










-
Neuroendocrine neoplasms (NENs) are subtype neoplasms of the endocrine system. They were formerly known as 'carcinoids' due to their simple structure and weak invasiveness relative to cancer. Despite the low incidence rate of NENs, with the development of detection techniques, an increasing number of NENs patients have been identified in recent years[1]. NENs derive from the body's neuroendocrine cells in their original form, although some recent studies reveal that NENs may originate from stem cells[2−4]. However, NENs are most commonly found in the gastrointestinal tract and pancreas; hence, they are named gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs). A recent epidemiological investigation on GEP-NENs revealed that the occurrence of GEP-NENs has been progressively increasing over the last 40 years[5]. GEP-NENs are categorized as either functional or non-functional according to whether or not they are capable of secreting hormones or active substances, such as serotonin.
In spite of the slow growth of GEP-NENs, a large proportion of small bowel and pancreatic NENs were metastatic at diagnosis[6]. It is reported that approximately half of GEP-NENs patients had synchronous or metachronous metastases[7]. Moreover, the liver is the most common metastatic site of GEP-NENs. Metastatic GEP-NENs can seriously impair the quality of life; patients suffer from minor and major complications, such as bowel obstruction, hepatic failure, reduction of pulmonary function, and pathological fracture. Furthermore, GEP-NENs micrometastasis could be found in any body tissue, making it difficult to eliminate all tumor cells. Therefore, metastatic GEP-NENs, as a special group of GEP-NENs, deserve further investigation.
Comprehensive treatment strategies for metastatic GEP-NENs include resection of primary and metastatic sites, systemic chemotherapy, and local radiotherapy[8]. Several studies have reported that surgery and chemotherapy are beneficial in controlling tumor burden[9−12]. However, there is insufficient high-quality data to evaluate the prognosis of stage IV GEP-NENs. In this study, clinical data of stage IV GEP-NENs was obtained from the SEER database, and randomly allocated in the training and validation sets in a 7:3 ratio. Subsequently, the independent risk factor of overall survival in GEP-NENs patients was identified. Then, a predictive nomogram was developed to evaluate patients with stage IV GEP-NENs and make predictions about their overall survival. The validation set also verified the accuracy of the predictive model.
-
First, the approval of the Surveillance, Epidemiology, and End Results (SEER) database (account ID: 12311-Nov2021) was acquired. Then, stage IV GEP-NENs patients were selected as the study object. Clinical data of GEP-NENs patients was downloaded from a database named 'SEER Research Plus Data, 18 Registries, Nov 2019 Sub (2000–2017)' via SEER. Stat software (version 8.4.0.1). 'SEER Research Plus Data, 18 Registries, Nov 2019 Sub (2000–2017)' is a subset of the SEER database and contains the newly diagnosed tumor patients from 2000 to 2017. The clinical data of individuals with stage IV GEP-NENs were examined using a retrospective analysis. The following is a list of the requirements for inclusion: (a) patients were diagnosed with NENs based on histopathology, (b) primary NENs originated from the gastrointestinal tract or pancreas, and (c) the American Joint Committee on Cancer (AJCC) stage IV was confirmed, which was used the 7th edition of AJCC classification system[13]. Patients were identified by the International Classification of Disease for Oncology, third edition (ICD-O-3) for histology type codes (8013, 8150, 8151, 8152, 8153, 8154, 8156, 8240, 8241, 8243, 8244, 8245, 8246, and 8249) and primary site codes (C16.0 to C16.6, C16.8 to C16.9, C17.0 to C17.3, C17.8 to C17.9, C18.0 to C18.9, C19.9, C20.9, C24.1, C25.0 to C25.2, C25.4, and C25.7 to C25.9). The exclusion criteria were unknown race, tumor differentiation, tumor size, T and N stage, metastasis status and surgery of primary site, and incomplete survival data. It is worth noting that patients diagnosed from 2010–2017 were included in this study due to their detailed metastasis data since 2010. Based on the above screening criteria, all cases were randomly allocated to the training set and validation set at a proportion of 70%:30%.
Data elements
-
For this study, the clinical variables that possibly correlated with the prognosis were age, race, sex, primary site, differentiation, tumor size, tumor-node-metastasis (TNM) stage, lymph node (LN) metastasis, surgery, chemotherapy, radiotherapy, and bone, brain, liver and lung metastases. Five categorical variables were included in the study for the primary site variables: the stomach, small intestine, pancreas, colorectum and others (Ampulla Vater, Appendix). The main end outcome of this study was overall survival (OS). The definition of OS was the date from diagnosis to death (for any reason) or loss to follow-up. The OS was used to evaluate the clinical outcome of stage IV GEP-NENs patients.
Nomogram establishment and validation
-
First of all, to identify the risk factors of OS for stage IV GEP-NENs patients, univariate and multivariate Cox regression analysis was carried out in the training cohort. Then, a prognostic nomogram that integrated with the risk factors of OS was constructed. The comparison of the nomogram-predicted outcome and actually observed outcome was evaluated by C-index and calibration curve. ROC and AUC accessed the specificity and sensitivity of the predictive nomogram. Moreover, the clinical benefit of the predictive nomogram was estimated by using DCA. Scatter plot analysis was used to evaluate the relationship between risk score and survival months. Kaplan-Meier analysis was adopted to evaluate the prognosis of the two groups. Both the training and validation cohorts were used to evaluate the established nomogram. All the above analysis were achieved by using R Studio software (version 4.2.1).
Statistical analysis
-
To carry out a comparison between two subgroups that had categorical variables, either the Chi-square test or Fisher's exact test was utilized. The Kruskal-Wallis test was used for continuous variables if appropriate. Cox regression analyses, both univariate and multivariate, were applied in order to determine risk variables of overall survival and the hazard ratio (HR) of clinical features. R Studio software (version 4.2.1) was utilized to finish the statistical analysis. A p-value of less than 0.05 was regarded as statistically significant.
-
According to inclusion and exclusion criteria, 2,139 stage IV GEP-NENs patients were enrolled in this study (Fig. 1). The patients were randomly distributed across the training group (n = 1,497) and validation group (n = 642) (ratio = 7:3). Information in great detail on the two subgroups of patients is summarized in Table 1. The raw data from the screening in this study can be found in the Supplementary Data 1. In the training group, 775 (51.8%) were male patients, 897 (59.9%) patients were less than 65 years old, and most of the patients belonged to the white race (n = 1,219, 81.4%). For the validation group, 336 (52.3%) were male patients, 375 (58.4%) patients were less than 65 years old, and the vast majority of patients were of the white race (n = 537, 83.6%). Regarding other variables, the proportion of primary site, tumor differentiation, tumor size, LN metastasis, surgery, chemotherapy, radiotherapy, distant metastatic site, and vital status of the training group was similar to the validation group (Table 1). The comparison of all clinical characteristics of the patients in the two subgroups revealed no significant differences. The training group was utilized for the predictive model development and internal validation. External validation was done by the validation group.
