-
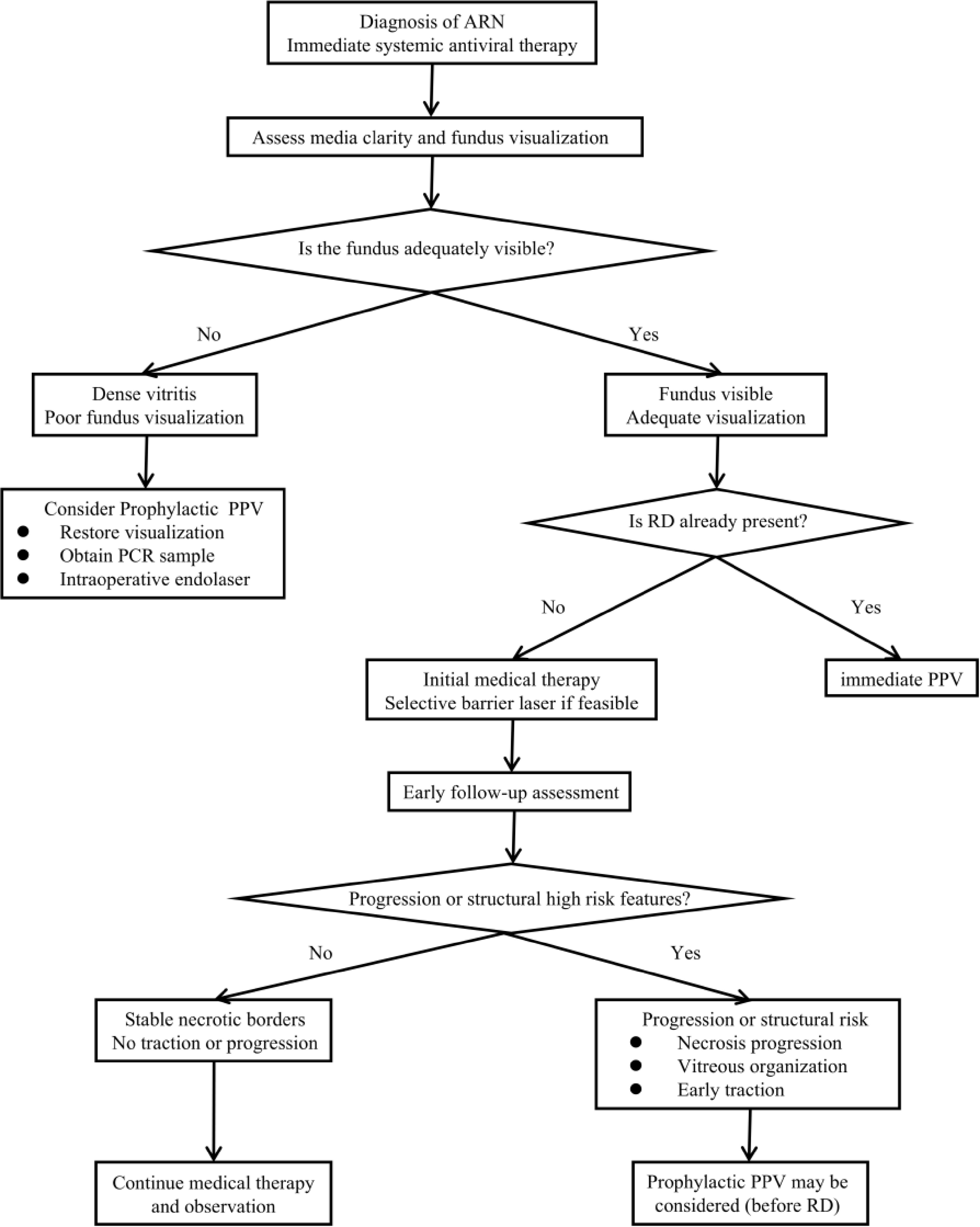
Figure 1.
Timing of prophylactic pars plana vitrectomy (PPV) in acute retinal necrosis (ARN). PCR, polymerase chain reaction; RD, retinal detachment.
-
Domain Evidence-based concern Clinical significance Implication for PPV timing Viral etiology VZV-related ARN is often associated with more extensive necrosis and a higher risk of structural complications than some other viral subtypes More aggressive viral phenotypes may require closer monitoring and earlier consideration of surgery The threshold for PPV may be lower when other high-risk features are also present Media clarity and fundus visibility Dense vitritis may obscure the peripheral retina and limit the assessment of necrotic borders, peripheral breaks, and traction It determines whether the eye can be adequately assessed and whether nonsurgical management remains feasible Poor visualization may support earlier PPV to improve retinal assessment and facilitate intraoperative treatment Retinal extent and location Posterior pole involvement or more extensive necrosis is associated with poorer visual prognosis and higher structural risk Retinal extent appears to carry substantial weight in risk assessments, especially when posterior involvement or broader disease suggests evolving structural instability Strongly favors proactive surgical intervention. Extensive lesions frequently necessitate prophylactic silicone oil tamponade during PPV Vitreoretinal traction and interface change Progressive vitreous organization and traction at the necrotic border may increase the risk of retinal breaks and later detachment Emerging tractional change is a direct sign of increasing structural instability The emergence of tractional change may support the consideration of PPV even before established RD Progressive necrosis despite therapy Continued extension of the necrotic retina despite antiviral treatment suggests ongoing disease activity and persistent structural risk This feature indicates that medical treatment alone may be insufficient to maintain stability Prophylactic PPV may be considered during early follow-up, before RD develops, if progression continues despite treatment Stable disease with adequate visualization Limited peripheral disease that remains stable under treatment may carry lower short-term structural risks Adequate visualization and stability support continued monitoring rather than immediate intervention Observation with continued chemical therapy is often appropriate, with PPV deferred unless progression or traction develops PPV, pars plana vitrectomy; VZV, varicella-zoster virus; ARN, acute retinal necrosis; RD, retinal detachment. Table 1.
Clinical features and scenarios influencing the timing of prophylactic pars plana vitrectomy in acute retinal necrosis.
Figures
(1)
Tables
(1)