







-
Major depressive disorder (MDD) stands as one of the most devastating conditions faced globally, wreaking havoc on patients' emotional lives, thinking abilities, relationships, and basic daily functioning[1,2]. Despite advances in the diagnosis and treatment of depression over recent decades, major gaps remain in both mechanistic understanding and clinical effectiveness[3−7]. Current diagnostic systems like the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5, published by the American Psychiatric Association) and the International Classification of Diseases, 11th Revision (ICD-11, issued by the World Health Organization) provide a shared clinical language. However, they are built around observable symptoms rather than the underlying biological complexity that actually drives this disorder[8−11].
The central limitation is that current diagnostic criteria are fundamentally descriptive rather than mechanistic. DSM-5 requires at least five symptoms from a checklist, lasting two weeks or more, with either low mood or loss of interest being present[10,12,13]. In practice, this diagnostic framework allows for hundreds of different symptom combinations to meet criteria for the same diagnosis[14,15]. As a result, patients with identical diagnoses might have completely different biological problems driving their depression. Increasing evidence supports the view that MDD is a heterogeneous syndrome rather than a single disease entity[16−18]. This creates a real headache for researchers trying to find biological markers, because they end up averaging across what are likely distinct disease processes, which makes it nearly impossible to find clear signals[19−22].
The dominant therapeutic paradigm has evolved only marginally from its mid-20th century origins. The monoamine hypothesis, formulated in the 1950s, remains influential in clinical practise and continues to guide first-line pharmacotherapy targeting serotonin, norepinephrine, and dopamine systems[23,24]. This led to the development of selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs), which continue to constitute the cornerstone of first-line agents[25−28]. However, treatment responses vary wildly among patients, and clinical benefit often emerges only after 4–8 weeks[26,29,30]. This delayed onset strongly implies that these agents may modulate downstream neurobiological changes rather than directly addressing primary etiological drivers. Real-world data show that only 30%–40% of patients achieve remission after their first antidepressant trial. Among patients with treatment-resistant depression, 50%–67% still do not experience adequate relief despite multiple treatment attempts[6,31−33]. Some medications like duloxetine have a Number Needed to Treat (NNT) of nine, indicating that a substantial proportion of treated patients experience side effects and delayed symptom relief without meaningful benefit beyond placebo[29,34,35].
More fundamentally, the current framework fails to recognize depression as a whole-body, multi-system disorder[36,37]. Evidence increasingly indicates that MDD involves complex, interconnected disruptions across brain circuits, hormone systems, immune function, metabolism, gut bacteria, and social environment[37−39]. Approximately 30% of patients show chronic low-grade inflammation with elevated markers such as C-reactive protein (CRP) and IL-6. This inflammation correlates with specific symptoms, particularly loss of pleasure and cognitive problems, and predicts poor response to standard antidepressants[31,40−42]. Other subgroups show disrupted stress hormone systems, cellular energy problems, altered gut microbes, and changes in gene expression[43−45]. Yet despite all this evidence, routine clinical practice rarely incorporates any objective biological measures, and treatment decisions remain largely disconnected from mechanistic understanding[36,44].
In addition, clinical monitoring is another unmet need. The current clinical framework lacks good ways to monitor how patients are doing over time and adjust treatments accordingly based on their ongoing response patterns[46,47]. Follow-up visits still rely mainly on patients' subjective reports, which can miss clinically important changes in symptom severity[48]. New technologies like digital monitoring platforms, wearable sensors, and genetic testing for drug metabolism show real promise, but they are barely being used in routine clinical practice yet[49−53].
Collectively, these limitations indicate the need to move beyond symptom-based categories toward mechanism-informed diagnosis and treatment. This means developing what researchers call precision psychiatry, an approach rooted in the principles of precision medicine. While often used interchangeably with personalized medicine, precision psychiatry is distinct: it does not aim to create unique treatments for each individual, but rather leverages multimodal data such as genetic, imaging, immunological, and metabolic data to stratify patients into biologically defined subgroups that share a common disease mechanism. This stratification enables more targeted and effective interventions than the current one-size-fits-all approach, moving beyond the descriptive categories of traditional psychiatry by linking specific pathophysiological pathways to tailored treatments[16,54]. In this context, artificial intelligence (AI) and machine learning show particular promise here, offering ways to identify biologically meaningful subtypes, predict which treatments will work for whom, and potentially enable real-time treatment adjustments[50,55]. This review summarizes key advances enabling this transition and provides both the conceptual foundation and practical considerations for implementing truly mechanism based, individualized depression care.
-
Over the past decade, MDD research has been moving away from symptom-based classification and toward stratifying patients by underlying mechanisms (Table 1). The goal here is to identify biotypes (such as monoamine neurotransmitter imbalance, abnormal neural plasticity, dysregulation of the HPA axis and stress system, inflammation and immune activation, abnormal neural circuits, and brain networks, genetic and epigenetic factors, imbalance of glutamate/GABA and other excitatory-inhibitory systems, circadian rhythm and sleep mechanism abnormalities, gut-brain axis, and metabolic factors), (Fig. 1), that reflect shared pathophysiological pathways and can inform treatment selection[56−58]. This shift depends on a more nuanced grasp of the multisystem origins of MDD, and recent advances in high-dimensional data capture, multi-omics platforms, and AI-powered analytics. Together, these developments support subtype identification that is more flexible and clinical informative than traditional categorical approaches[50,59].
Table 1. Recent advances in major depressive disorder research: multi-omics, digital phenotyping, and precision psychiatry approaches.
