









-
Acute retinal necrosis (ARN) is a necrotizing retinitis that poses a significant threat to vision and is classified as a rare but severe blinding eye disease. Vision-threatening complications associated with ARN include retinal detachment (RD), retinal ischemia, edema, and optic neuropathy[1]. ARN can be caused by several viruses, including varicella zoster virus (VZV), herpes simplex virus Type I (HSV-I), herpes simplex virus Type II (HSV-II), cytomegalovirus (CMV), and Epstein–Barr virus (EBV)[2]. Clinically, ARN is typically characterized by rapidly progressive peripheral necrotizing retinitis with prominent intraocular inflammation[3]. The diagnosis of ARN can be facilitated by polymerase chain reaction (PCR) analysis of aqueous or vitreous humor samples, allowing for timely intervention[4]. Treatment options include oral and systemic intravenous antiviral medications, intravitreal injections of antiviral drugs, local and oral corticosteroids, prophylactic retinal laser photocoagulation (LPC), and pars plana vitrectomy (PPV). Despite these combined approaches, RD continues to occur in a substantial proportion of cases and remains a major determinant of poor visual prognosis[5,6].
In this setting, prophylactic PPV has been increasingly adopted in selected patients to improve visualization, thereby allowing adequate retinal assessment and intraoperative endolaser therapy, while also reducing the risk of subsequent RD[7,8]. Nevertheless, the reported benefit of prophylactic PPV remains uncertain. Published studies vary widely in terms of patient selection, definitions of early intervention, and operative techniques, and the interpretation of outcomes is complicated by the tendency for more severe presentations to undergo surgery[9,10]. This review summarizes the current evidence on prophylactic PPV in ARN, with particular attention to the indications, timing, and operative considerations and the clinical factors that influence surgical decision-making. It suggests that surgical timing is better understood in relation to fundus assessability and structural risk than to a fixed time point after diagnosis alone.
-
ARN most often reflects the reactivation of latent herpesviruses, whereas primary infection with hematogenous dissemination appears to be rare[11]. Retinal destruction is generally caused by two converging processes. First, viral replication within retinal cells can directly cause cytolysis. Second, a severe inflammatory response with occlusive retinal vasculitis compromises retinal and choroidal perfusion, producing ischemic necrosis that amplifies tissue loss[11,12]. Optic nerve involvement may occur in parallel, and optic disc edema has been described as part of the clinical spectrum and may signal an unfavorable visual prognosis[11,13]. In the posterior segment, dense vitritis may rapidly obscure visualization of the fundus, and the vitreous cavity becomes laden with inflammatory cells and retinal debris. Even after active inflammation subsides, early vitreous organization and membrane formation can resemble proliferative vitreoretinopathy (PVR). The necrotic retina is left thin and friable, especially at the border between necrotic and viable tissue, where traction is readily translated into occult breaks and rhegmatogenous retinal detachment (RRD)[6,14,15].
Because antiviral therapy suppresses viral replication but does not reverse established vitreous organization or vitreoretinal traction, these structural changes form the pathological basis for considering surgical intervention in selected high-risk eyes[15,16].
-
ARN patients often complain of acute vision loss in the affected eye, accompanied by floaters, photophobia, and eye pain[6]. However, in a series of clinical studies, the objective ocular examination findings are of greater prognostic value for the evaluation of risk and prognosis, because dense vitritis and a wider range of retinitis are associated with a higher risk of RD[17]. In addition, intraocular pathogens are often established through viral PCR detection in the aqueous fluid and vitreous fluid and are often included in early clinical evaluation[18]. Therefore, risk stratification in many published clinical studies is usually based on viral etiology, media clarity, and the objective structural characteristics of the retina observed during examination.
Viral etiology
-
ARN is mainly caused by herpesviruses. Systematic reviews and clinical studies show that VZV is the most common pathogen, and VZV-related ARN often manifests as a more extensive peripheral retinal necrosis and may be accompanied by a higher incidence risk of RRD[6,19]. The clinical cohort study of von Hofsten et al. also found that VZV-related cases usually showed more serious inflammatory lesions and poorer baseline vision[20]. However, there are differences in the intensity of this pathogenesis with the severity of the disease and prognosis in different studies, and not all reports show statistically significant differences between viral subtypes[21]. Therefore, differences in pathogenicity among viral subtypes suggest that clinicians should consider the pathogen-specific characteristics when determining the timing of surgical intervention.
