-
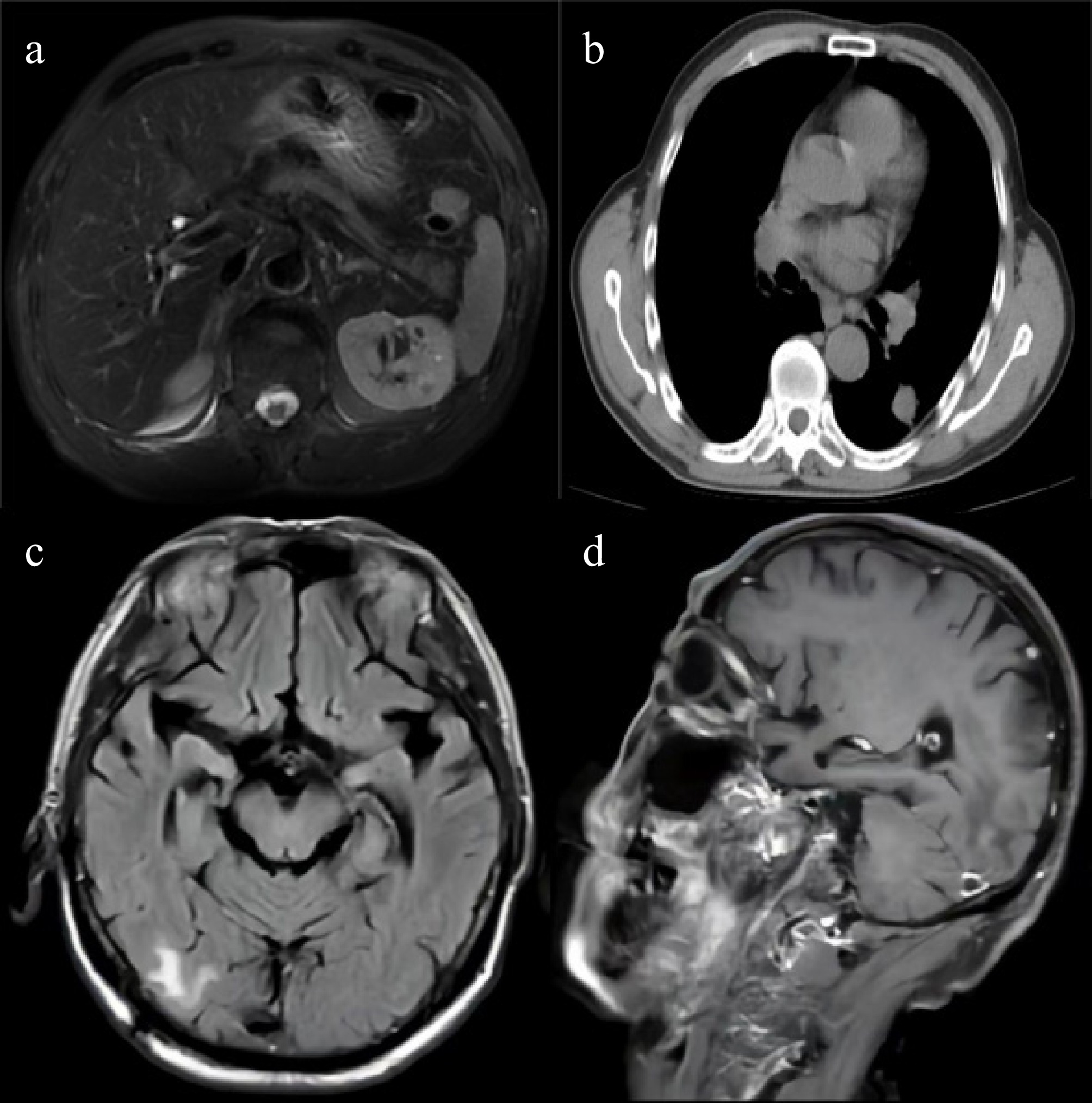
Figure 1.
Cross-sectional contrast-enhanced imaging of the patient. (a) Contrast-enhanced MR of the liver: images show hypervascular nodules near the inferior vena cava in segment VIII and in segment VII, primarily considered early hepatocellular carcinoma (eHCC). (b) Contrast-enhanced CT of the chest: images reveal a nodule in the left lower lobe, multiple lymph nodes in the left neck, supraclavicular area, mediastinum, and left pulmonary hilum, and osteolytic destruction of the left scapula, primarily suggesting pulmonary malignancy with metastases. (c) Contrast-enhanced MR of the brain: Images demonstrate multiple enhancing nodules in the brain, with metastasis as the primary consideration. (d) Contrast-enhanced MR of the brain: images show multiple enhancing nodules in another region of the brain.