Category Key approach/method Main finding or contribution Implication for MDD Ref. Multi-omics and
causal inferenceMitochondrial multi-omics integration Identified mitochondrial-related causal genes for MDD Links cellular energetics to depression pathogenesis [74] Gut microbiome + metabolomics Revealed bacterial/metabolic signatures in MDD Supports gut-brain axis as therapeutic target [75] Proteome-transcriptome integration (brain/blood) Prioritized causal genes for depression Enables cross-tissue biomarker discovery [81] Single-nucleus ATAC-seq Mapped chromatin accessibility in MDD-relevant cell types Identifies regulatory variants in excitatory neurons [82] Bulk and single-nucleus transcriptomics Convergent synaptic dysregulation in excitatory neurons Highlights shared molecular pathology across cohorts [83] Cross-disorder systems biology (MDD/PTSD) Shared and distinct molecular signatures across brain regions Suggests transdiagnostic mechanisms [84] Two-sample Mendelian randomization IL-6 and plasma proteins causally linked to MDD Validates immune-inflammatory pathway as causal [78,79] Digital phenotyping and AI Graph neural networks on fMRI Detected functional connectivity features of MDD Offers data-driven neuroimaging biomarkers [77] Survey of ML/DL in psychiatry Reviewed AI applications in depression detection/treatment Maps current landscape of computational psychiatry [50] Smartphone/wearable digital phenotyping Demonstrated feasibility of passive mood monitoring Enables real-time symptom tracking [50,85] Wearable sensors + ML modeling Predicted depression severity from behavioral data Supports scalable screening tools [86,87] Retrospective mHealth analysis Highlighted challenges in data quality/prediction Calls for standardized digital biomarker validation [88] Novel therapeutics Preclinical/clinical review Ketamine may benefit TRD in Alzheimer's/elderly Expands ketamine's applicability beyond typical TRD [89] fMRI + glutamate spectroscopy Linked S-ketamine's acute network effects to delayed glutamate changes Clarifies mechanism of rapid-acting antidepressants [90] KOR antagonist (anticipant) in UCMS mice Reversed stress-induced depressive behaviors Supports kappa opioid system as drug target [91] Precision psychiatry and EHR EHR-based stratification Showed EHR can enable patient subtyping and treatment prediction Bridges real-world data to precision care [92,93] Pharmacogenomics + CDS in EHR Implemented PGx-guided prescribing with clinical impact Proves feasibility of genomic medicine in psychiatry [94−96] Patient-centered care and equity Decision aids for depression/TRD Improved shared decision-making in RCTs Enhances patient autonomy in complex treatment choices [97,98] Conceptual framework Argues for 'person-centered' over purely biological precision psychiatry Calls for integrating lived experience [99] Health equity frameworks Highlight disparities in genomic/
digital mental health accessUrges inclusive design and intersectional research [100−102] Detection and prediction DNA methylation risk scores (MRS) MRS significantly discriminated MDD cases from controls Enhancing MDD prediction from PRS and environmental traits [103] Examine surrogate measures of insulin resistance Three measures positively predicted incident MDD in a 9-year follow-up period Useful for evaluating the risk of MDD among patients with metabolic pathology [104] Machine learning to identity multivariate MDD biomarkers Mean accuracies for diagnostic classification ranged between 48.1% and 62.0% Improved predictive capability compared with univariate neuroimaging markers [105] Volatile organic compounds (VOCs) from breath 76.8% accuracy to distinguish MDD patients from healthy controls Promising for use of biomarkers in gas samples of human breath as a diagnostic measure [106] 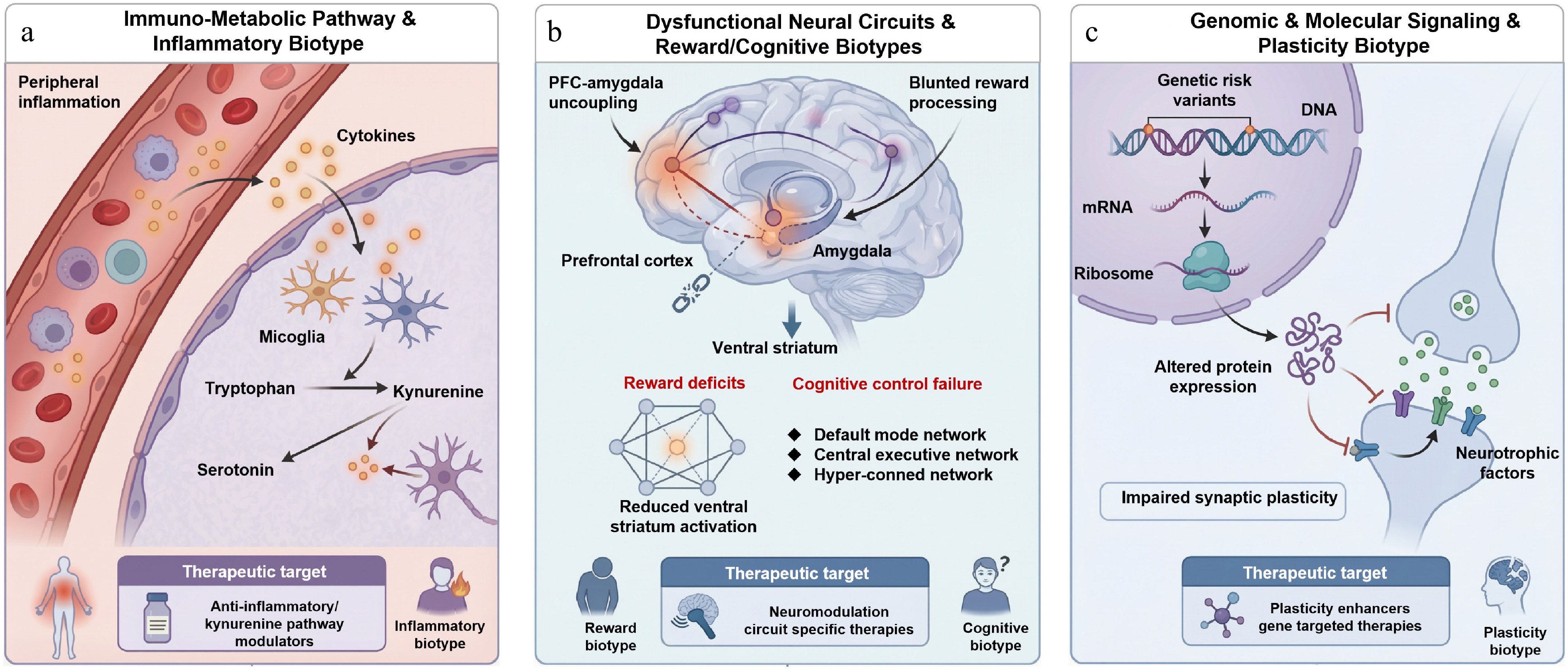
Figure 1.
Integrated biological biotypes of depression and their underlying mechanistic pathways. (a) Immuno-metabolic/inflammatory biotype, where peripheral inflammation drives microglial activation, and shifts tryptophan metabolism toward neurotoxic kynurenine metabolites, reducing serotonin; (b) neural circuit/reward-cognitive biotype, characterized by disrupted prefrontal amygdala connectivity, blunted ventral striatum response, and impaired default mode executive network interactions; and (c) genomic/plasticity biotype, marked by genetic risk variants that impair neurotrophic signaling and synaptic plasticity. Each biotype maps to specific therapeutic strategies, anti-inflammatory/kynurenine modulators, circuit targeted neuromodulation, and plasticity enhancing agents, respectively, illustrating a mechanism-based framework for precision treatment in depression.
