










-
Colorectal cancer (CRC) is a leading cancer worldwide, ranking third in both incidence and mortality in 2020[1]. Mortality rates increase significantly with disease progression[2]. As CRC screening gains recognition for its role in preventing advanced-stage diagnoses and reducing mortality, early detection rates have shown consistent growth[3]. The American Joint Committee on Cancer's TNM classification describes early CRC as invasive cancer that remains within the mucosal and submucosal layers of the colon (Tis or T1)[4]. Conventional surgical resection, whether open or laparoscopic-assisted, has long been considered as the standard treatment for CRC[5]. However, minimally invasive options like endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are increasingly recognized as safe and effective alternatives[6−8]. Compared to surgery, endoscopic treatment (ET) is associated with fewer complications, a lower mortality risk, reduced bleeding, and a shorter hospital stay[9]. Moreover, ET usually requires curative en-bloc resection, which is mandatory and must be specifically considered as a quality parameter[10]. To qualify as a successful curative resection, patients need to meet low-risk criteria, which include submucosal invasion of less than 1,000 μm, lack of poor differentiation, no lymphovascular infiltration, and no indication of tumor budding. If any of these criteria are not met, lymph node dissection is advised to reduce the risk of lymph node or distant metastases[11].
Understanding whether endoscopic treatment provides comparable outcomes to surgery for early CRC is essential. While most research on endoscopic treatment for early-stage colorectal cancer has been carried out in Asia, limited data are available from the USA. Consequently, further investigations into endoscopic resection outcomes in the American population are necessary. This study employed the the Surveillance, Epidemiology, and End Results (SEER) database, which encompasses 34% of the US population, to examine the survival of T1 stage colorectal cancer patients who underwent either surgery or endoscopic treatment.
-
Retrospective cohort research was conducted utilizing the 'SEER Research Plus Data, 18 Registries, Nov 2020 Sub (2000−2018)' database (
https://seer.cancer.gov ). The eligibility requirements consisted of: (1) patients aged over 20 years, without limitations on gender or race; (2) individuals diagnosed with TisM0 or T1M0 colorectal adenocarcinoma (confined to the submucosa and without metastasis) through pathology, not involving the appendix and cecum; (3) only one primary tumor case and (4) those who received either endoscopic treatment (endoscopic mucosal resection, EMR; endoscopic submucosal dissection, ESD) or surgical intervention. Patients were dropped if they fulfilled any of the subsequent criteria: (1) non-adenocarcinoma histology, (2) metastatic cancer, (3) age below 20 years, (4) tumors identified solely through autopsy or death certificates, or (5) absent or unidentified information. The study applied the 7th edition of the American Joint Committee on Cancer (AJCC) TNM classification system. The collected data encompassed demographics (age, sex, race, and year of diagnosis), clinical and histological attributes(tumor size, lymph node metastases grade, TNM stage, and therapy type), survival duration, cancer-specific survival (CSS), and overall survival (OS). In the OS analysis, deaths from any cause were defined as events, while survivors were treated as censored. For the CSS analysis, only deaths due to CRC were considered events, with deaths from other causes or surviving patients regarded as censored. Patients with T1 stage CRC ('C18.0-C20.0 colon and rectum' ICD-O-3) were selected for the analysis. They were divided into two groups based on treatment: endoscopic treatment (ET) and surgery. Figure 1 shows the study population selection flowchart.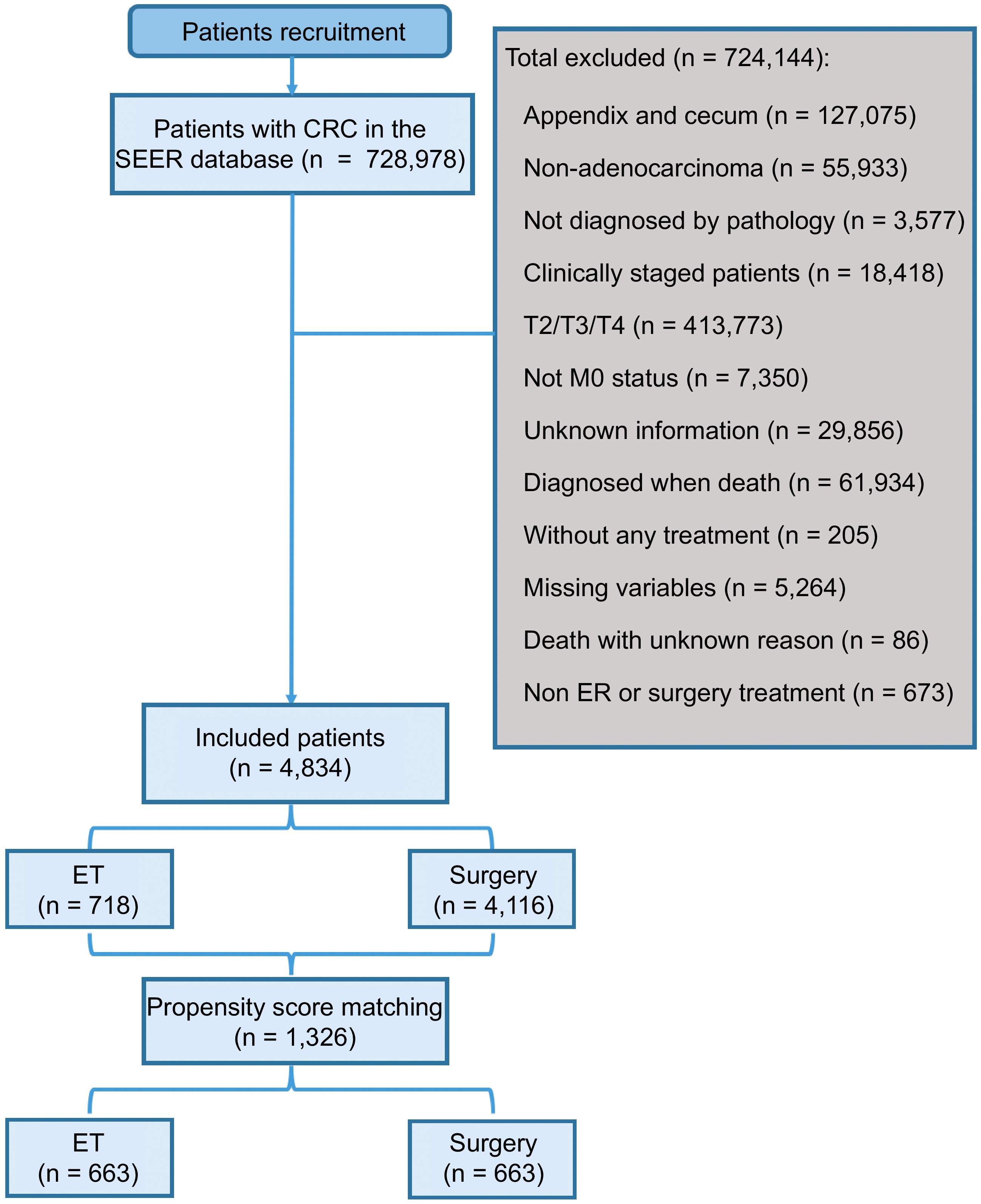
Figure 1.