-
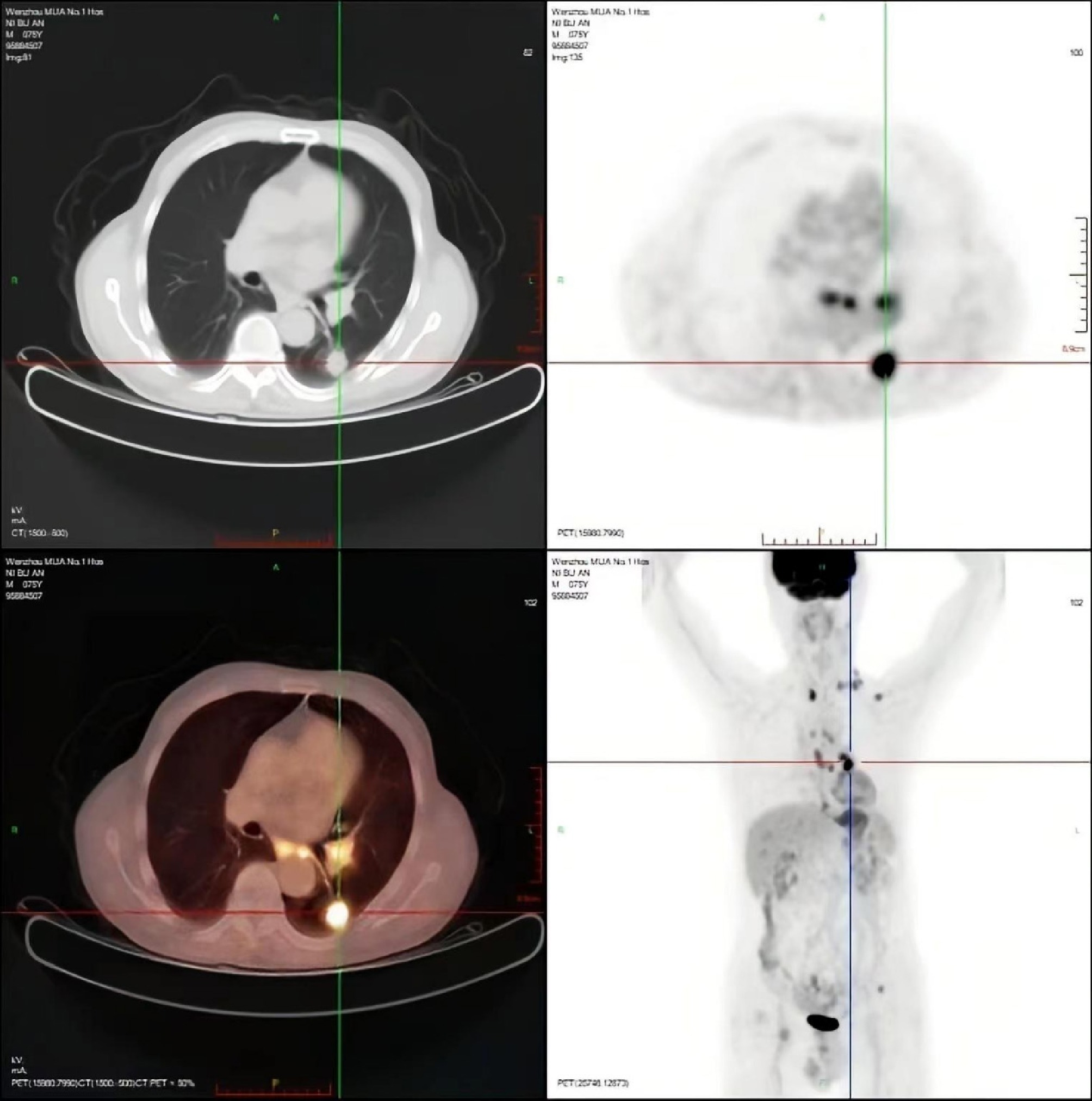
Figure 2.
PET-CT evaluation. (a) PET maximum intensity projection (MIP) whole-body image: shows multiple hypermetabolic foci in the left lower lung, multiple lymph node stations, brain (left frontal and right temporal lobes), left scapula, and left ilium, suggesting malignant metastases. (b) Fused PET/CT image of the chest: corresponds to Fig. 1b, confirming hypermetabolism in the left lower lung nodule and mediastinal lymph nodes. (c) Fused PET/CT image of the abdomen: corresponds to Fig. 1a, shows residual increased metabolism in the hepatic nodules (segments VII and VIII), suggesting residual tumor activity post-treatment. (d) Fused PET/CT image of the brain: corresponds to Fig. 1c, d, reveals hypermetabolic small nodules in the brain (left frontal and right temporal lobes).