The rise of biological biotypes
-
Early efforts to stratify MDD patients relied on single biomarkers like serum cortisol, CRP, or brain-derived neurotrophic factors (BDNF). While these flagged certain subgroups, such as inflammatory depression or HPA axis overactivity, they provided limited explanatory power due to their neglect of interactions across biological systems[31,41,60,61]. The real turning point came when researchers started combining data types. Drysdale et al. used resting state functional magnetic resonance imaging (fMRI) alongside machine learning to pinpoint four reproducible neural circuit biotypes in MDD, each with its own prefrontal limbic connectivity signature, and each predicting whether patients would respond to transcranial magnetic stimulation (TMS)[62]. In parallel, other groups built MDD models that pulled together inflammation, metabolism, and neuroendocrine activity, sorting patients into categories like high inflammation/insulin resistant, HPA axis hyperactive, or autonomic dysregulated, and each subtype (typically a category defined by clinical, biological, or combined features) responded differently to factors like anti-inflammatories, lifestyle interventions, or glucocorticoid modulators[63,64]. These studies support a model in which MDD comprises overlapping yet distinguishable biological syndromes. For clinical utility, such subtypes must be linked to reproducible mechanisms, measurable markers, and actionable treatment strategies[21,65,66].
From discrete categories to continuous dimensions
-
The concept of continuous subtyping is increasingly replacing traditional discrete classification[67−69]. The mechanisms driving MDD do not fit neatly into separate boxes; however, they are better thought of as existing along multiple sliding scales, such as inflammatory load, neural plasticity, stress reactivity, microbiome diversity, monoamine system integrity, and so on[56,70,71]. In this model, every patient becomes a point in multidimensional space, positioned according to how much each mechanism contributes to their condition. For example, patients with high neuroinflammatory activity but normal monoamine function (normal CSF 5-HIAA) may plausibly benefit more from immune-targeted interventions than from SSRIs alone[70]. Patients with pronounced glutamatergic dysfunction and severe anhedonia may be more likely to respond to ketamine or similar agents[68,72]. This dimensional approach not only maps onto biology more accurately, but it also gives clinicians a quantitative framework for matching treatments to patients. It sidesteps the awkwardness of forcing people into mutually exclusive boxes and acknowledges what we see all the time in practice; mixed presentations are the norm, not the exception[16,56].
Multi-omics integration and AI-driven subtyping
-
The core technologies driving the transition toward mechanism-based, multidimensional patient stratification in depression are multi-omics integration and machine learning[73]. Combined analysis of genomic, epigenomic, transcriptomic, proteomic, metabolomic, and microbiomic data, which some call the six-omics layers, can reveal the full arc from genetic risk through environmental exposures to downstream physiological changes[49,74]. A multicenter study illustrates this nicely: researchers found that certain gut microbiota profiles (like depleted Faecalibacterium) correlated with disrupted plasma tryptophan metabolism (higher kynurenine-to-tryptophan ratios) and weaker functional connectivity in the anterior cingulate cortex, essentially defining a gut-brain axis subtype[75,76]. Modern algorithms, including graph neural networks and deep autoencoders can extract latent structures from heterogeneous datasets and support unsupervised or semi-supervised biotype discovery[50,77]. Causal inference tools such as Mendelian randomization and mediation analysis can help distinguish drivers from downstream correlates[74,78]. For example, Mendelian randomization studies have implicated IL-6 as causally contributing to MDD rather than just being a byproduct of the illness[31], strengthening the rationale for anti-inflammatory interventions in appropriately selected patients[79,80].
Digital phenotyping enables dynamic subtyping
-
Conventional subtyping provides a static profile and may miss fluctuations in symptoms and biology over time[88]. Digital phenotyping supports more dynamic stratification by enabling longitudinal, real-world measurement[85,107]. Smartphones and wearables can capture speech features, activity patterns, sleep metrics, and social interaction frequency, generating behavioral signatures that may change with treatment[86−88]. Someone with anhedonia-predominant depression might show sharply reduced activity and flatter speech, while an anxious patient could have fragmented sleep and low heart rate variability. Time-series models can flag these patterns as they emerge[55,107,108]. In the EMBARC (Establishing Moderators and Biosignatures of Antidepressant Response for Clinical Care) study, combining baseline fMRI with eight weeks of digital behavioral tracking yielded a dynamic prediction model that beat static baseline only models for forecasting long-term remission[109,110].
Challenges and future directions
-
Despite its promise, mechanism-based stratification faces challenges[111]. First, reproducibility across cohorts has been spotty, as many biotypes work well in specific populations or with one data type but do not generalize[56,111]. The next is about feasibility: multi-omics is expensive and slow, hardly practical for primary care[112]. Regulatory and ethical guardrails for AI-derived subtypes remain underdeveloped, including questions of validation, accountability, and clinical responsibility[113]. These issues require urgent attention[54]. A further layer of complexity arises from the frequent overlap and co-occurrence of multiple biotypes within the same individual. For example, a patient may simultaneously exhibit elevated inflammatory markers, disrupted prefrontal-amygdala connectivity, and reduced BDNF signaling. Such multimodal pathophysiology is not merely additive as it can create emergent interactions that confound treatment selection. Should clinicians prioritize anti-inflammatory agents, neuromodulation, or plasticity-enhancing drugs first? The lack of evidence on how to sequence or combine mechanism-targeted therapies in patients with mixed biotypes remains a major barrier to clinical implementation[62,114].
The path forward probably involves closed-loop precision care platforms. Imagine starting with baseline multi-omics, neuroimaging, and digital phenotyping to create a detailed biopsychosocial snapshot for each patient; using that profile to select targeted interventions such as anti-inflammatories, neuromodulation, probiotics, and cognitive training, then continuously adjusting based on real-time monitoring and feedback[49,115]. Early pilots are encouraging. For example, machine learning models have shown potential for predicting antidepressant response with impressive accuracy[116]. Making this scalable will require simpler biomarker approaches, like dried blood spots for CRP or salivary cortisol, and equity-minded design to ensure algorithms perform well across diverse populations, not just the groups they were trained on[117,118].
-
For three decades, antidepressant development has seen high failure rates and limited innovation[119]. Most new drugs amount to tweaks of existing monoaminergic compounds, and fewer than 10% succeed in clinical translation[25,120]. Contributing factors include simplified disease models and heavy reliance on animal experiments that do not really mirror human biology[121]. As the biological heterogeneity of MDD has become clearer, drug development has begun to shift towards approaches grounded in human genetics and mechanism-defined subgroups[122]. This transformation is reflected in three main trends: choosing targets validated by genetic data, designing therapies matched to the underlying biology, and running adaptive trials enriched with biomarker-defined patient subgroups[49,123].