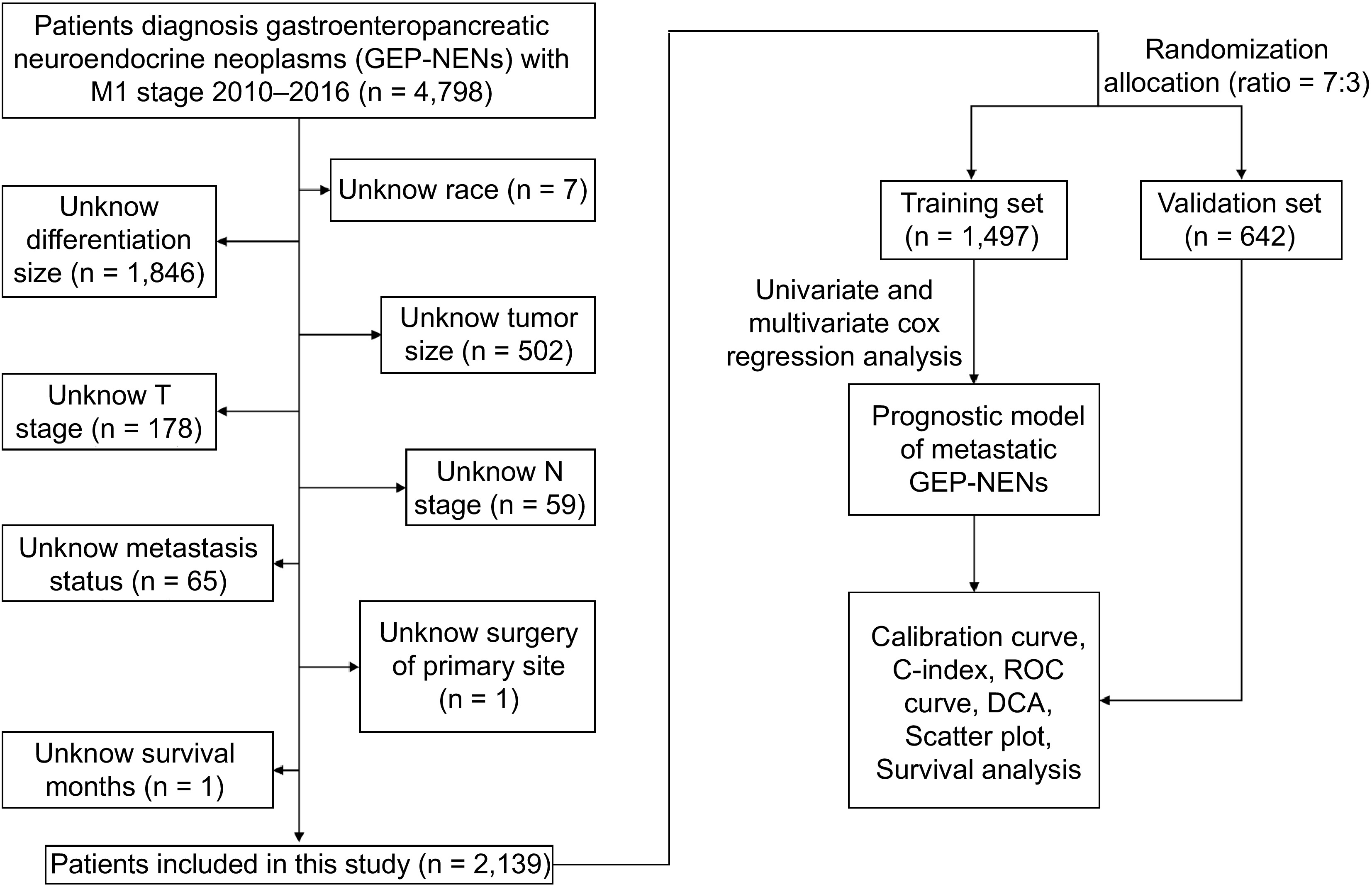
Figure 1.
Flow chart of patient selection and research routine of this study.
Table 1. Characteristics of stage IV GEP-NENs.
Characteristics Training set
(n = 1,497)Validating set
(n = 642)p-value Sex 0.847 Female 722 (48.2%) 306 (47.7%) Male 775 (51.8%) 336 (52.3%) Age (year) 0.546 < 65 897 (59.9%) 375 (58.4%) ≥ 65 600 (40.1%) 267 (41.6%) Race 0.449 Black 198 (13.2%) 73 (11.4%) White 1219 (81.4%) 537 (83.6%) Other* 80 (5.3%) 32 (5.0%) Primary site 0.824 Stomach 56 (3.7%) 21 (3.3%) Colorectum 326 (21.8%) 148 (23.1%) Pancreas 401 (26.8%) 169 (26.3%) Small intestine 652 (43.6%) 272 (42.4%) Other* 62 (4.1%) 32 (5.0%) Tumor differentiation 0.610 Well differentiated 764 (51.0%) 311 (48.4%) Moderately differentiated 305 (20.4%) 146 (22.7%) Poorly differentiated 296 (19.8%) 129 (20.1%) Undifferentiated 132 (8.8%) 56 (8.7%) Tumor size (mm) 0.934 ≤ 20 392 (26.2%) 166 (25.9%) 21 − 40 561 (37.5%) 246 (38.3%) ≥ 41 544 (36.3%) 230 (35.8%) LN metastasis 0.065 No 438 (29.3%) 162 (25.2%) Yes 1059 (70.7%) 480 (74.8%) Surgery 0.260 None surgery 357 (23.8%) 138 (21.5%) Resection 1140 (76.2%) 504 (78.5%) Chemotherapy 0.984 No/Unknown 998 (66.7%) 429 (66.8%) Yes 499 (33.3%) 213 (33.2%) Radiotherapy 0.231 No 1447 (96.7%) 613 (95.5%) Yes 50 (3.3%) 29 (4.5%) Bone metastasis 0.344 No 1423 (95.1%) 617 (96.1%) Yes 74 (4.9%) 25 (3.9%) Brain metastasis 0.805 No 1482 (99.0%) 637 (99.2%) Yes 15 (1.0%) 5 (0.8%) Liver metastasis 0.205 No 381 (25.5%) 181 (28.2%) Yes 1116 (74.5%) 461 (71.8%) Lung metastasis 0.642 No 1422 (95.0%) 606 (94.4%) Yes 75 (5.0%) 36 (5.6%) Vital status 0.906 Alive 759 (50.7%) 323 (50.3%) Dead 738 (49.3%) 319 (49.7%) Race, Other* (American Indian/AK Native, Asian/Pacific Islander); Primary site, Other* (Ampulla Vater, Appendix). Cox proportional hazards regression model analysis
-
The Cox proportional hazards regression model was utilized to identify factors that might increase the risk of overall survival. The result showed that age, sex, primary site, tumor differentiation, tumor size, surgery, chemotherapy, bone metastasis, brain metastasis, and lung metastasis were the risk factors influencing the overall survival of patients (p < 0.05) (Table 2). Additionally, a multivariate analysis was conducted to confirm the independent risk factor of overall survival. According to the result, the independent risk factors were listed as follows: age, primary site, tumor differentiation, tumor size, surgery, chemotherapy, and lung metastasis (p < 0.05) (Table 2). As shown in Fig. 2, independent risk factors that correlated with overall survival were identified in the training set.
Table 2. Univariate and multivariate analysis of overall survival in patients of the training group.