Media clarity and fundus visibility
-
A series of clinical studies on ARN show that dense vitritis is common in ARN patients, which is also a characteristic feature of the inflammatory response in this disease[6]. In the cohort reported by Fu et al., the severity of vitritis was documented as part of the clinical assessment in patients with ARN[8]. Dense vitreous inflammation may significantly impair visualization of the peripheral retina, particularly during the acute phase. Limited fundus visualization may hinder the accurate delineation of necrotic borders and evaluations of peripheral vitreoretinal changes[6,22]. Moreover, the study of Mojarrad et al. also pointed out that dense vitritis or media opacity may limit the application of prophylactic LPC[21].
Therefore, media clarity is an indicator of disease severity and it also affects the ability to adequately assess the fundus and determines whether nonsurgical treatment remains an option.
Retinal extent and structural risk
-
Some existing studies have evaluated the progression and prognostic risk of ARN by focusing on the extent and location of retinal necrosis. Multicenter studies, including those by Soitong et al., have further demonstrated that the extent of retinal involvement is closely associated with visual outcomes in ARN. In particular, the lesions that involve the posterior pole (Zone 1) usually suggest that the disease is more serious and is associated with poor visual prognosis and higher risk of RD[23]. In a nonsurgical treatment cohort study confirmed by PCR, posterior polar involvement was identified as an independent risk factor for poor prognosis, and RD was closely related to the failure of vision improvement[24]. On the contrary, the involvement of the mid-peripheral region (Zone 2) is more often discussed in practice as an indication for prophylactic PPV, whereas lesions in the the most peripheral zone (Zone 3) are more often treated conservatively when the condition is stable[7]. Notably, when intraoperative visualization is adequate, structural retinal changes can often be observed near the necrotic margins, suggesting that traction at these borders may also contribute to disease progression[25].
In summary, these findings suggest that retinal extent and the associated structural changes are particularly relevant when the timing of prophylactic PPV is considered in a risk-based manner. The factors discussed above and their relevance to prophylactic PPV timing are summarized in Table 1.
Table 1. Clinical features and scenarios influencing the timing of prophylactic pars plana vitrectomy in acute retinal necrosis.
Domain Evidence-based concern Clinical significance Implication for PPV timing Viral etiology VZV-related ARN is often associated with more extensive necrosis and a higher risk of structural complications than some other viral subtypes More aggressive viral phenotypes may require closer monitoring and earlier consideration of surgery The threshold for PPV may be lower when other high-risk features are also present Media clarity and fundus visibility Dense vitritis may obscure the peripheral retina and limit the assessment of necrotic borders, peripheral breaks, and traction It determines whether the eye can be adequately assessed and whether nonsurgical management remains feasible Poor visualization may support earlier PPV to improve retinal assessment and facilitate intraoperative treatment Retinal extent and location Posterior pole involvement or more extensive necrosis is associated with poorer visual prognosis and higher structural risk Retinal extent appears to carry substantial weight in risk assessments, especially when posterior involvement or broader disease suggests evolving structural instability Strongly favors proactive surgical intervention. Extensive lesions frequently necessitate prophylactic silicone oil tamponade during PPV Vitreoretinal traction and interface change Progressive vitreous organization and traction at the necrotic border may increase the risk of retinal breaks and later detachment Emerging tractional change is a direct sign of increasing structural instability The emergence of tractional change may support the consideration of PPV even before established RD Progressive necrosis despite therapy Continued extension of the necrotic retina despite antiviral treatment suggests ongoing disease activity and persistent structural risk This feature indicates that medical treatment alone may be insufficient to maintain stability Prophylactic PPV may be considered during early follow-up, before RD develops, if progression continues despite treatment Stable disease with adequate visualization Limited peripheral disease that remains stable under treatment may carry lower short-term structural risks Adequate visualization and stability support continued monitoring rather than immediate intervention Observation with continued chemical therapy is often appropriate, with PPV deferred unless progression or traction develops PPV, pars plana vitrectomy; VZV, varicella-zoster virus; ARN, acute retinal necrosis; RD, retinal detachment. -
Management of ARN generally requires a combination of pharmacological and surgical interventions. Pharmacological therapy includes antiviral agents, glucocorticoids, anti-inflammatory drugs, and antiplatelet agents, whereas the surgical options include LPC and PPV.