Anchoring drug discovery in human biology
-
Traditional drug target selection leaned heavily on animal behavioral assays such as the forced swim test, which do not capture the cognitive and emotional complexity of human depression, so candidate drugs kept failing in human trials[83,124]. The newer strategy starts with large-scale human genetic data. Genome wide association studies have turned up hundreds of loci linked to MDD risk, pointing to pathways involved in synaptic plasticity (BDNF, DLG2), glutamate signaling (GRM7, GRIA3), immune function (IL6R, CRP), and stress reactivity[82,84] (Fig. 2). More crucially, Mendelian randomization can further test whether these targets are causally related to MDD rather than correlated, helping prioritize targets with stronger mechanistic support[125].
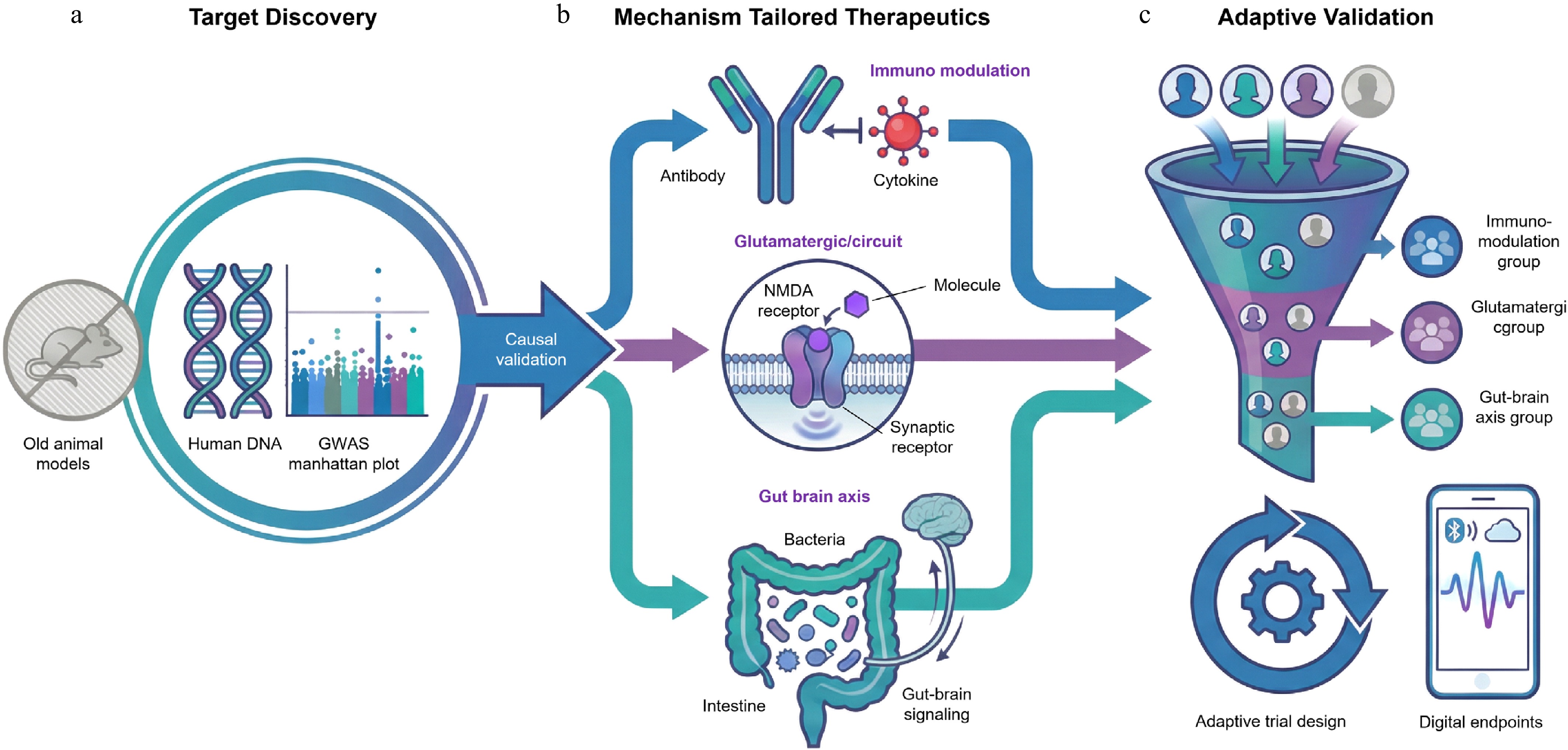
Figure 2.
The paradigm shifts toward precision drug development in depression. This framework illustrates the transition from empirical screening to a mechanism based approach across three stages: (a) human-anchored discovery, where large scale genomics (GWAS) and Mendelian randomization replace traditional animal models to identify causally valid targets; (b) mechanism tailored therapeutics, developing specific agents for distinct biotypes, such as anti-inflammatory biologics, rapid acting glutamatergic modulators, and microbiome interventions; and (c) next-generation evidence generation, utilizing biomarker enriched adaptive platform trials and digital endpoints to efficiently validate efficacy in specific patient subgroups.
Studies have shown that elevated IL-6 signaling genuinely raises MDD risk[31,126], motivating efforts to repurpose anti-inflammatory drugs for certain patients[126]. A randomized trial reported that tocilizumab (an IL-6 receptor blocker) significantly eased anhedonia and fatigue in MDD patients with baseline CRP above 3 mg·L−1, with minimal effects in the low inflammation group[126]. Another example is SLC6A15, a neuronal amino acid transporter associated with stress vulnerability and a smaller prefrontal cortex volume, making it an attractive target for neuroprotective drugs[127]. Overall, anchoring target selection in human causal genetics can improve the likelihood that experimental treatments address disease-relevant mechanisms[81].
From one-size-fits-all to mechanism-tailored therapeutics
-
The second pillar of precision drug development is biology-matched agents. Therapeutics designed, not for all patients with MDD, but for specific pathophysiological subtypes[122]. Glutamatergic modulators represent one mechanistic leap forward. Esketamine (S-ketamine), an NMDA receptor antagonist, has been approved by the FDA for treatment-resistant depression and works within hours rather than weeks like SSRIs[89]. It seems especially effective in patients with abnormal prefrontal glutamate/glutamine ratios or hyperconnectivity in the default mode network[90]. Similarly, kappa-opioid receptor (KOR) antagonists like CERC-501 are now in Phase II trials targeting patients with high stress reactivity or severe anhedonia, trying to prevent stress induced dopamine suppression[91].
Moreover, gut-brain axis targeted therapies are becomming fertile ground. Since gut microbiota dysbiosis and disrupted tryptophan metabolism appear central to certain MDD subtypes, researchers are testing targeted interventions, such as defined probiotic mixes, postbiotics, and even fecal microbiota transplantation as an add-on therapy[128]. A preliminary trial report shows improvements in gut microbial diversity and plasma kynurenine to tryptophan ratios alongside symptom reduction in selected patients[129,130]. Such examples demonstrate that future antidepressants will not be blunt instruments trying to lift the mood across the board, they'll be precise tools aimed at particular circuits or molecular pathways gone awry[131].