Characteristic Univariate analysis Multivariate analysis Hazard ratio (95% CI) p-value Hazard ratio (95% CI) p-value Age < 65 1 1 ≥ 65 1.768 (1.529−2.043) < 0.001*** 1.7388 (1.4983−2.0178) < 0.001*** Sex Female 1 1 Male 1.186 (1.027−1.371) 0.0206* 1.1354 (0.9770−1.319)4 0.0976 Race Black 1 White 0.9511 (0.7683−1.177) 0.645 Other 0.8780 (0.5992−1.286) 0.504 Primary site Stomach 1 1 Pancreas 0.4687 (0.3393−0.6475) < 0.001*** 0.5646 (0.4057−0.7859) < 0.001*** Small intestine 0.1693 (0.1215−0.2360) < 0.001*** 0.4707 (0.3238−0.6844) < 0.001*** Colorectum 0.8889 (0.6448−1.2254) 0.472 1.0968 (0.7842−1.5341) 0.5892 Other 0.5199 (0.3386−0.7982) 0.0028** 0.7265 (0.4611−1.1447) 0.168 Tumor differentiation Well 1 1 Moderate 1.406 (1.133−1.746) 0.0020** 1.2833 (1.0308−1.5975) 0.0256* Poor 7.245 (6.044−8.685) < 0.001*** 4.9798 (4.0054−6.1913) < 0.001*** Undifferentiated 7.344 (5.841−9.235) < 0.001*** 4.3354 (3.3169−5.6666) < 0.001*** Tumor size ≤ 20 1 1 21−40 1.688 (1.352−2.107) < 0.001*** 1.2281 (0.9751−1.5469) 0.0809 ≥ 41 3.609 (2.924−4.454) < 0.001*** 1.6713 (1.3110−2.1305) < 0.001*** LN metastasis No 1 Yes 0.952 (0.8141−1.113) 0.538 Surgery None surgery 1 1 Resection 0.3404 (0.2922−0.3967) < 0.001*** 0.5327 (0.4386−0.6471) < 0.001*** Chemotherapy No/unknown 1 1 Yes 2.146 (1.855−2.484) < 0.001*** 0.7411 (0.6177−0.8891) 0.0013** Radiotherapy No 1 Yes 1.131 (0.7751−1.65) 0.524 Bone metastasis No 1 1 Yes 2.458 (1.877−3.219) < 0.001*** 1.1790 (0.8839−1.5725) 0.2625 Brain metastasis No 1 1 Yes 5.609 (3.348−9.4) < 0.001*** 1.4468 (0.8486−2.4666) 0.1748 Liver metastasis No 1 Yes 1.082 (0.9165−1.279) 0.351 Lung metastasis No 1 1 Yes 3.094 (2.376−4.028) < 0.001*** 1.4748 (1.1180−1.9455) 0.0060** * p-value < 0.05; ** p-value < 0.01; *** p-value < 0.001; CI, confidence interval. Values in blodface were p-value < 0.05. 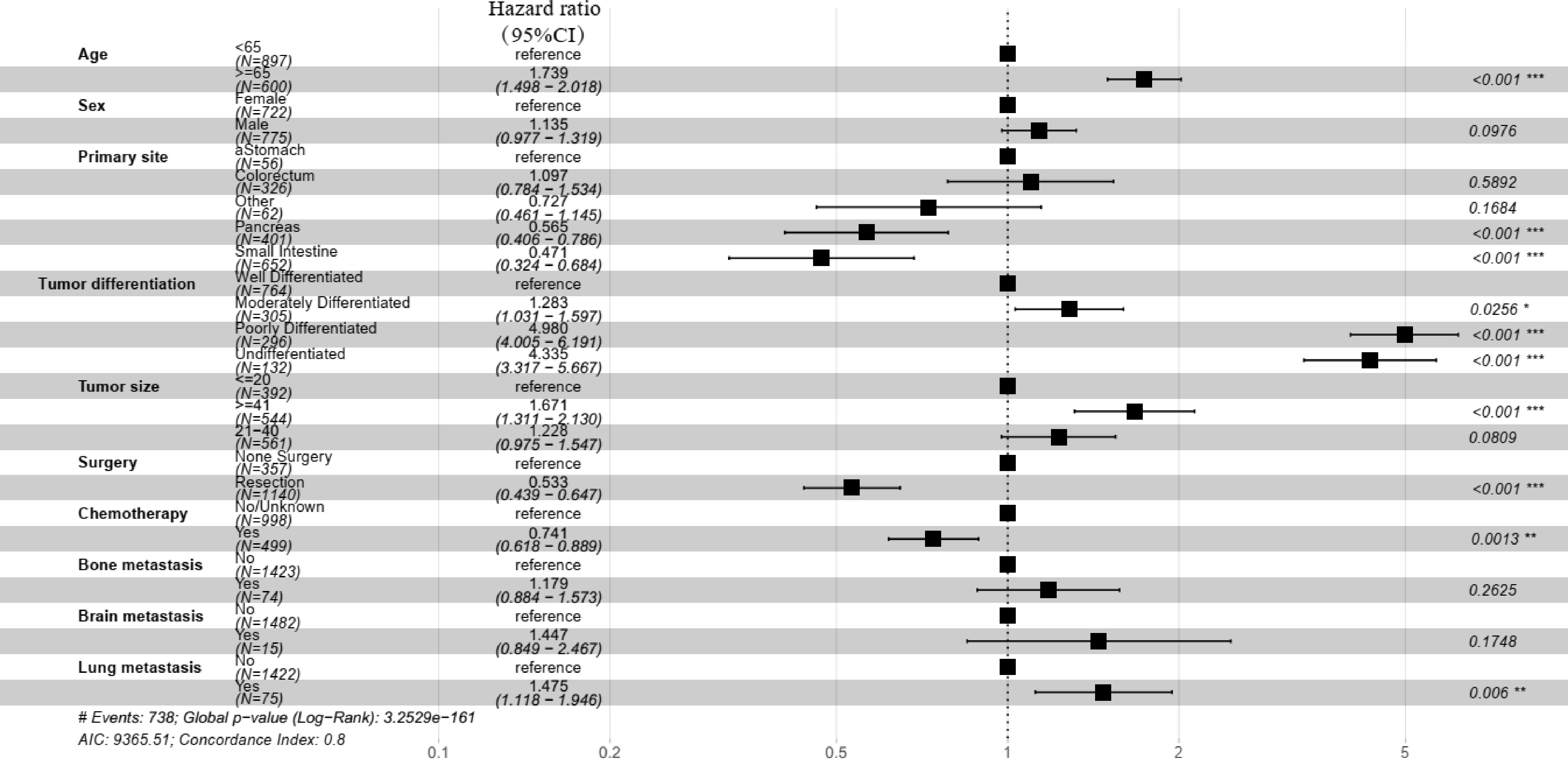
Figure 2.
Forest plot of the multivariate Cox regression analysis of the training group.
Prognostic nomogram establishment
-
Based on the results of univariate Cox analysis, a prognostic nomogram was constructed to estimate 1-, 3-, and 5-year overall survival probabilities. Potential risk variables, including age, sex, primary site, tumor differentiation, tumor size, surgery, chemotherapy, and bone, brain and lung metastases, were used to evaluate the corresponding scores. Eventually, all scores were added to the total points utilized to evaluate the overall survival probabilities (Fig. 3).