Systemic antiviral therapy is the cornerstone of ARN management, aimed at halting disease progression and protecting the contralateral eye[6,26]. At present, there is no direct evidence that prophylactic PPV in the affected eye changes the risk of involvement in the contralateral eye.
Intravenous acyclovir (IV ACV) remains the standard treatment[27]. In recent years, oral valacyclovir has emerged as an effective alternative[28]. In addition to systemic treatment, the role of intravitreal injections of antiviral drugs as an adjunctive therapy has also gained recognition. However, they should not be used as monotherapy because of the risk of contralateral eye involvement[2]. Meanwhile, the use of systemic corticosteroids is crucial for inhibiting the host's inflammatory response and reducing damage to the optic nerve and retinal blood vessels[29].
LPC aims to create a barrier at the junction between necrotic and healthy retina to prevent retinal tears and RD resulting from pathological changes[30].
However, its efficacy remains controversial. In the presence of dense vitritis, adequate visualization of the peripheral retina may not be achievable, limiting precise laser placement. Furthermore, although some studies suggest that LPC may reduce the incidence of RD[31], large-scale meta-analyses and retrospective studies have failed to provide conclusive evidence supporting its independent role in preventing RD[32,33]. Consequently, routine prophylactic laser is not uniformly adopted in clinical practice and is often individualized according to the extent and location of retinal involvement[1].
However, current nonsurgical management primarily suppresses viral replication and intraocular inflammation, and does not eliminate inflammatory mediators within the vitreous or relieve traction caused by necrotic retinal tissue. As a result, the incidence of RD remains as high as 50% with antiviral monotherapy[34]. Patients with severe disease often require additional therapeutic modalities to improve their visual prognosis.
-
Prophylactic PPV refers to vitrectomy performed during the acute inflammatory phase or the post-inflammatory period before the occurrence of RD. The procedure aims to remove inflammatory mediators and cytokines from the vitreous cavity and to relieve vitreoretinal traction on necrotic and thinned retina. It is often combined with intraoperative LPC to seal the necrotic margins, thereby reducing the incidence of RD[2,6]. This topic remains a central focus of ongoing discussion.
Some retrospective series and pooled analyses suggest that prophylactic PPV may reduce the subsequent risk of RD in selected settings[10,35,36], whereas other reports do not support its routine application across all cases and note that visual outcomes may remain poor despite surgery[35,37].
The differences between existing research conclusions are more likely to be caused by differences in patient selection criteria, the definition of early intervention, and surgical techniques, rather than different views on the efficacy of the surgery itself.
Evidence appraisal
-
In many cohort studies, prophylactic PPV is prioritized for patients who are considered to be at high risk, such as extensive retinal necrosis, severe vitreitis, visual axis obstruction, and unsuitability for laser treatment or early retinal traction. As a result, there is a difference in the severity of the baseline condition between the surgical group and the nonsurgical group, making it difficult to compare the two directly. When diseases of different severity are combined and analyzed, the potential benefits of specific high-risk subgroups may become less obvious, which may partly explain the inconsistent conclusions in the summary analysis[27,38]. This limits a direct comparison between surgical and nonsurgical cohorts.
The definition of prophylactic PPV also varies from study to study. Some studies define early surgery according to the time from diagnosis[36], whereas others define it according to the anatomical status at presentation, such as the presence of established RD or suspected peripheral retinal breaks[27]. A recent analysis of the IRIS registry defines early PPV as surgery performed on eyes without established RD within 31 days after diagnosis, which shows that the definition of the timing of prophylactic PPV in comparative analyses of different studies is inconsistent[38]. These different criteria make it impossible for the research population to be directly compared. Therefore, research classified as focusing on early intervention may actually correspond to different clinical situations, which makes the interpretation of the conclusions based solely on the timing of surgery more complicated.