Redefining evidence generation
-
Even with a well-validated target and a biologically tailored drug, traditional trial designs with their broad inclusion criteria and rigid protocols will still wash out efficacy signals under a flood of patient heterogeneity. Thus, precision drug development requires precision trial designs to match[132,133].
Biomarker-enriched enrollment is one solution that only brings in patients who share the relevant underlying pathology[133]. For example, trials targeting p11-mediated signaling have used baseline p11 expression to enrich samples and improve response rates[133]. Similarly, the EMBARC platform uses fMRI connectivity patterns to identify a prefrontal amygdala decoupling subtype, which sharply improved their ability to predict who would respond to SSRIs[134].
Adaptive platform trials push this further. Instead of testing one drug at a time, these protocols run multiple investigational agents simultaneously under a shared framework, adjusting allocation ratios, doses, or target populations on the fly, based on accumulating data[135]. The EU-PEARL initiative used a Bayesian adaptive design to evaluate three mechanistically different agents in treatment-resistant depression all at once, dropping ineffective arms in real time and fast tracking promising ones into Phase III[135]. It is more efficient and arguably more ethical, since fewer patients end up on ineffective treatments.
Digital biomarkers are also being explored as trial endpoints. With the help of smartphones and wearable devices, passive collected behavioral data such as voice features, typing rhythms, and activity patterns can continuously and objectively reflect disease states and treatment responses in real-life environments[136,137]. In some studies, improvements in digital activity patterns occurred earlier than improvements in traditional scales (such as HAMD) scores, suggesting that these indicators may serve as early signals of treatment response[136]. In terms of regulation, regulatory agencies such as the FDA is accelerating the layout of digital health technologies, proposing frameworks and guidelines to explain how digital indicators can be used as biomarkers or clinical outcome indicators under a clear context of use. It is required to pass the technical and clinical validation as fit for purpose[138]. The key difficulties include: variations brought about by different devices and algorithm versions, data loss, and compliance issues in real environments, bias and generalizability of algorithms in different populations, and the need to prove that these digital indicators can correspond to existing endpoints (such as HAMD/PHQ 9) in terms of reliability, sensitivity to change, and clinical significance[137,139]. Therefore, at present, most regulatory authorities position digital endpoints as exploratory or secondary/supporting evidence. Only after strict pre-setting, standardization in advance, and continuous performance monitoring and full validation can they be accepted as registered primary endpoints[138,140].
Challenges and the path forward
-
Precision drug development for depression shows real promise, but faces persistent challenges. Multi-omics biomarker profiling remains expensive, regulatory frameworks have lagged in addressing complex interventions such as AI-guided drug combinations, and standardized tools for diagnosing biotypes are limited[54]. Getting past these hurdles will require: (1) building cheaper, scalable biomarker platforms, such as multiplexed protein assays from dried blood spots; (2) creating richly phenotyped, multi-institution biobanks where data and samples can actually be shared; and (3) pushing regulatory science forward so there are faster approval routes for mechanism-based therapies.
-
Mechanism-based patient stratification, targeted drug development, and multimodal biomarker research have built a solid scientific base for precision treatment of depression, but implementation in routine care remains difficult[141]. Effective translation requires an ecosystem that is scalable, sustainable, patient-centered, and equitably accessible[54,142]. Key components include robust and interpretable predictive models, closed-loop care systems that support longitudinal adaptation (Fig. 3), technology that integrates seamlessly into existing clinical workflows, and a sustained commitment to equity in access and performance[49].
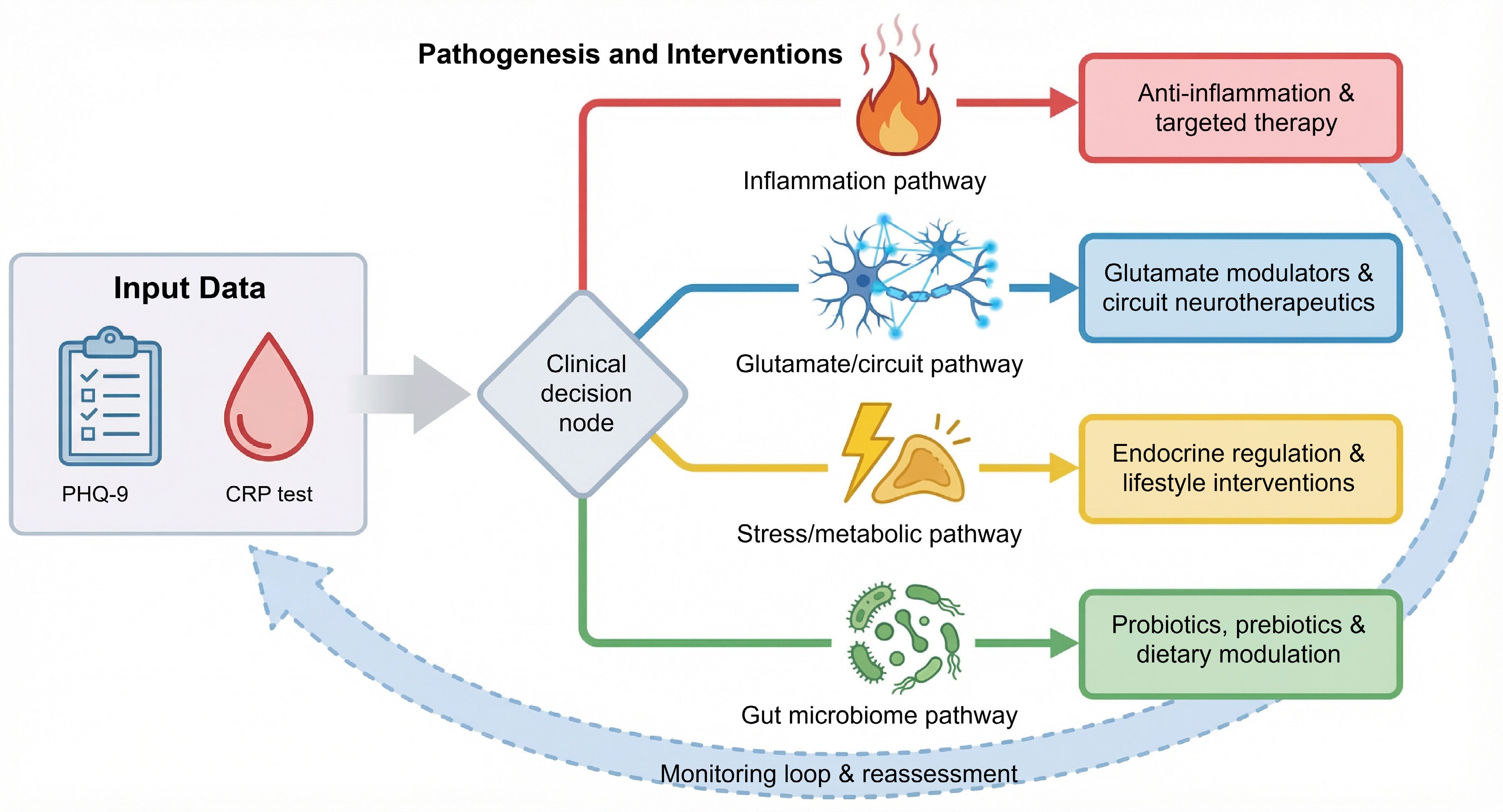
Figure 3.
