-
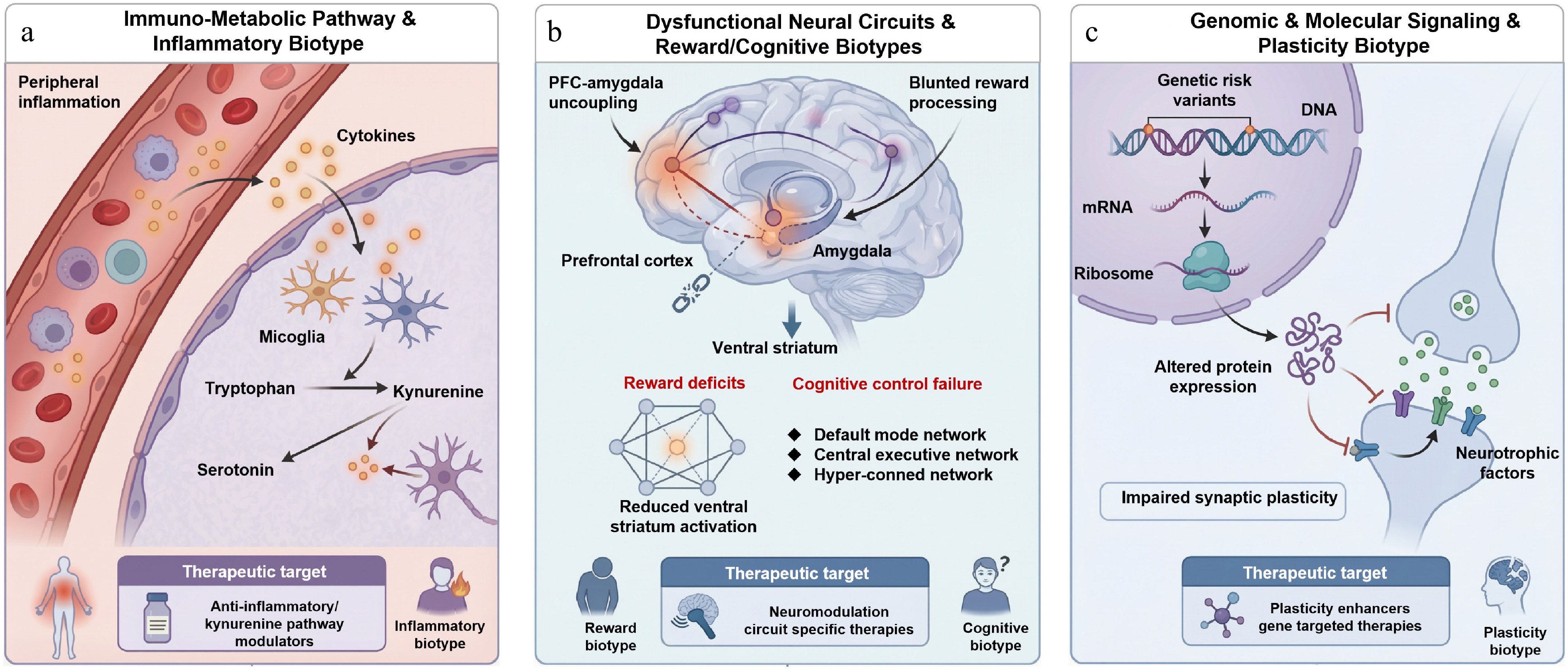
Figure 1.
Integrated biological biotypes of depression and their underlying mechanistic pathways. (a) Immuno-metabolic/inflammatory biotype, where peripheral inflammation drives microglial activation, and shifts tryptophan metabolism toward neurotoxic kynurenine metabolites, reducing serotonin; (b) neural circuit/reward-cognitive biotype, characterized by disrupted prefrontal amygdala connectivity, blunted ventral striatum response, and impaired default mode executive network interactions; and (c) genomic/plasticity biotype, marked by genetic risk variants that impair neurotrophic signaling and synaptic plasticity. Each biotype maps to specific therapeutic strategies, anti-inflammatory/kynurenine modulators, circuit targeted neuromodulation, and plasticity enhancing agents, respectively, illustrating a mechanism-based framework for precision treatment in depression.