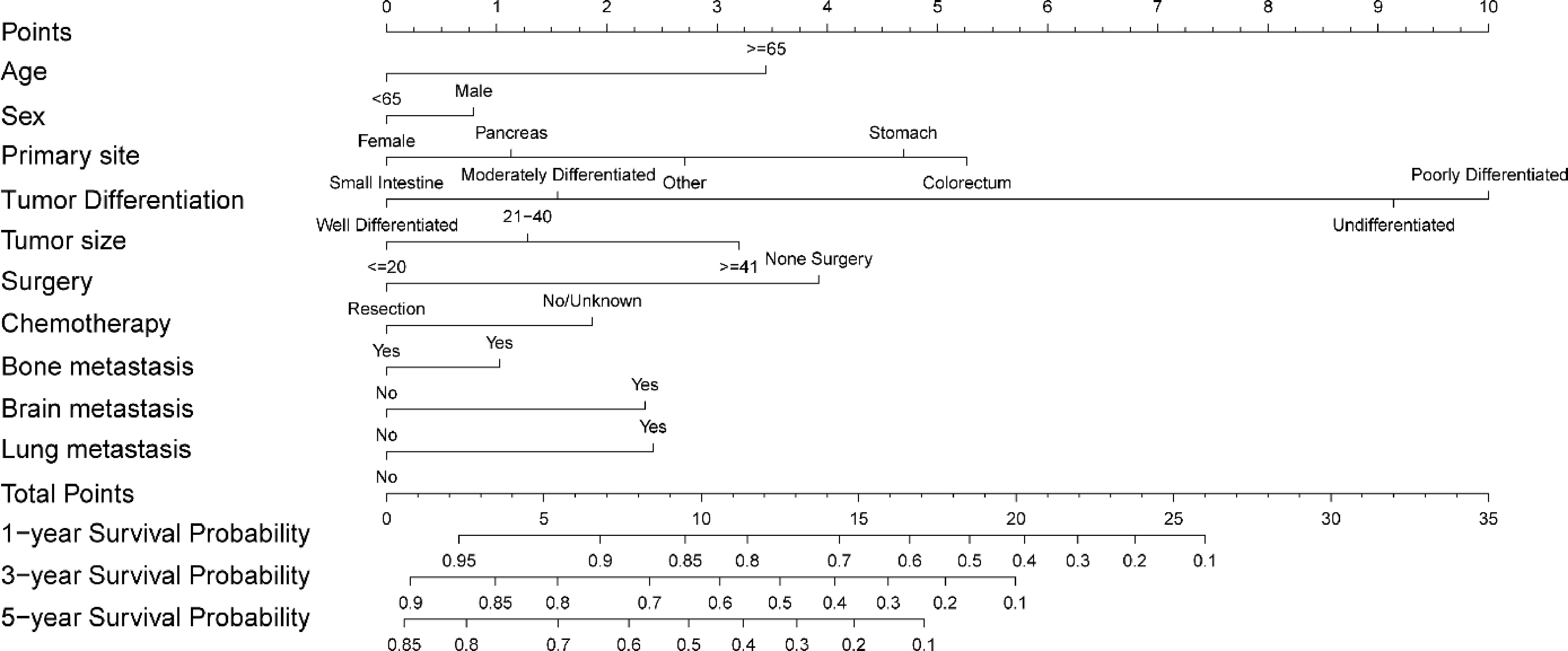
Figure 3.
The prognostic nomogram for predicting overall survival of stage IV GEP-NENs in the training group.
Calibration curve analysis of nomogram and validation
-
The calibration curve was used to evaluate the uniformity between the prognostic nomogram's predictive and actual survival probabilities. As illustrated in Fig. 4, the nomogram-predicted survival probabilities of the training group and validation group were highly congruent with actual observing outcomes.
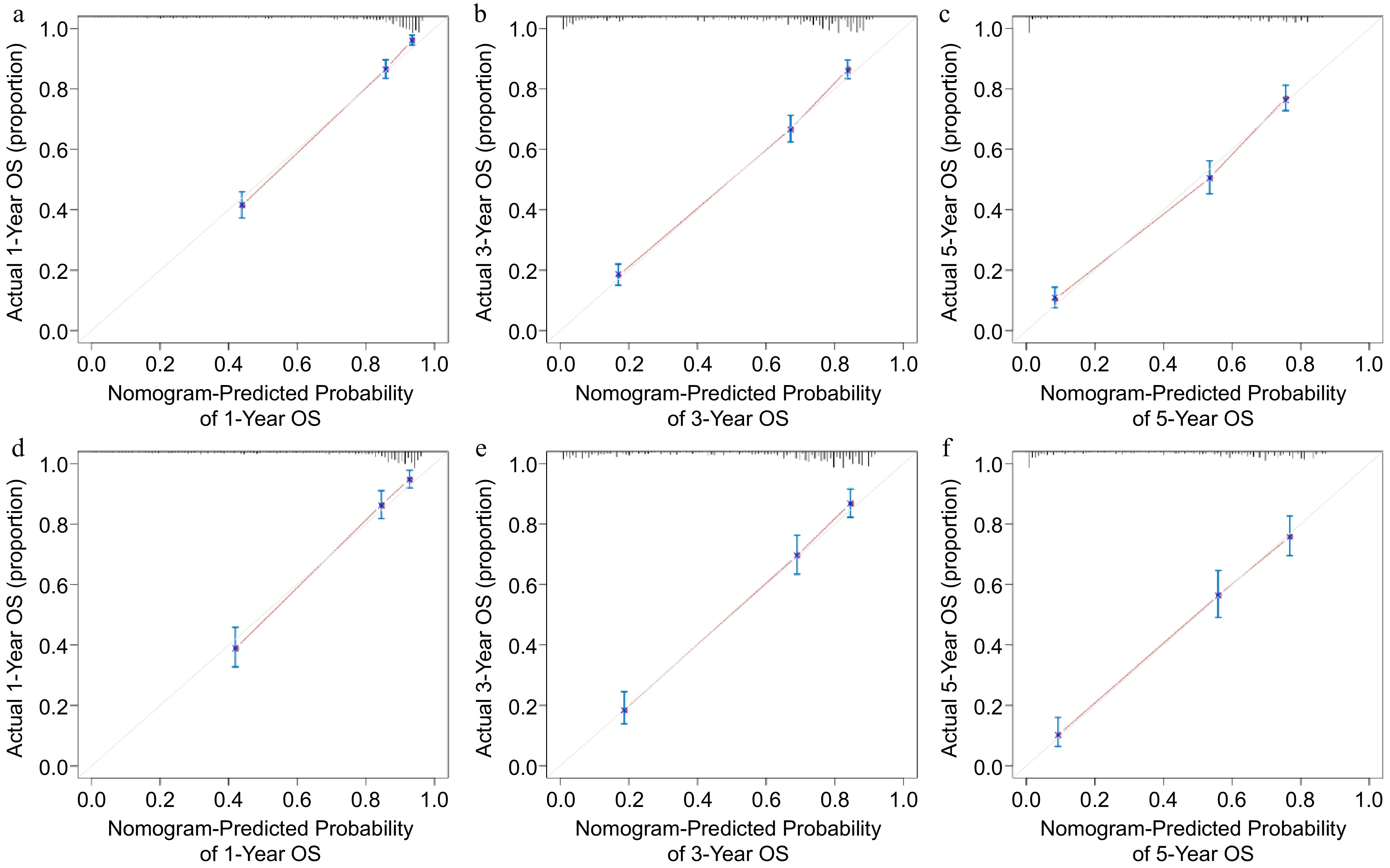
Figure 4.