Mechanism-based clinical decision framework for precision treatment in depression.
From research algorithms to clinically actionable predictive models
-
Plenty of machine learning models for predicting depression outcomes perform well in research settings, but hardly any have made it into routine use[143]. The usual culprits are insufficient external validation, distrust of black-box algorithms, expensive data collection, and a poor fit with existing electronic health record (EHR) systems[50,66,143]. To be clinically useful, models must be accurate, actionable, and usable in real time[144].
Some recent initiatives have moved toward this goal. The EMBARC consortium built a multimodal algorithm combining resting state fMRI, EEG, and blood inflammatory markers to predict SSRI response eight weeks out[66,109]. It hit an AUC of 0.78 and used circuit-level visualization to improve interpretability. The STARD*IT platform took a different route, pulling from real-world EHR data and pharmacogenomic profiles (CYP2D6/CYP2C19 metabolic types, for example) to create a decision support tool for choosing antidepressants, and in a prospective pilot, it increased initial remission rates by 22%[25,145].
However, deploying these models brings regulatory and ethical headaches. The FDA-issued AI/Machine Learning Software as a Medical Device (SaMD) Action Plan now requires algorithms to be transparent, robust, and capable of continuous learning[146,147]. Ideally, future prediction tools should work as clinical decision support systems embedded right in the EHR, presenting concise recommendations and clearly indicating the data elements supporting each output (e.g., whether an inflammatory profile supports consideration of anti-inflammatory strategies or referral to a precision pathway)[148,149].
Toward closed-loop, dynamic precision care
-
Depression is dynamic: symptoms fluctuate, biological states shift, and treatment responses change over time[49]. Therefore, precision treatment can not rely on a single baseline subtype assignment. Closed-loop care integrates continuous monitoring, real-time analysis, and adaptive intervention strategies[49,150].
Digital phenotyping gives us the tools to do this. Smartphones can passively track things like voice tone, typing speed, and how often someone interacts with others, while wearables capture heart rate variability, sleep structure, and activity levels[151,152]. These metrics become behavioral biomarkers that objectively reflect emotional changes. For example, one study in treatment-resistant depression found that drops in voice fundamental frequency showed up as much as five days before HAMD scores worsened, essentially an early warning system for relapse[49,153]. AI agents can act on these signals automatically as nudging someone toward mindfulness exercises, tweaking light therapy intensity, or alerting the clinical team to step up follow-up[153].
Importantly, the accuracy of assessment should not rely solely on biological or digital signals. Patient-reported outcomes (PROs) and quality of life (QoL) indicators can directly reflect symptoms, functions, health status, and treatment burden, which are often overlooked by doctors' ratings or sensor data[154]. PROs are widely regarded as the gold standard for assessing subjective symptoms and health-related quality of life, complementing traditional clinical endpoints such as survival rate or biomarker changes[155,156]. Embedding short, validated PRO/QoL tools (such as PHQ-9 for depressive symptoms, as well as functional and quality of life scales) into electronic or closed-loop monitoring systems has been proven feasible and readily accepted, which helps improve symptom monitoring, doctor-patient communication, and timely treatment adjustments[157]. Integrating this data into electronic health records through digital health technologies and feeding them back to patients and doctors can support collaborative decision-making and patient value-oriented healthcare, ensuring that technological progress truly enhances the quality of patients' daily lives, rather than merely optimizing a single biological or digital metric[154,158].
The next logical step involves closed-loop systems that may combine physiological markers, behavioral patterns, and treatment response data to refine mechanistic profiling over time. For instance, co-occurring signals such as more frequent nighttime awakenings, elevated cortisol levels and decreased social media engagement may support an HPA-axis hyperactivity profile with social withdrawal tendencies. It can then recommend a targeted approach combining cognitive behavioral therapy with a melatonin receptor agonist[159,160]. What's particularly interesting is that if physical activity levels do not show an improvement after a couple of weeks of this treatment, the system can flag this and suggest moving to TMS while arranging follow-up neuroimaging to better understand what is happening[55]. Such adaptive pathways represent a shift away from fixed, one-size-fits-all treatment protocols toward interactive, data-informed care[150,159].
Seamless integration into clinical workflows
-
Even the most sophisticated technology will get shelved if it does not align with the realities of clinical practise. Frontline psychiatrists typically juggle 15 to 20 patients a day, with limited time per visit, which constrains tolerance for complex interfaces or lengthy reports[161]. Therefore, precision tools should minimize clinician burden while providing clear value[93]. Smart defaults turn out to be crucial. The Mayo Clinic, for example, built pharmacogenomic test results straight into the EHR prescribing interface. When a clinician pulls up venlafaxine, the system automatically shows the patient's CYP2D6 metabolizer status as ultrarapid, normal, or poor, and flags the recommended dosing range[94,95]. That simple design drove a notable uptick in genotype-guided prescribing[49,96]. At the VA Health System, predictive models use baseline PHQ-9 scores, EHR data, and patient self-reports to estimate the probability of response to antidepressant medication, psychotherapy, or both, with the aim of eventually supporting shared decision-making in everyday practice[162,163].
In addition, natural language processing (NLP) may further reduce the burden by extracting information from unstructured clinical notes, cutting down on manual data entry. A system might automatically spot phrases like diurnal mood variation (worse in the morning), appetite loss, or suicidal ideation, then map them onto DSM-5 criteria or research biotypes[92]. For scale-up, a consistent principle is to automate data processing in the background while keeping point-of-care outputs simple, transparent, and actionable[92].
Centering health equity in precision implementation
-
The most concerning risk is that precision psychiatry could widen existing health disparities instead of narrowing them. Current multi-omics databases are heavily skewed toward specific demographic groups, with underrepresentation of racial and ethnic minorities, low-income communities, rural populations, and older adults[54,99]. Predictably, algorithms trained on these lopsided datasets often perform worse and can even introduce harmful biases in marginalized groups.