-
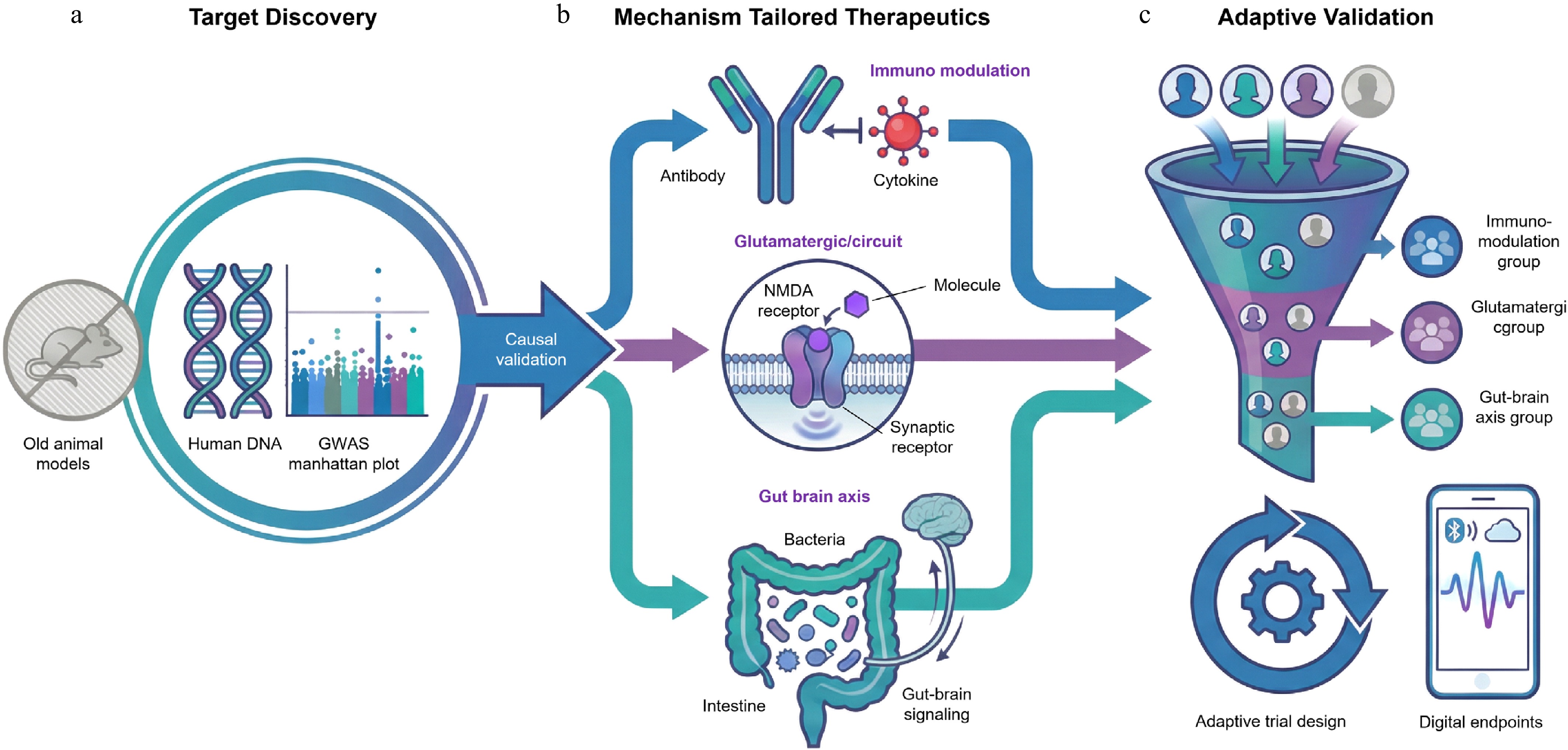
Figure 2.