Calibration curve analysis of the nomogram predicting survival probabilities. Nomogram-predicting (a) 1-year, (b) 3-year, and (c) 5-year survival probabilities in the training group. Nomogram-predicting (d) 1-year, (e) 3-year, and (f) 5-year survival probabilities in the validation group.
Validating the nomogram by C-index, ROC analysis, and DCA
-
For further evaluation of the predictive power of the prognostic nomogram, The C-index was calculated, and ROC and DCA curves were plotted for both the training and validation groups. Firstly, the C-index for stage IV GEP-NENs in the training group was 0.796 (95% CI 0.780–0.812). In terms of the validation group, C-index was 0.801 (95% CI 0.778–0.825). Secondly, as shown in Fig. 5, the AUC values of a prognostic nomogram predicting 1-, 3-, and 5-year overall survival were 0.879, 0.857, and 0.839 in the training group, significantly greater than other potential risk indicators associated with overall survival. Moreover, in the validation group, the AUC values of the nomogram estimating survival probabilities were 0.859, 0.844, and 0.831 at one, three, and five years, respectively. Similarly, the capacity of the predictive nomogram was more optimal than other risk factors (Fig. 5). Finally, DCA demonstrated that the nomogram well predicted 1-, 3-, and 5-year overall survival in the training and validation groups because it provided more clinical net benefits than two reference lines (all and none) (Fig. 6).
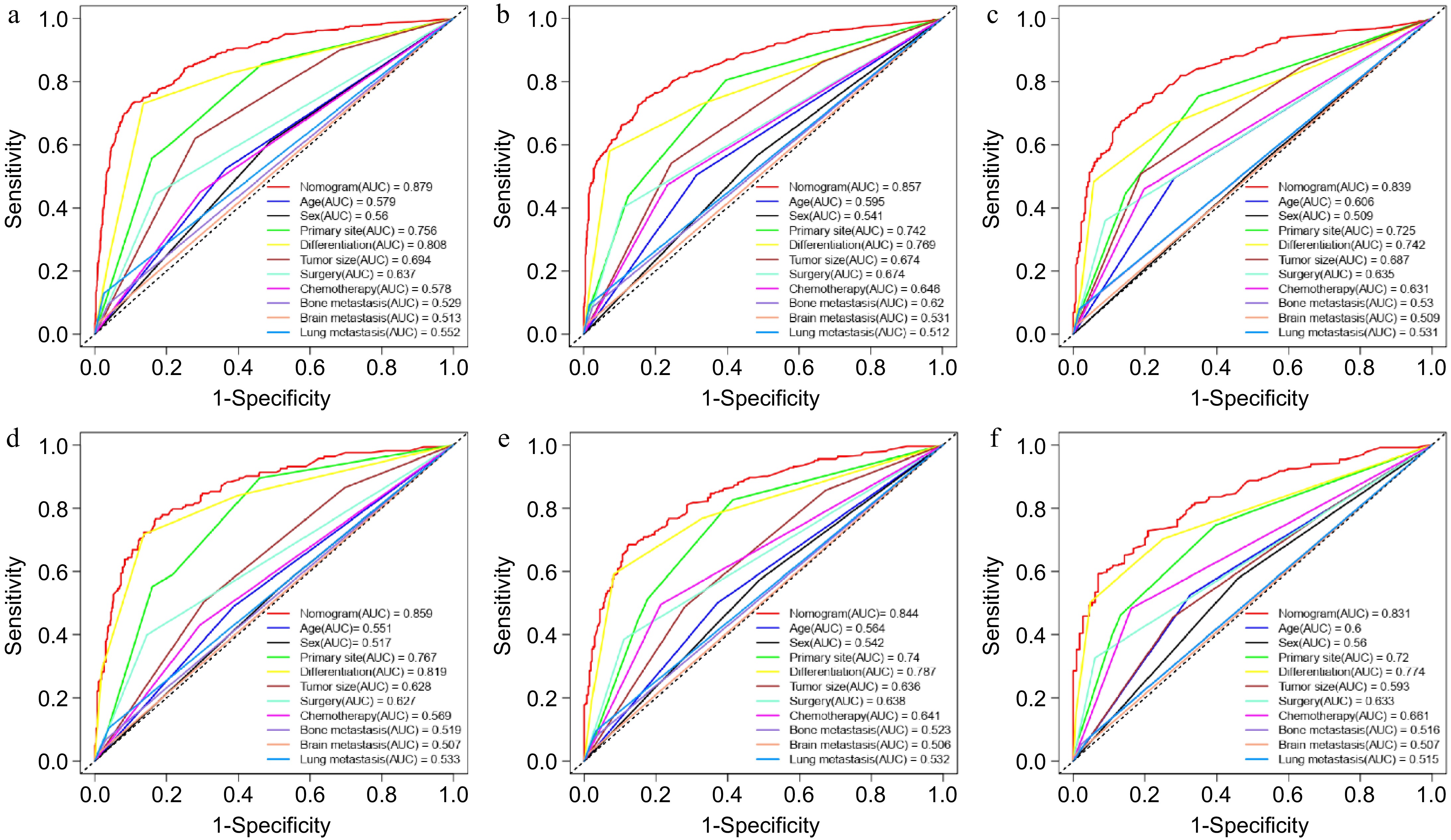
Figure 5.
ROC analysis and AUC evaluating the accuracy of nomogram- and risk factor-predicting overall survival. (a) 1-year, (b) 3-year, and (c) 5-year OS in the training group. (d) 1-year, (e) 3-year, and (f) 5-year OS in the validation group.