Avoiding this requires deliberate inclusive design from the start. That means enrolling diverse cohorts across race, ethnicity, and socioeconomic status when building models to enhance data representativeness. It also requires affordable alternatives (e.g., dried blood spot CRP tests, salivary cortisol) to prevent biomarker access from becoming a financial barrier. Digital inclusion matters too: phone follow-ups, text-based interventions, and support from community health workers can all reach people with limited smartphone access or digital literacy. Digital platforms need to be culturally tailored, such as language, visual design and context, so they make sense to the communities using them[99,101,102].
As emphasized by the WHO in 2023, precision medicine should support improved care at the population level rather than concentrating benefits among a small subset of patients. If precision psychiatry does not put health equity at the center of its implementation strategy, it will not live up to its promise of meaningfully reducing the global burden of mental illness[99,142].
-
Precision diagnosis and treatment of depression have made real headway, but turning mechanistic insights into standard clinical practice demands a coordinated push across technology, collaboration, and implementation[50]. Over the next decade, research should be aiming for the breakthrough integration of emerging tools, building institutionalized ecosystems for cross-disciplinary work, and creating concrete roadmaps for clinical translation (Fig. 4). These efforts are all directed toward accelerating the generation and equitable rollout of high-impact innovations[164,165].
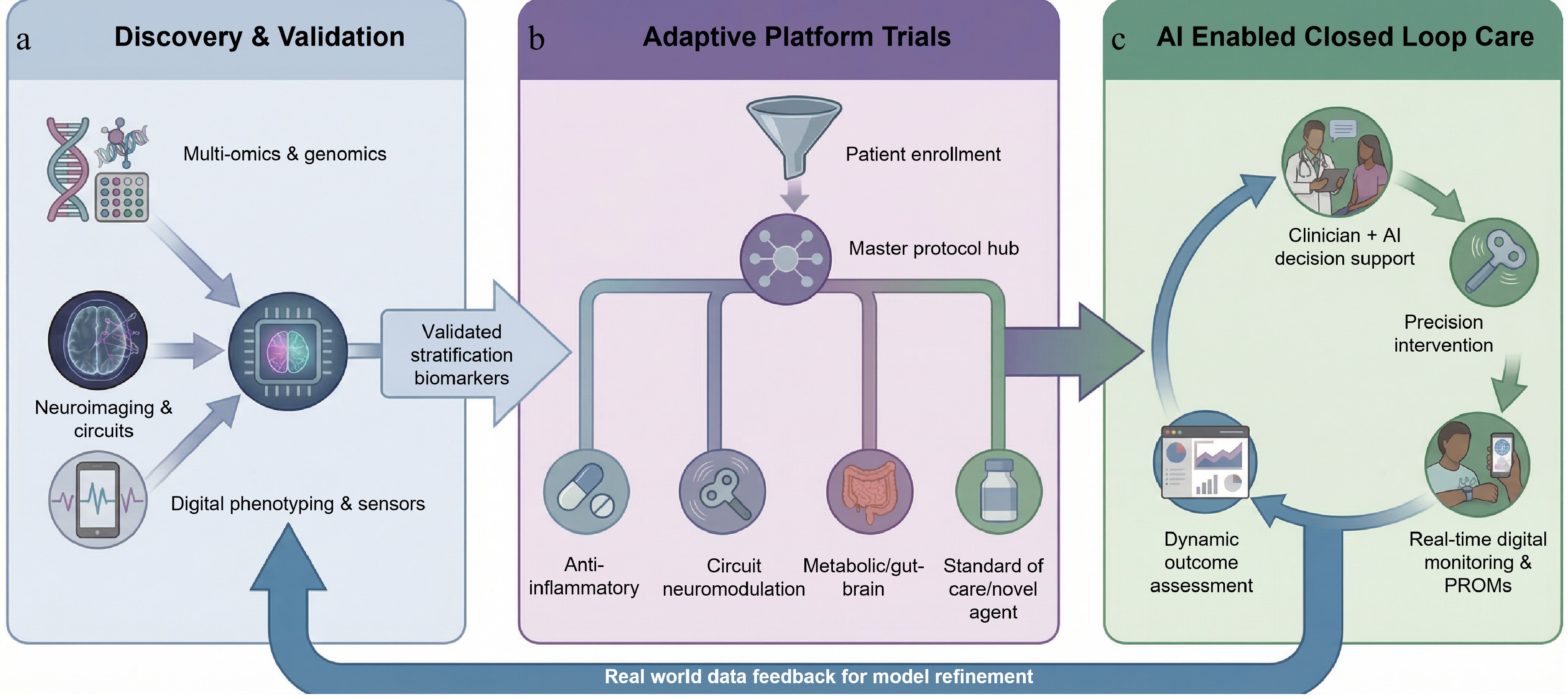
Figure 4.
An integrated roadmap for a precision psychiatry ecosystem. This framework illustrates the translational pathway from; (a) discovery and validation, where multi-omics and digital data inform AI-driven biotype identification; to (b) adaptive platform trials, utilizing master protocols to dynamically assign patients to mechanism-based treatments; and finally to (c) AI enabled closed loop care, where real-world clinical outcomes continuously refine predictive models, creating a learning health system that bridges research and clinical practice.
Emerging technological frontiers
-
Next-generation technology platforms will further sharpen our ability to untangle depression's complexity[166]. Single cell multi-omics can map transcriptomic, epigenomic, and proteomic variation within specific brain regions such as the prefrontal cortex and amygdala, across neurons, glia, and immune cells, revealing disease linked cellular subtypes and their regulatory circuits[18,49]. Paired with human induced pluripotent stem cells (iPSCs), researchers can grow patient-specific brain organoids or organ-on-chip models that mimic functional disruptions at key interfaces like the gut-brain axis or blood-brain barrier, streamlining drug screening and toxicity testing[167].
In drug development, generative AI is reshaping molecular design. By learning structure activity patterns from existing antidepressants, these systems can propose entirely new molecular scaffolds with better pharmacokinetics and target selectivity, and predict how they will perform in particular biological subtypes[168]. Meanwhile, in silico clinical trials use digital twin technology to simulate treatment responses in thousands of virtual patients, cutting development timelines and reducing late-stage failure risk[50,169].
For interventions, precision neuromodulation is moving toward closed-loop systems. Next-generation brain-computer interface (BCI) platforms decode mood-related neural activity in real time, such as theta oscillations in the anterior cingulate, and automatically fire TMS or deep brain stimulation (DBS) pulses when pathological states are detected, delivering intervention exactly when needed[166]. This kind of technology looks especially promising as a mechanism-matched, non-drug option for treatment-resistant symptoms like anhedonia or cognitive rigidity[166].