Reported outcomes also differ across studies. Some studies focus mainly on RD, whereas others place more emphasis on final visual acuity or visual prognosis[38,39]. Other reports pay greater attention to anatomical outcomes or the later clinical course[6,38]. As a result, studies that appear to evaluate the same intervention may still be addressing different clinical endpoints. This is particularly relevant in ARN, where anatomical stabilization and visual outcomes do not always move in parallel[6,38]. Therefore, differences in the definition of outcomes further complicate the interpretation of the reported effects of prophylactic PPV.
Differences in surgical techniques further complicate comparisons of the outcomes. Differences in vitreous base management, endolaser photocoagulation, and tamponade selection are rarely analyzed independently, yet these factors may influence both RD rates and visual outcomes. Without considering these operational differences, it remains difficult to determine whether variations in the outcomes reflect surgical timing alone or the broader operative strategy chosen[2,6,33].
Taken together, these limitations help explain why the current literature remains inconclusive and why existing studies do not support a single timing threshold for prophylactic PPV. In this context, the review focuses on the clinical circumstances in which prophylactic PPV is considered, with particular emphasis on surgical timing and decision-making.
Timing in clinical practice
-
Published studies describe diversified strategies for the selecting the timing of prophylactic PPV in ARN[1,27]. In published reports, the timing of prophylactic PPV does not follow a uniform pattern and may be influenced by ocular findings at presentation and by changes that become evident during follow-up. Media clarity, the severity and extent of the disease, and differences in treatment preference across centers may all influence when prophylactic PPV is considered.
Dense vitreous inflammation in the acute phase may obscure visualization of the fundus, thereby limiting an accurate assessment of the extent of retinal involvement[22]. In this context, extremely early PPV has been proposed as a way to restore fundus visualization, better define the extent of retinal necrosis, and identify and manage peripheral vitreoretinal changes that may later lead to RD. In addition, in extremely early PPV, undiluted vitreous samples can be obtained for PCR detection, which helps to identify the causative virus[1]. At the same time, if the condition requires it, LPC can be further implemented during surgery[40]. However, because of the different definitions of indications in different studies and limited high-quality control data, the best time for surgery is still controversial.
In contrast, when media clarity is adequate at presentation, systemic antiviral therapy should be initiated promptly, followed by corticosteroids to control inflammation. PPV may be indicated if the disease progresses despite therapy, particularly in the presence of increasing vitreoretinal traction or progressive extension of retinal necrosis[17]. In this setting, surgery does not need to wait for the complete resolution of inflammation. Instead, it may be more practical to operate after treatment has brought the eye to a relatively more stable clinical state. This is usually reflected by a smaller anterior chamber reaction, reduced vitreous haze, improved fundus visualization, and clearer delineation of the necrotic borders[6,41]. These changes may help reduce intraoperative difficulty and allow more accurate intraoperative assessments. However, there is still no uniform standard in the current literature for this clinical judgment. Similarly, Fu et al. pointed out that when dense vitritis or retinitis has not improved after systemic and intravitreal antiviral therapy, and there is no RD, prophylactic PPV can be performed[8].
In summary, the existing literature shows that the timing of prophylactic PPV in ARN is best guided by the assessability of the fundus and signs of structural instability, not simply on the time from disease onset or diagnosis alone.
Based on the clinical scenarios described above, a simplified decision-making framework for prophylactic PPV in ARN is illustrated in Figure 1.