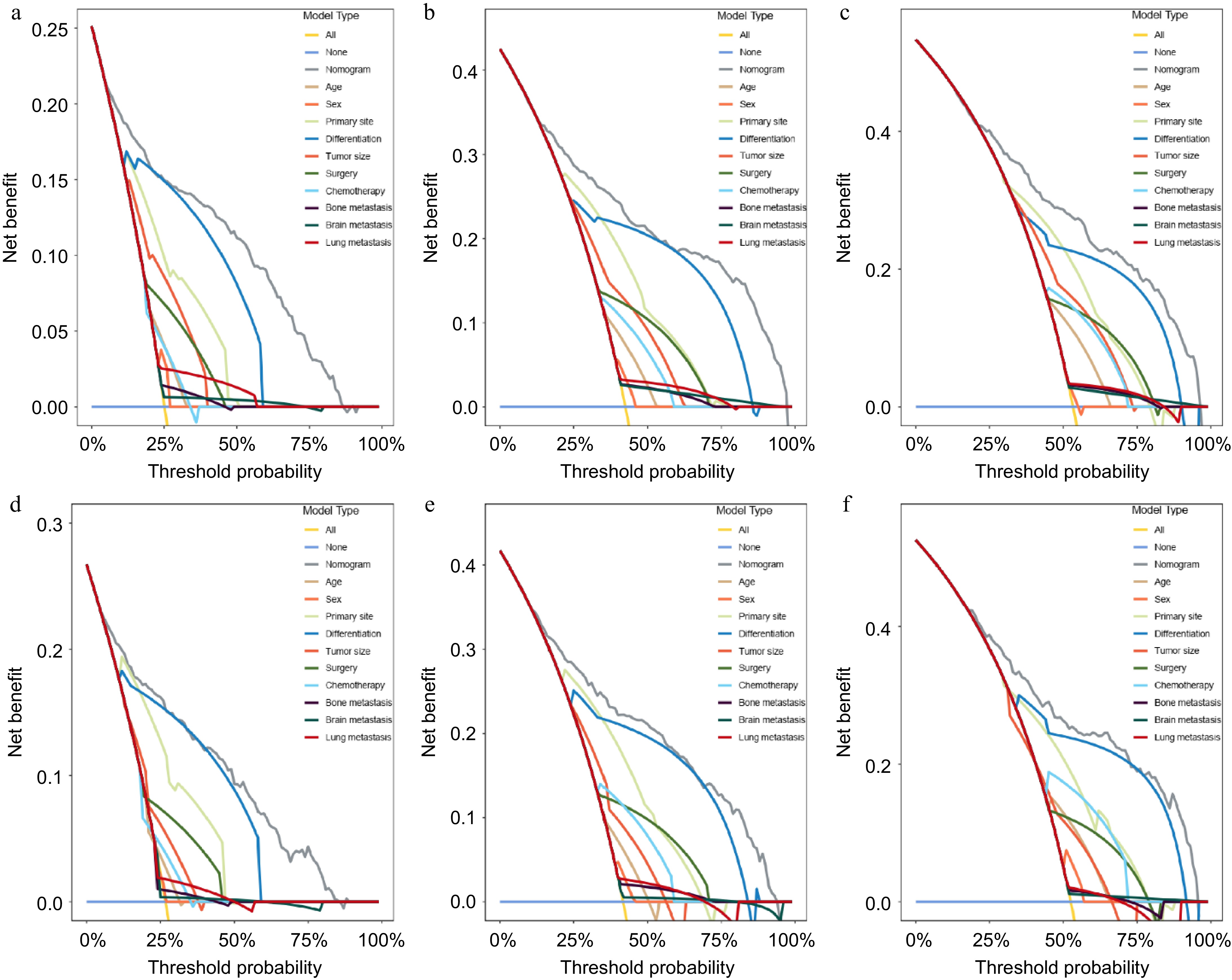
Figure 6.
DCA analysis of the clinical benefit of the nomogram- and risk factor-predicting in the training group and validation group. (a) 1-year, (b) 3-year, and (c) 5-year OS in the training group. (d)1-year, (e) 3-year, and (f) 5-year OS in the validation group.
In summary, the C-index, ROC analysis, and DCA results indicated that the prognostic nomogram based on risk factors showed favorable predictive value and clinical application.
Risk score evaluation and survival analysis
-
The correlation between risk score and survival months was evaluated using scatter plots. As shown in Fig. 7a, based on the median value of the risk score obtained from the prediction model, the training group was split into high-risk and low-risk groups. Patients in the training group with higher risk scores were observed to have decreased overall survival. (Fig. 7b). Furthermore, the validation group exhibited similar results (Fig. 7c, d). Eventually, a Kaplan-Meier analysis was conducted to estimate the prognosis between high-risk and low-risk groups. As demonstrated in Fig. 8, when compared to the low-risk group, the high-risk group had a lower number of months of survival in both the training and validation groups.
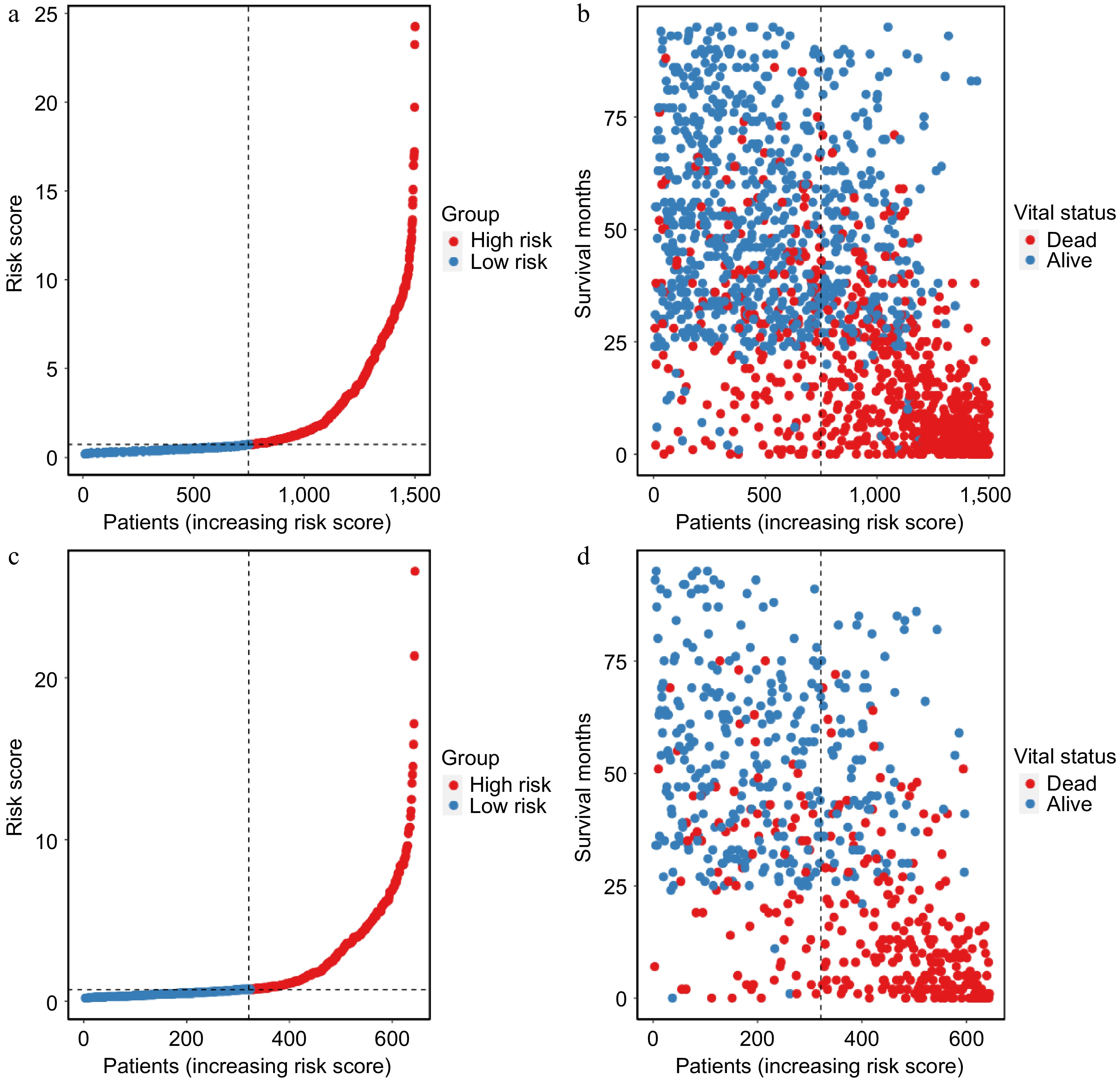
Figure 7.