The paradigm shifts toward precision drug development in depression. This framework illustrates the transition from empirical screening to a mechanism based approach across three stages: (a) human-anchored discovery, where large scale genomics (GWAS) and Mendelian randomization replace traditional animal models to identify causally valid targets; (b) mechanism tailored therapeutics, developing specific agents for distinct biotypes, such as anti-inflammatory biologics, rapid acting glutamatergic modulators, and microbiome interventions; and (c) next-generation evidence generation, utilizing biomarker enriched adaptive platform trials and digital endpoints to efficiently validate efficacy in specific patient subgroups.
-
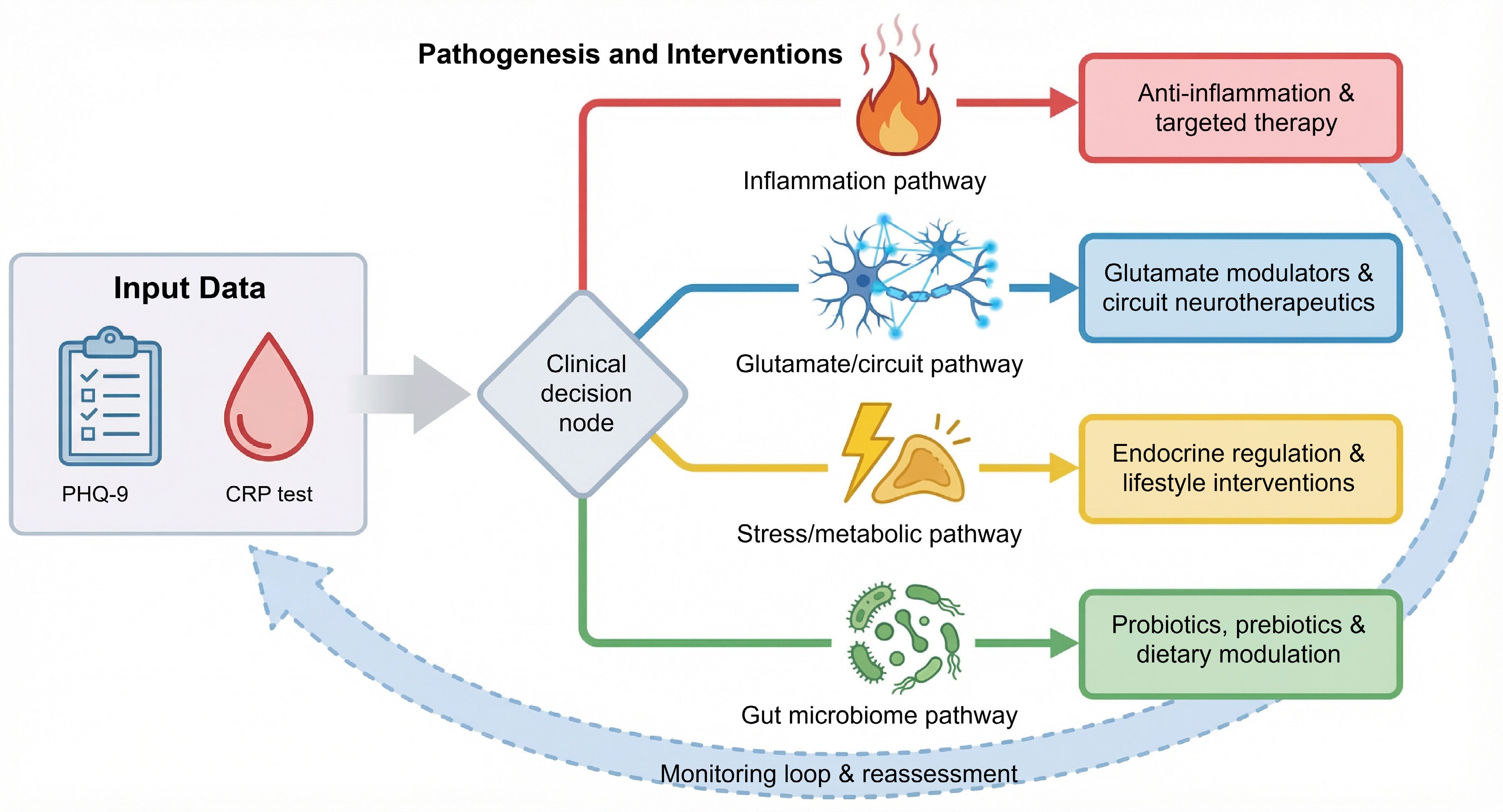
Figure 3.