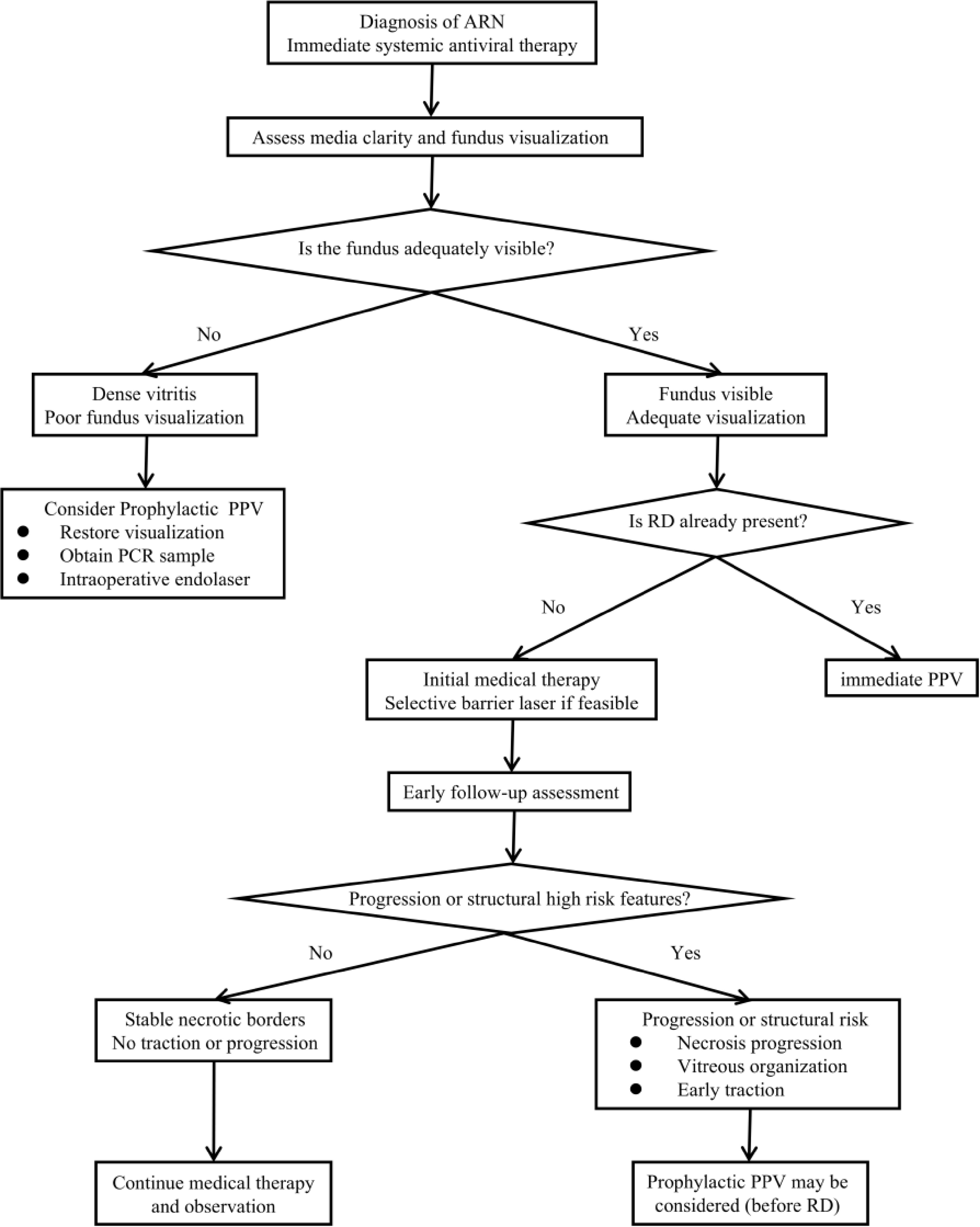
Figure 1.
Timing of prophylactic pars plana vitrectomy (PPV) in acute retinal necrosis (ARN). PCR, polymerase chain reaction; RD, retinal detachment.
Operative considerations in practice
Traction control
-
The traction at the vitreoretinal interface has been repeatedly mentioned in surgery-related literature and is regarded as an important part of retinal fissure and secondary detachment in ARN, especially when vitreous organization and inflammatory adhesions are gradually aggravated[6]. In a series of studies on ARN-related RD cases, it was emphasized that particular care should be taken when separating the vitreous from the retina and removing the peripheral vitreous, as the necrotic retina is prone to iatrogenic retinal breaks[42]. The study of Nie et al. pointed out that RD still occurs after PPV in some patients, which is often associated with PVR, indicating that the prognosis cannot be determined by the timing of surgery alone[7]. Therefore, gentle removal of the vitreous base should be attempted during surgery to reduce traction at the margins of the necrotic retina, and additional macular procedures should be performed only when clear signs of macular involvement are present, rather than as a routine practice[10].
