measure refraction and axial length. An additional 9-month follow-up visit may be considered.
Ethnicity, age at the onset of myopia, and key environmental exposures have been shown to be associated with myopia's progression and are therefore incorporated into evaluating the treatment's efficacy for a given patient[15]. Earlier age of myopia onset has also been found to pose a considerable risk for high myopia in adulthood, as demonstrated by Hu et al. in a study conducted in 443 participants in China[28,29]. However, the role of baseline myopia in determining progression remains uncertain, with some studies indicating a potential promotive effect[30] and others demonstrating no influence[31].
The panel's recommended definition of successful myopia control for children, regardless of age, should be a progression of ≤ 0.50 D over 1 year (Table 4). Although recommendations were also made regarding the acceptable benchmark for increased axial length as a treatment outcome, some experts suggested more stringent values to correct fast-growing eyes[32,33]. Eye growth is a normal part of development in all young patients. It has also been proposed that the success of myopia control should be measured by the slowing of the increase in axial length to reach the growth in axial length in emmetropic eyes in children of the same age[34]. Across ethnicities, stable emmetropic eyes have been shown to grow at 0.24 mm/year at 6 years of age, decreasing to 0.05 mm/year at 11 years of age[35]. These physiologic emmetropic growth trajectories should inform the criteria for successful myopia control. However, it has also been proposed that 25% faster eye growth compared with that in emmetropic eyes is acceptable as a successful outcome of myopia control[36,37]. Therefore, achieving an annual axial length increase of less than 0.2 mm in children aged ≥ 10 years was perceived by the EECPs as a sign of effective myopia control, whereas a reduction to approximately 0.1 mm per year is considered to be a clinically acceptable outcome.
Several factors need to be considered before stopping myopia control treatment with lenses[15], the main factors being age and myopia progression, as assessed by measurements of spherical equivalent and axial length. It is important to note that the decision to stop treatment is based on a combination of these and other factors like lifestyle and treatment adherence. The panel recommended discontinuing treatment with myopia control contact lenses at 18 years or above. This recommendation aligns with IMI guidelines recommending the discontinuation of myopia control treatments during the expected age of myopia's stabilization, which can extend up to the 20s[15].
The panel discussed combination therapy as a potential strategy to further enhance the outcomes of myopia control. Among these, the use of contact lenses in conjunction with atropine has been extensively studied[38]. Although higher concentrations of atropine (0.5%–1%) have demonstrated substantial efficacy in slowing myopia's progression, their use is often limited by side effects such as photophobia and reduced near visual acuity[39]. Studies evaluating lower concentrations have shown that 0.01% atropine can achieve better myopia control and less axial elongation than 0.02% atropine, suggesting a dose-dependent relationship[38,39].
Multiple randomized controlled trials have demonstrated the enhanced efficacy of ortho-k lenses when used in combination with 0.01% atropine[38]. When combined with MiSight® 1 day daily disposable, dual-focus soft contact lenses, 0.01% atropine has been associated with slower myopia progression (0.25 ± 0.25 D over 1 year) compared with the rate observed prior to treatment (1.12 ± 0.75 D over 3 years)[40]. However, other evidence indicates no significant difference between 0.01% atropine monotherapy and combination treatment with MiSight® 1 day lenses and 0.01% atropine[41]. Despite some ECPs reporting the successful use of moderate atropine concentrations in combination therapy without experiencing the adverse visual effects commonly seen with higher doses[42], it remains prudent to initiate combination therapy with a low concentration of atropine, given the current body of evidence.
Although its use is off-label in most countries, survey data from Wolffsohn et al. has identified that some ECPs believe combination treatment to be more effective than monotherapy alone[14]. However, the clinical evidence for the additive effect of atropine is limited and inconclusive, and effects like rebounding after discontinuation have been documented[38,43].
As a growing global health concern, myopia demands a unified management strategy to effectively mitigate its impact[14]. This position statement presents the attitude and practices of a selection of optometrists and ophthalmologists in their approach to the growing and concerning epidemic of myopia. The expanding evidence base supporting low-dose atropine and contact lens options, such as MCSCLs and ortho-k lenses, highlights the importance of co-management between ophthalmologists and optometrists. By fostering collaboration and aligning treatment protocols, we can enhance patients' outcomes and more effectively address the wide prevalence of myopia.
We hope that this position statement will serve as a guidance to our colleagues and can be adapted suitably across diverse practices. Since the availability of different MCSCLs or ortho-k lenses is dependent on local regulatory approval, it may be useful to more comprehensive country-level assessments to further understand the prescription patterns and barriers to large-scale adoption of MCSCLs or ortho-k lenses for controlling myopia. Local guidelines may need to be formulated to address the specific needs of ECPs in a particular country.