Scatter plot demonstrating the risk score distribution and survival status in the (a), (b) training cohort, and the (c), (d) validation cohort.
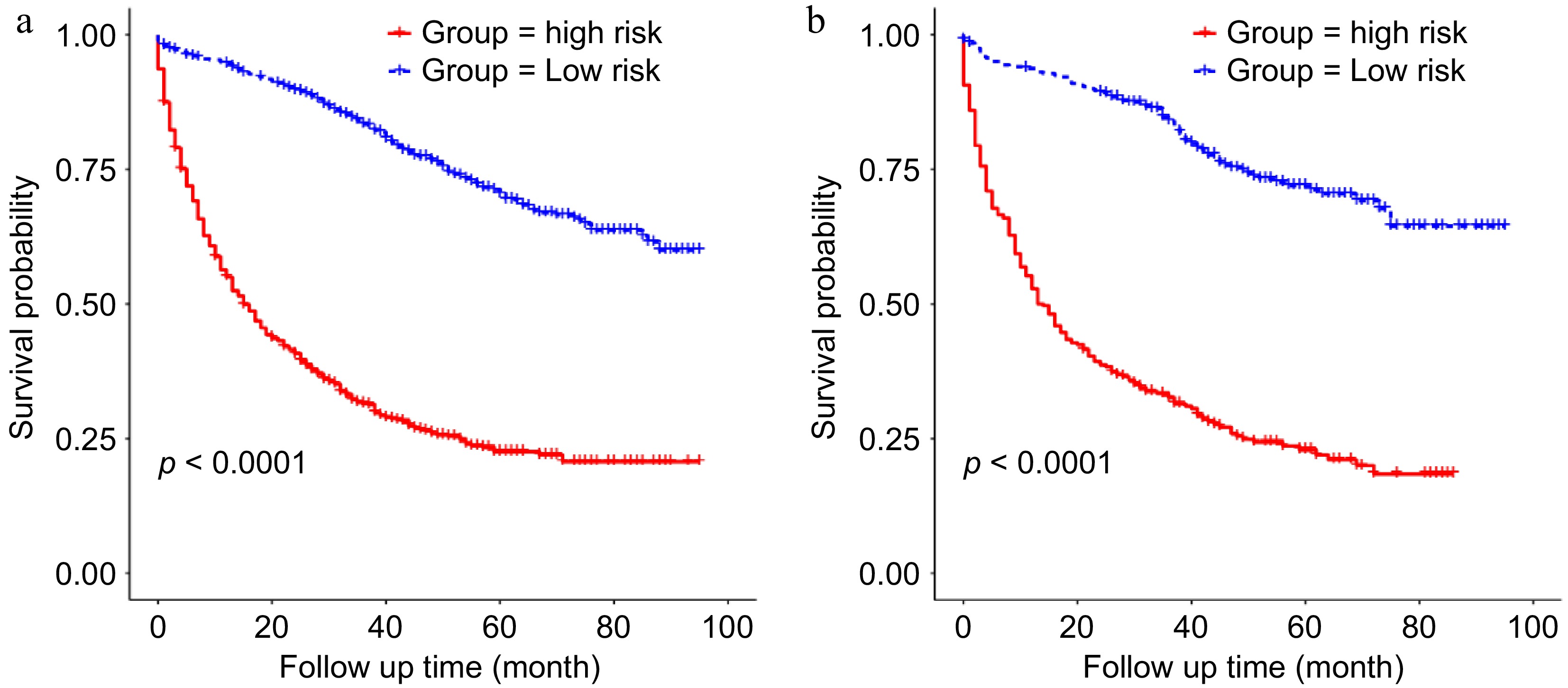
Figure 8.
Kaplan-Meier analysis of the survival difference between the high-risk and the low-risk groups based on the nomogram in the (a) training group, and the (b) validation group.
-
The neuroendocrine cells of the pancreas and the gastrointestinal tract are the sources of the GEP-NENs, a distinct subset of the NENs. Globally, the incidence of GEP-NENs has increased dramatically in recent decades[1]. Multiple treatments, including surgery, chemotherapy, and medical therapy, are available to control stage IV GEP-NENs as recommended by the European Society of Medical Oncology (ESMO) Guideline for Clinical Practice of GEP-NENs[14]. However, effective tools to predict the prognosis of stage IV GEP-NENs are still limited. The AJCC staging system as a predictive tool for malignancy prognosis was applied extensively in clinics for many years. Nevertheless, The AJCC staging method solely considers the degree of tumor invasion, the number of positive lymph nodes, and organs of distant metastases. Many essential parameters are neglected, such as age, sex, tumor size, tumor differentiation, and treatment details. Therefore, using the AJCC staging system to evaluate the survival of GEP-NENs patients is not entirely accurate. A new prognostic model urgently needs to be exploited for this population.
In this study, stage IV GEP-NENs patients were enrolled from the SEER database to develop a predictive nomogram. According to the findings of this study, potential risk factors affecting the overall survival were age, sex, primary site, tumor differentiation, tumor size, surgery, chemotherapy, and bone, brain, and lung metastases. Furthermore, a novel nomogram was developed to predict overall survival using the above risk parameters. C-index, calibration curve, ROC analysis, DCA, scatter plot of risk score, and Kaplan-Meier analysis were applied for evaluation and validation. Subsequently, the results showed excellent performance of prognostic nomograms in the training and validation groups.
This study confirmed seven out of nine risk factors as the independent risk indicators, including age, primary site, tumor differentiation, tumor size, surgery, chemotherapy, and lung metastasis. This study demonstrated that the risk of death for stage IV GEP-NENs patients aged 65 or older increased 1.715 folds (95% CI 1.4786–1.9894) compared to the patients below 65 years (Table 2); the somatic function of the elderly GEP-NENs patients was more vulnerable than young adults. The primary site was another important parameter affecting stage IV GEP-NENs patients' prognosis. From the nomogram, it was detected that the small intestine had the lowest point, followed by the pancreas, other, stomach, and colorectum. These findings were in line with the previous relevant studies[15,16]. However, the relationship between the primary site of GEP-NENs and clinical behavior is still unclear. This was mainly due to the difference in gene expression pattern and heterogeneity of different primary sites of GEP-NENs. The Tumor differentiation grade indicates tumor growth and malignant degree and is crucial in discriminating survival of stage IV GEP-NENs patients. With the increase in tumor grade, the HR of prognosis also increased (Table 2). Briefly, the higher the tumor grade, the greater the mortality risk for patients compared to those with a low grade, which was consistent with that in other studies[17,18]. In a recent study, genetic and epigenetic alterations were revealed in different grades of GEP-NENs[19,20]. Hence, the inherent genetic background determines the prognosis of different grade GEP-NENs. In terms of tumor size, the results were consistent with previous studies[21,22]. Patients with increasing tumor size also reflected tumors with more aggressive behavior[23].