Interdisciplinary collaboration frameworks
-
A technological breakthrough alone is insufficient without the right collaborative infrastructure. A major priority is building deeply phenotyped, comprehensive depression biobanks that pull together genomic data, multi-omics profiles, neuroimaging, digital behavioral metrics, environmental exposures, and longitudinal follow-up, all while making sure the populations represented are diverse enough to prevent algorithmic bias[54,170]. These resources need to be shared openly through data ecosystems that follow FAIR principles (findable, accessible, interoperable, reusable) to enable independent validation and global collaboration[171].
Furthermore, sustained partnerships across industry, academia, and clinical care are also essential. Pharmaceutical companies bring compound libraries and trial networks, academic institutions contribute mechanistic understanding and methodological innovation, clinical centers make sure patients are engaged and findings hold up in the real world[172]. Initiatives like PsychENCODE and the EU-AIMS consortium show this kind of partnership can really speed up the journey from biomarker discovery to validation[1]. Looking ahead, patient advocacy groups and policymakers should also be incorporated to ensure that research priorities reflect patient needs and implementation constraints[173].
Clinical translation roadmap
-
To prevent innovations from remaining confined to academic journals, a translational roadmap is needed. While any timeline is inherently speculative, the following scenario-based projections outline what could be achievable under favorable conditions of continued research investment, regulatory innovation, and healthcare system adaptation. Short-term horizon (1–3 years), assuming successful completion of ongoing validation studies, could see the prospective validation of three to five mechanism-based depression subtypes, with selected biomarkers incorporated into clinical guidelines. Concurrently, if regulatory science keeps pace, we might witness the first FDA-authorization of an AI-powered clinical decision support tool classified as a medical device (SaMD) for depression treatment selection.
Medium-term targets (3–7 years) are predicated on broader health system adoption and infrastructure development. Should multimodal stratification platforms demonstrate cost-effectiveness in diverse healthcare settings, they could begin roll out across major health systems. Adaptive platform trials, assuming regulatory and payer alignment, might become a standard route for new drug approvals in depression. Digital phenotyping metrics could gain formal acceptance as regulatory endpoints if ongoing validation studies confirm their reliability and clinical utility.
The long-term vision (7–10 years) rests on the cumulative realization of these earlier milestones. If the preceding conditions are met, we could envision a future where every newly diagnosed MDD patient walks out of their initial assessment with an individualized biopsychosocial profile that guides first-line treatment selection.
None of this happens without fundamental policy shifts and strategic funding. Regulatory agencies would need to establish approval pathways designed for complex interventions, such as AI paired with medications and behavioral therapies. Insurers have to move toward value-based reimbursement that rewards precision matching, not just volume. Governments and foundations should funnel resources into high-risk, high-reward interdisciplinary work, especially implementation research focused on closing equity gaps. The timeline presented here is therefore contingent on these parallel developments occurring in synchrony.
-
The clinical management of MDD stands at a historic inflection point. For decades, symptom-based diagnosis and monoamine-focused treatments have provided a framework to work with, but they have been hobbled by a blind spot, the biological heterogeneity underlying depression. The result has been stubbornly high prevalence, disappointing remission rates, and frequent relapses[174]. This review systematically lays out why and how we need to shift toward precision psychiatry. The core pieces include weaving together multi-omics, neuroimaging, immunometabolic data, digital phenotyping, and environmental exposures to carve out biologically coherent subtypes with shared disease mechanisms; designing therapeutics matched to those mechanisms, built on genetically validated targets; speeding up translation through biomarker-enriched and adaptive trial designs, and deploying closed-loop care systems embedded in clinical workflows that allow for dynamic, individualized treatment adjustments[122].
However, technological sophistication does not automatically translate into clinical benefit. Without an explicit focus on health equity, precision approaches could exacerbate disparities. Moving forward, inclusivity, accessibility, and cultural fit need to be baked in from the start, algorithms have to perform reliably across diverse populations, biomarker testing needs to be affordable and widely available, and digital tools have to actually reach the marginalized groups.
Ultimately, precision psychiatry should aim to improve the speed, safety, and effectiveness of depression care for all patients. This is both a scientific shift and an ethical obligation. Only by braiding together mechanistic depth, intelligent data analysis, and genuine human compassion can we find our way out of the fog surrounding MDD diagnosis and treatment for so long, and step into an era that is truly patient centered, evidence based, and grounded in equity.
We gratefully acknowledge grant support from the Double First-Rate construction plan of China Pharmaceutical University (CPU2025CXY03), and Natural Science Foundation of Jiangsu Province (BK20242072).
-
Not applicable.
-
The authors confirm their contributions to the work as follows: draft manuscript preparation: Wang M, Jiang Y, Wu C; performing the graphmapping: Liao J; data collection and manuscript revision: Zhou B, Yuan Y, Sun J. All authors reviewed the results and approved the final version of the manuscript.
-
Data sharing is not applicable to this review as no datasets were generated or analyzed.
-
The authors declare no competing financial interest.
-
#Authors contributed equally: Menghua Wang, Yanli Jiang, Chunyu Wu
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press on behalf of China Pharmaceutical University. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Wang M, Jiang Y, Wu C, Liao J, Zhou B, et al. 2026. Precision psychiatry in depression via mechanism based stratification and therapy. Targetome 2(3): e019 doi: 10.48130/targetome-0026-0014 

Precision psychiatry in depression via mechanism based stratification and therapy
- Received: 29 January 2026
- Revised: 20 February 2026
- Accepted: 04 March 2026
- Published online: 11 May 2026
Abstract: Major depressive disorder (MDD) exhibits such pronounced heterogeneity that conventional symptom-based diagnoses and monoamine-focused treatments have proven largely inadequate, pushing the field toward what we now call precision psychiatry. In this review, we map out stratification approaches rooted in mechanisms spanning neural circuits, immune function, metabolic regulation, and the gut-brain axis. We also discuss how multi-omics, neuroimaging, and digital phenotyping can be integrated to construct continuous, biological grounded disease subtypes. Building from this groundwork, precision drug development has increasingly turned its attention to targets with genetic validation, therapeutics tailored to specific biological profiles, and adaptive trial designs that leverage biomarker-guided patient selection. Making this vision operational demands more than scientific insight as it requires weaving predictive algorithms into closed-loop care systems and everyday clinical practice, all while keeping health equity front and center so that technological progress does not end up widening gaps in access and outcomes. Real progress in MDD care will only emerge when we manage to blend deep mechanistic understanding with intelligent data analysis and genuinely inclusive implementation.