Mechanism-based clinical decision framework for precision treatment in depression.
-
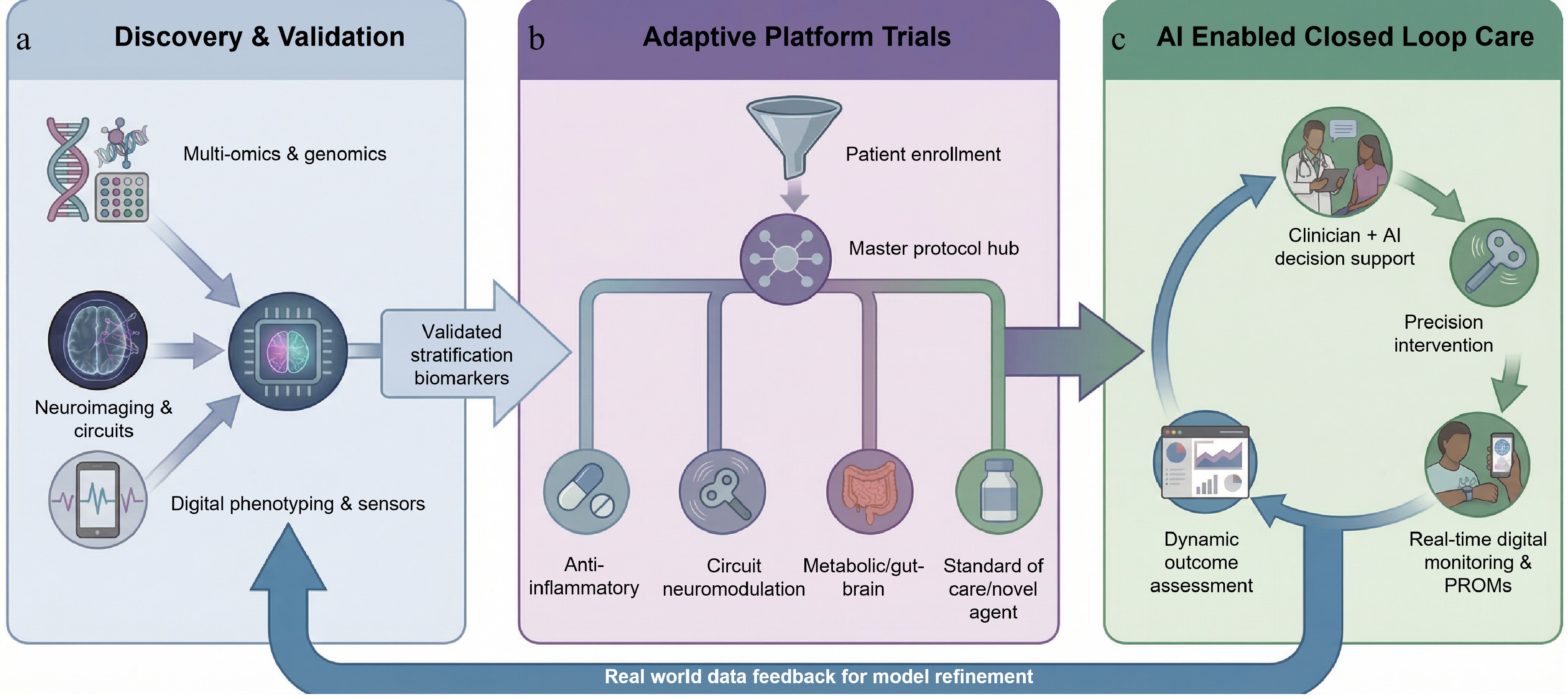
Figure 4.