Notably, this study identified surgery and chemotherapy as protective measures. ESMO guidelines suggest clinicians take multiple therapeutic schedules to treat advanced or metastatic GEP-NENs[24]. Resection of the primary site in stage IV GEP-NENs is an effective method to help reduce the tumor burden. Several studies implied that primary site resection improved the overall survival of GEP-NENs with liver metastasis[10,25,26]. Furthermore, resection of the liver metastasis and primary site or both improved clinical outcomes[27]. More importantly, resection of primary and metastatic sites is the only curative treatment of GEP-NENs. Systemic chemotherapy is another way to control disease progression. Somatostatin analogs, lutetium-177 dotatate, and the antiangiogenic agent sunitinib have been confirmed to possess antitumor properties in GEP-NENs[28−30]. Besides, as for the advanced GEP-NENs, recent studies recommended that researchers explore the genomic information and tumor microenvironment of GEP-NENs to identify the therapeutic targets[31,32].
The liver is the major metastatic site in stage IV GEP-NENs. Approximately three-quarters of all patients in this study had liver metastasis, consistent with the previous studies[33−35]. However, with or without liver metastasis, it was not considered a risk factor for stage IV GEP-NENs in this study, as the oligohepatic metastasis can be curatively resected and grow slowly. However, brain metastasis could damage the functional areas and the vital centers of the brain, inducing nerve system disorder. Bone metastasis might also cause bone damage, pathological fracture, or spinal cord compression[36]. Lung metastasis could lead to obstruction of the bronchus and pulmonary failure. These complications could seriously reduce the quality of life. Thus, brain, bone, and lung metastases were related to poor prognosis in GEP-NENs partially due to tumor burden increased lethal levels[37].
To the best of current knowledge, this is the first research that has used the SEER database to construct a nomogram that can predict the outcome of stage IV GEP-NENs. Moreover, it was validated with an internal test cohort. More importantly, all cases were retrieved from the SEER database, which has abundant information on tumor patients in the United States of America. Thus, the data from these cases is representative. In addition, the nomogram accurately predicted the prognosis of stage IV GEP-NENs patients, accounting for the clinical predictors and treatment methods. According to the nomogram, surgery, and chemotherapy could help reduce the mortality risk of stage IV GEP-NENs. What's more, the clinicopathological characteristics such as age, primary site, tumor grade, and tumor size help clinicians assess prognosis by using the prognostic nomogram. Therefore, the nomogram is clinician-friendly in evaluating the risk in stage IV GEP-NENs patients. Besides, based on the nomogram, it will be possible to integrate genomic information into nomogram construction to realize precise treatment in the future. In addition, other prognostic models of stage IV GEP-NENs included neuroendocrine prognostic score (NEP-Score)[38] and classification prognostic score developed by Sara Pusceddu et al.[39] also provided convenience to evaluate prognosis. However, based on a series of results, it seems that the prognostic nomogram exhibited better predictive capacity performance. The current study included a number of limitations. First, this retrospective study had inevitable selection bias. A larger sample size for the prospective study is needed in the future. Second, the SEER database lacked detailed information about treatment and some important indicators, including operative methods, chemotherapy regimens, targeted and immunotherapy, expression of Ki67, and genomic sequencing data. These factors are also closely correlated with the survival of GEP-NENs patients. Moreover, the predictive nomogram should be validated in an external cohort of stage IV GEP-NENs. The supplementary multicenter prospective cohort study should be implemented in the near future for this special group of patients.
-
In summary, based on the SEER database, a prognostic model for stage IV GEP-NENs was developed. In addition, the nomogram was validated, and its accuracy was preliminarily confirmed. However, external validation and prospective cohort studies are required in the future. Currently, the nomogram can assist clinicians in determining the prognosis of patients with stage IV GEP-NENs, thereby improving overall survival by identifying the associated risk factors, implementing a series of pertinent treatment measures, and strengthening follow-up.
This study was funded by Guangdong Provincial Key Laboratory of Digestive Cancer Research (Grant No. 2021B1212040006), the Youth Program of National Nature Science Foundation of China (Grant No. 82102786), the Shenzhen Science and Technology Program (Grant Nos JCYJ20190809190601671, JCYJ20230807110411024, and JCYJ20230807110718037). We acknowledged the Surveillance, Epidemiology, and End Results (SEER) Program (
https://seer.cancer.gov ) that provided the cases in this study.-
The cases in this study were obtained from SEER databases with approval (ID: 12311-Nov2021). Ethical approval and written informed consent of patients could be found in National Cancer Institute's SEER database.
-
The authors confirm contribution to the paper as follows: study conception and design, methodology, writing - draft manuscript preparation : Chen S, Feng Y; computer code and supporting algorithms implemented: Zhang W, Cheng L, Xu J; data validation : Gu L; formal analysis: Hong C; data curation: Huang Y; writing - manuscript review and editing: Zhang C, He Y; supervision of the whole study: Deng C, Sun C. All authors agreed to the final version of the manuscript.
-
All case data were obtained from the Surveillance, Epidemiology, and End Results (SEER) databases (https://seer.cancer.gov) that are publicly available.
-
The authors declare that they have no conflict of interest.
-
# Authors contributed equally: Songyao Chen, Yongxin Feng
- Supplementary Data 1 Raw data of screened stage IV GEP-NENs patients.
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Chen S, Feng Y, Zhang W, Cheng L, Xu J, et al. 2025. A prognostic nomogram of stage IV gastroenteropancreatic neuroendocrine neoplasms establishment based on the SEER database. Gastrointestinal Tumors 12: e011 doi: 10.48130/git-0025-0010 

A prognostic nomogram of stage IV gastroenteropancreatic neuroendocrine neoplasms establishment based on the SEER database
- Received: 13 January 2025
- Revised: 18 April 2025
- Accepted: 28 April 2025
- Published online: 04 June 2025
Abstract: Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs) are highly heterogeneous neoplasms of the gastrointestinal tract and pancreas. The objective of this study was to develop and verify a prediction nomogram for determining the overall survival rate of stage IV GEP-NENs. Data from 2139 stage IV GEP-NENs patients between 2010 and 2017 were extracted from the SEER database. Concordance index (C-index), calibration curve analysis, receiver operating curve (ROC) analysis, and decision curve analysis (DCA) were used to evaluate and validate the predictive performance of the nomogram. The difference in survival rates between the low-risk and high-risk groups was analyzed using the Kaplan-Meier method. Ten risk factors were integrated into the prognostic nomogram. The C-index (0.7961 in the training set and 0.801 in the validating set) and calibration curve analysis exhibited an excellent consistency between the two groups. The AUC value was 0.879, 0.857, and 0.839, respectively, for nomograms predicting 1-, 3-, and 5-year overall survival in the training set. In the validation set, AUC values were 0.859, 0.844, and 0.831 for nomograms predicting 1-, 3-, and 5-year overall survival. According to the DCA analysis, the nomogram offered significant clinical benefits. The scatter plot of risk score demonstrated that with the increase in risk score, the proportion of death also increased. In both training and validation sets, the Kaplan-Meier analysis displayed that patients in the high-risk group with stage IV GEP-NENs had a worse overall survival rate than patients in the low-risk group. A prognostic nomogram of stage IV GEP-NENs was established by integrating age, sex, differentiation, primary site, tumor size, surgery, chemotherapy, and bone, brain, and lung metastases. With further verification, the nomogram with favorable specificity, sensitivity, and added clinical benefit could help clinicians assess prognosis and provide treatment guidance for stage IV GEP-NENs patients.