Endolaser strategy
-
Intraoperative LPC is often used as an adjunct during PPV, typically applied around the margins of the necrotic retina when visualization permits[6]. Wu et al. supported the use of extensive peripheral LPC during ARN surgery, including 360° circumferential laser treatment[42]. However, other studies favor a selective barrier laser approach, performing localized LPC posterior to the necrotic margins without extensive peripheral photocoagulation[6]. Because of the lack of direct comparisons of different laser strategies, it is difficult to determine the best unified model at present.
Tamponade selection
-
There are differences in the selection of fillers in the prophylactic PPV strategies used for ARN[6]. In the surgical series of ARN-related RD, silicone oil is often used in cases of extensive retinal necrosis or PVR to prevent recurrence[42]. However, the preventive research cohort shows that postoperative detachment of silicone oil filling the eye may still occur, indicating that the filling cannot completely eliminate the structural risk[7]. A study of the outcomes of silicone oil removal further emphasizes the surgical consequences of this choice[43]. In general, existing evidence supports an individualized approach to tamponade selection based on intraoperative findings rather than routine use.
-
In this review, we focus on the actual surgical timing and operational considerations reported in real-world clinical practice. The necessity and timing of surgery usually need to be judged according to the clinical evaluation of high-risk characteristics, including the specific etiology of the virus, the degree of vitreous opacity, and the structural risk factors related to the extent and severity of retinal necrosis. Existing studies suggest that PPV is often considered and implemented before RD occurs. This intervention is more common in two types of situations: Obvious limitation of the field of view caused by severe vitritis in the early stage of the disease, or progressive necrosis or traction-related changes occur despite antiviral treatment during early follow-up. In addition, anatomical outcomes may also be influenced by intraoperative strategies, particularly the management of traction in fragile retinal areas, the extent of endolaser photocoagulation, and the choice of intraocular tamponade. However, the current evidence remains insufficient to define their independent effect[6,27].
At present, there is no uniform definition of prophylactic PPV in ARN. Future studies should prioritize standardization of this definition and adopt more comparable study designs to better clarify the timing and potential benefits of surgery. More unified standards are also needed for case severity stratification, surgical techniques, and the reporting of clinical outcomes. Such improvements will be important for defining the role and timing of prophylactic PPV in ARN more clearly.
This research was supported by the Department of Ophthalmology at the First Hospital of Jilin University, which provided the necessary facilities and excellent academic environment for this study. We extend our sincere gratitude to our colleagues for their stimulating discussions and assistance. Finally, we acknowledge the anonymous reviewers for their insightful comments and suggestions. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
-
Not applicable.
-
The authors confirm their contributions to the paper as follows: writing – original draft preparation: Liu R; writing – review and editing: Hui P, Teng S; conception: Sun Y. All authors reviewed the results and approved the final version of the manuscript.
-
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
-
The authors declare that they have no conflict of interest.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Liu R, Hui P, Teng S, Sun Y. 2026. Optimal timing and efficacy of prophylactic pars plana vitrectomy in acute retinal necrosis: insights from literature and clinical practice. Visual Neuroscience 43: e022 doi: 10.48130/vns-0026-0020 

Optimal timing and efficacy of prophylactic pars plana vitrectomy in acute retinal necrosis: insights from literature and clinical practice
- Received: 11 January 2026
- Revised: 23 April 2026
- Accepted: 29 April 2026
- Published online: 20 May 2026
Abstract: Acute retinal necrosis (ARN) is a rare but vision-threatening disease. Retinal detachment (RD) is a common complication that leads to severe vision loss. Molecular analysis of the aqueous or vitreous humor using polymerase chain reaction (PCR) enables precise diagnosis and facilitates timely therapeutic intervention. Although antiviral therapy is the cornerstone of managing ARN, pharmacological treatment alone often fails to prevent RD. Therefore, pars plana vitrectomy (PPV) is often considered before RD develops in clinical practice. However, its role in this setting and the optimal timing of surgery have yet to be clearly defined and remain debated. In this review, we propose that the timing of prophylactic PPV is better considered in relation to fundus visibility and the presence or evolution of structural risk, rather than as a fixed time point after diagnosis.