-
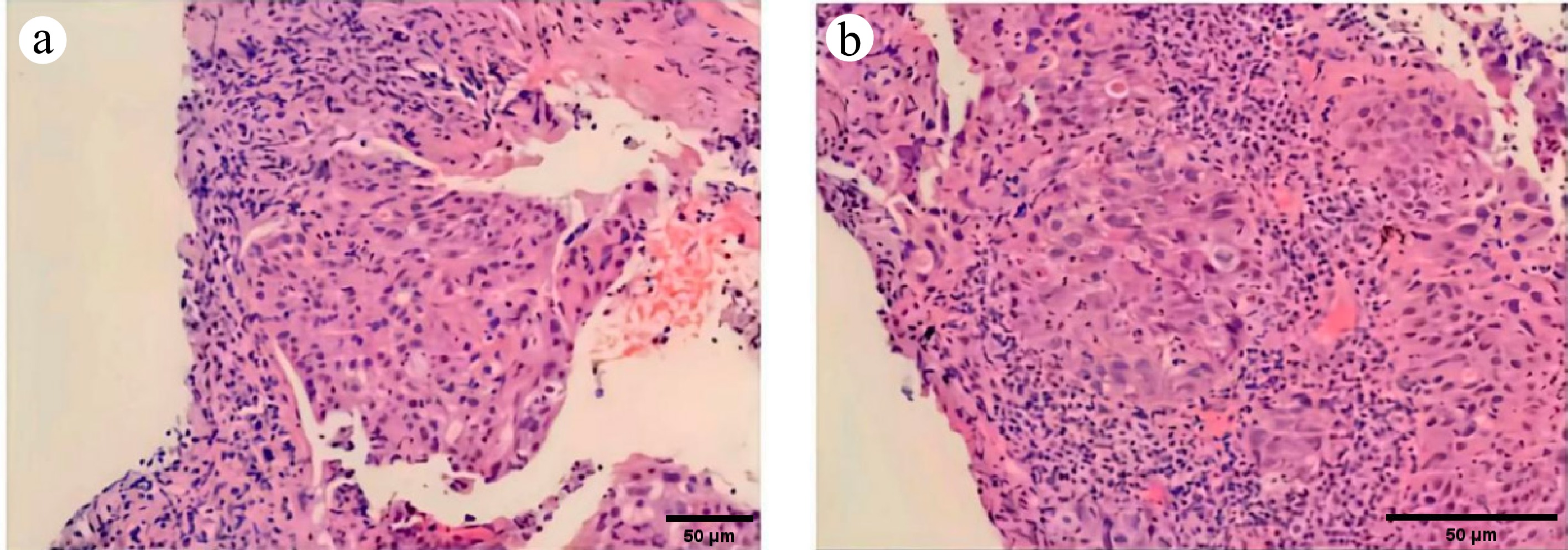
Figure 3.
Histopathological images of the lung metastasis biopsy: (a) 100×, (b) 200×. H & E-stained micrograph: shows the tumor tissue and the morphology of tumor cells.
-
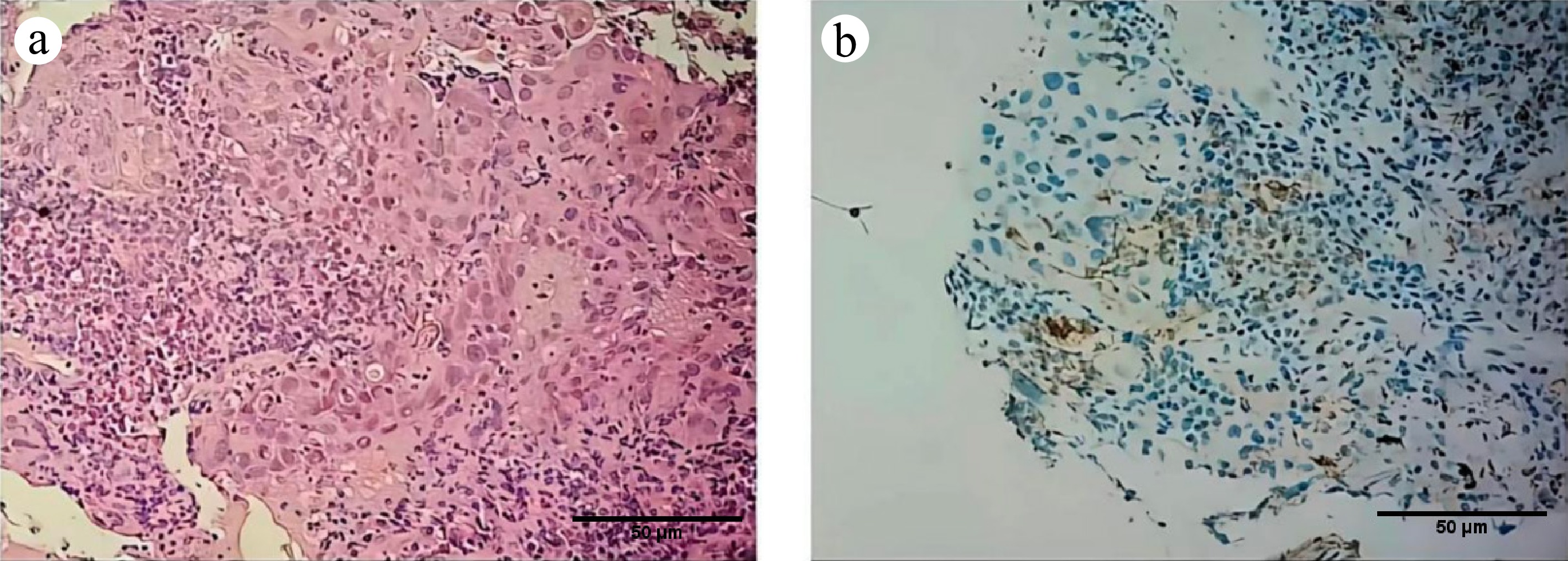
Figure 4.