An integrated roadmap for a precision psychiatry ecosystem. This framework illustrates the translational pathway from; (a) discovery and validation, where multi-omics and digital data inform AI-driven biotype identification; to (b) adaptive platform trials, utilizing master protocols to dynamically assign patients to mechanism-based treatments; and finally to (c) AI enabled closed loop care, where real-world clinical outcomes continuously refine predictive models, creating a learning health system that bridges research and clinical practice.
-
Category Key approach/method Main finding or contribution Implication for MDD Ref. Multi-omics and
causal inferenceMitochondrial multi-omics integration Identified mitochondrial-related causal genes for MDD Links cellular energetics to depression pathogenesis [74] Gut microbiome + metabolomics Revealed bacterial/metabolic signatures in MDD Supports gut-brain axis as therapeutic target [75] Proteome-transcriptome integration (brain/blood) Prioritized causal genes for depression Enables cross-tissue biomarker discovery [81] Single-nucleus ATAC-seq Mapped chromatin accessibility in MDD-relevant cell types Identifies regulatory variants in excitatory neurons [82] Bulk and single-nucleus transcriptomics Convergent synaptic dysregulation in excitatory neurons Highlights shared molecular pathology across cohorts [83] Cross-disorder systems biology (MDD/PTSD) Shared and distinct molecular signatures across brain regions Suggests transdiagnostic mechanisms [84] Two-sample Mendelian randomization IL-6 and plasma proteins causally linked to MDD Validates immune-inflammatory pathway as causal [78,79] Digital phenotyping and AI Graph neural networks on fMRI Detected functional connectivity features of MDD Offers data-driven neuroimaging biomarkers [77] Survey of ML/DL in psychiatry Reviewed AI applications in depression detection/treatment Maps current landscape of computational psychiatry [50] Smartphone/wearable digital phenotyping Demonstrated feasibility of passive mood monitoring Enables real-time symptom tracking [50,85] Wearable sensors + ML modeling Predicted depression severity from behavioral data Supports scalable screening tools [86,87] Retrospective mHealth analysis Highlighted challenges in data quality/prediction Calls for standardized digital biomarker validation [88] Novel therapeutics Preclinical/clinical review Ketamine may benefit TRD in Alzheimer's/elderly Expands ketamine's applicability beyond typical TRD [89] fMRI + glutamate spectroscopy Linked S-ketamine's acute network effects to delayed glutamate changes Clarifies mechanism of rapid-acting antidepressants [90] KOR antagonist (anticipant) in UCMS mice Reversed stress-induced depressive behaviors Supports kappa opioid system as drug target [91] Precision psychiatry and EHR EHR-based stratification Showed EHR can enable patient subtyping and treatment prediction Bridges real-world data to precision care [92,93] Pharmacogenomics + CDS in EHR Implemented PGx-guided prescribing with clinical impact Proves feasibility of genomic medicine in psychiatry [94−96] Patient-centered care and equity Decision aids for depression/TRD Improved shared decision-making in RCTs Enhances patient autonomy in complex treatment choices [97,98] Conceptual framework Argues for 'person-centered' over purely biological precision psychiatry Calls for integrating lived experience [99] Health equity frameworks Highlight disparities in genomic/
digital mental health accessUrges inclusive design and intersectional research [100−102] Detection and prediction DNA methylation risk scores (MRS) MRS significantly discriminated MDD cases from controls Enhancing MDD prediction from PRS and environmental traits [103] Examine surrogate measures of insulin resistance Three measures positively predicted incident MDD in a 9-year follow-up period Useful for evaluating the risk of MDD among patients with metabolic pathology [104] Machine learning to identity multivariate MDD biomarkers Mean accuracies for diagnostic classification ranged between 48.1% and 62.0% Improved predictive capability compared with univariate neuroimaging markers [105] Volatile organic compounds (VOCs) from breath 76.8% accuracy to distinguish MDD patients from healthy controls Promising for use of biomarkers in gas samples of human breath as a diagnostic measure [106] Table 1.
Recent advances in major depressive disorder research: multi-omics, digital phenotyping, and precision psychiatry approaches.
Figures
(4)
Tables
(1)