-
A potential limitation of the consensus recommendations presented in this position statement is the relatively small sample size of the survey participants and the expert panel, which precluded a meaningful evaluation of statistical significance; as such, the survey's results and the responses to the consensus statements have been summarized descriptively. However, the roundtable discussion comprised regional thought leaders in childhood myopia in APAC, who provided valuable insights on standardizing clinical practice for controlling myopia. This position statement represents the clinical experience of ECPs within the APAC region and may not be representative of global clinical experience. However, the consensus recommendations presented here are intended to function as a guide and reflect the current literature and clinical experience, thereby requiring modification with the emergence of new evidence.
-
The data presented in this manuscript comprise aggregated survey responses and expert opinions obtained from participants in an in-person advisory board meeting. No human or animal subject research was conducted for the purposes of this publication. Accordingly, approval from an institutional review board or independent ethics committee was not applicable.
-
The authors confirm their contributions to the paper as follows: conceptualization, methodology and writing—original draft preparation: Foo LL, Song T; resources, project administration and funding acquisition: Song T; writing—review and editing: Foo LL, Baek SH, Choy EPY, Hsu CYY, Lumb E, Lee HJ, Gifford K, Koh LB, Lee KL, Li J, Liang CK, Abdul Rahim MAS, Ng WY, Matsumura S, Tan TC, Toh D, Woon PS, Song T. All authors reviewed the results and approved the final version of the manuscript.
-
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
-
The authors would like to express their gratitude to Liu IT for her active participation and contribution to the roundtable discussion. The authors would also like to recognize the efforts of the survey respondents for their responses and insights. This study was funded by CooperVision Singapore Pte Ltd.
-
Foo LL is a researcher at the Singapore National Eye Centre/Singapore Eye Research Institute, Singapore and received funding from CooperVision to conduct this study. Song T is a postgraduate researcher at the School of Optometry, Aston University, Birmingham, United Kingdom, and is employed by CooperVision. Lumb E is employed by CooperVision. Gifford K has received funding or honoraria for education, research, travel, lecturing, or authorship from Alcon, CooperVision, EssilorLuxottica, Hoya, Johnson & Johnson, Menicon, Oculus, Ocumetra, Eyerising International, Seed, Sight Glass Vision, and Topcon Healthcare. These authors hereby declare that although the above relationships exist, their work in this study, including data analysis and manuscript preparation, was conducted independently and was not influenced by any interests, ensuring objectivity and impartiality. The remaining authors declare that they have no conflict of interest.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Foo LL, Gifford K, Baek SH, Choy EPY, Hsu CYY, et al. 2026. Joint position statement on standardizing the clinical use of contact lenses for myopia control from ophthalmology and optometry practices in the Asia-Pacific region. Visual Neuroscience 43: e013 doi: 10.48130/vns-0026-0009 

Joint position statement on standardizing the clinical use of contact lenses for myopia control from ophthalmology and optometry practices in the Asia-Pacific region
- Received: 05 September 2025
- Revised: 21 January 2026
- Accepted: 21 January 2026
- Published online: 26 March 2026
Abstract: The increasing prevalence of myopia in Asia is a public health concern, necessitating prompt control strategies because of its progressive nature and long-term consequences for vision. Despite demonstrating efficacy, convenience, and a positive lifestyle impact, myopia control contact lenses are not widely used. Standardized guidelines on the use of myopia control soft contact lenses (MCSCLs) and orthokeratology (ortho-k) lenses enable eye care professionals (ECPs) to achieve maximum potential for childhood myopia control. An expert panel of ECPs from the Asia-Pacific region was convened to examine prescribing behaviors, identify areas for improvement, and advance the discussion on myopia control contact lens usage. An online survey conducted among ECPs across Chinese Taipei (China), Hong Kong SAR (China), Japan, Malaysia, Singapore, and South Korea gathered insights on current practices, challenges, and preferences. The expert panel discussed the survey's results and deliberated on acceptable practices in a roundtable meeting in Kuala Lumpur. Recommendations for guiding patient selection, the fitting process, follow-up schedules, and treatment outcomes for MCSCLs and ortho-k lenses were proposed. This position statement reports these recommendations and related consensus statements on incorporating MCSCLs and ortho-k lenses into clinical practice in Asia to improve myopia control outcomes and long-term ocular health in Asian children.
-
Key words:
- Myopia /
- Myopia control /
- Childhood myopia /
- Soft contact lenses /
- Orthokeratology