Supplementary pathological examination of the lung metastasis: (a) 200×, (b) 200×. H & E-stained micrograph: shows the morphology of the tumor area.
-
Antibody Result Staining intensity/extent Notes/significance Hepatocytic markers HepPar-1 Positive Diffuse strong positivity (> 80%) Confirms hepatocellular origin GPC-3 Focally positive ~30% of cells, moderate intensity Supports HCC diagnosis SMARCA4/BRG1 Negative Complete loss of nuclear staining in tumor cells Key diagnostic finding Proliferation index Ki-67 High ~60% nuclear positivity in tumor cells Indicates high proliferative activity Immune checkpoint PD-L1 (Clone E1L3N) Low expression TPS = 10% Epithelial and differential diagnosis markers CK7 Partially positive ~40% of cells positive CK19 Positive Diffuse positivity TTF-1 Negative 0% Rules out lung adenocarcinoma Napsin A Negative 0% Rules out lung adenocarcinoma P40 Negative 0% Rules out squamous cell carcinoma CK5/6 Negative 0% Rules out squamous cell carcinoma Table 1.
Immunohistochemical profile of the lung metastasis biopsy.
-
Category Details Demographics Age/sex 75-year-old male Chief complaint and history Admitted due to 'discovered pulmonary space-occupying lesions over one week after TACE therapy for liver malignancy' Physical examination on admission Conscious, fair general condition. Vital signs: T 37 °C, BP 120/79 mmHg, P 57 bpm, R 18 bpm, SpO2 97%. No jaundice. No palpable superficial lymphadenopathy. Clear breath sounds bilaterally without rales. Soft abdomen, no tenderness, liver and spleen not palpable below the costal margin. No pitting edema in lower limbs. Neurological examination normal Imaging findings Liver MRI Residual enhancing nodules in liver segments S7 and S8, suggesting residual tumor post-TACE Chest CT Nodule in the left lower lobe; widespread lymphadenopathy Brain MRI Multiple enhancing nodules throughout the brain, consistent with metastases Whole-body PET-CT Intense hypermetabolism in the liver lesions, left lung nodule, lymph nodes, bones, and brain, confirming multifocal metastatic disease Pathological diagnosis (lung biopsy) Histology (H&E) Poorly differentiated malignant tumor. Cells arranged in sheets and irregular nests, with hyperchromatic nuclei, high nuclear-to-cytoplasmic ratio, eccentric nuclei, and focally eosinophilic cytoplasm. Necrosis present Immunohistochemistry Positive markers: Hepatocyte(+), GPC-3 (focal+), CK7 (partial+), CK19 (+);
Negative markers: TTF-1 (−), Napsin-A (−), P40 (−), CK5/6 (−);
Crucial finding: SMARCA4/BRG1 (−/loss of expression);
Proliferation index: Ki-67 (approx. 60%+);
PD-L1 (Clone E1L3N): TPS = 10%Final diagnosis Metastatic SMARCA4-deficient hepatocellular carcinoma Treatment Lenvatinib (a multi-kinase inhibitor) combined with Atezolizumab (an anti-PD-L1 immune checkpoint inhibitor) Outcome Disease progressed rapidly despite combination therapy. Patient survival was approximately one year from diagnosis Table 2.
Summary of clinical, pathological, and treatment characteristics of the patient with SMARCA4-deficient hepatocellular carcinoma.
Figures
(4)
Tables
(2)