Flow diagram of eligible patients diagnosed with T1 stage CRC.
This study adhered to the ethical norms established by institutional and national research committees in accordance with the principles of the 1964 Helsinki Declaration and its subsequent revisions or similar standards. The SEER Program offers anonymised data derived from population-based cancer registries. The SEER database comprises public-use data. Hence, no further approval or local ethical declaration was necessary for this work.
Statistical analysis
-
The research utilized SEER* Stat software (version 8.3.9) for data extraction. Analytical procedures were conducted using two primary statistical platforms: SPSS (version 25.0, Chicago, IL, USA) and R software (version 3.5.1, available at
www.R–project.org ). Propensity score matching was implemented to address potential baseline clinicopathological variations. The matching protocol employed a 1:1 ratio between surgical and endocrine therapy groups, with a match tolerance of 0.01. Categorical variables were assessed via the R × C Chi–squared test. Survival analysis was performed via the Kaplan–Meier method, with intergroup comparisons assessed by the log–rank test. Variables demonstrating a p–value below 0.1 in univariate analysis were further examined through a multivariate Cox proportional hazards model to ascertain independent prognostic factors. The overall survival (OS) and cancer–specific survival (CSS) rates for 3–year and 5–year intervals were assessed. Statistical significance was determined using two–sided tests, setting a threshold of p < 0.05.Additionally, subgroup analyses were conducted using Cox regression models stratified by age, sex, tumor grade, tumor location, and tumor size to explore potential heterogeneity in outcomes.
-
This study included 4,834 colorectal cancer (CRC) patients who met the inclusion criteria, among whom 4,116 (85.15%) underwent surgical intervention, while 718 (14.85%) had endoscopic treatment (ET). Figure 1 depicts the complete procedure of patient selection. In both treatment groups, the bulk of patients were between 60 and 79 years old. There were notable variations between the two groups with regard to tumor size, histological grade, lymph node metastasis (LNM), tumor site, overall stage, and T stage (p < 0.001) (Table 1).
Table 1. Baseline characteristics of patients treated with surgery and ET for T1 stage colorectal cancer before PSM.
Variables Surgery
(n = 4,116)ET
(n = 718)p-value Age (years) 20−59 970 (83.8) 188 (16.2) 0.175 60−79 2,374 (86.0) 388 (14.0) ≥ 80 772 (84.5) 142 (15.5) Marital status Unmarried 1,532 (84.8) 274 (15.2) 0.646 Married 2,584 (85.3) 444 (14.7) Sex Male 2,089 (84.8) 373 (15.2) 0.571 Female 2,027 (85.5) 345 (14.5) Race Non-API 3,840 (85.0) 675 (15.5) 0.515 API 276 (86.5) 43 (13.5) Tumor size ≤ 3 cm 2,413 (81.2) 557 (18.8) < 0.001 > 3 cm 1,703 (91.4) 161 (8.6) Histological
gradeGrade I 984 (81.4) 225 (18.6) < 0.001 Grade II 2,813 (86.3) 446 (13.7) Grade III−IV 319 (87.2) 47 (12.8) LNM Negative 3,888 (84.4) 716 (15.6) < 0.001 Positive 288 (99.1) 2 (0.9) Tumor location Colon 2,927 (90.4) 311 (9.6) < 0.001 Rectum 1,189 (74.5) 407 (25.5) Stage 0 269 (72.9) 100 (27.1) < 0.001 1 3,407 (85.0) 602 (15.0) 2 217 (93.9) 14 (6.1) 3 223 (99.1) 2 (0.9) T stage Tis 277 (73.5) 100 (26.5) < 0.001 T1 3,839 (86.1) 618 (13.9) A decreasing trend in the proportion of patients undergoing endoscopic treatment for T1 stage CRC was observed, with rates declining from 16.0% in 2000–2004 to 5.0% in 2011–2018 (p < 0.001) (Fig. 2). Furthermore, a binary multivariable logistic regression analysis indicated that tumors located in the colon, higher histological grade, and greater tumor size were strongly linked to a higher chance of receiving surgical therapy (Supplementary Table S1).
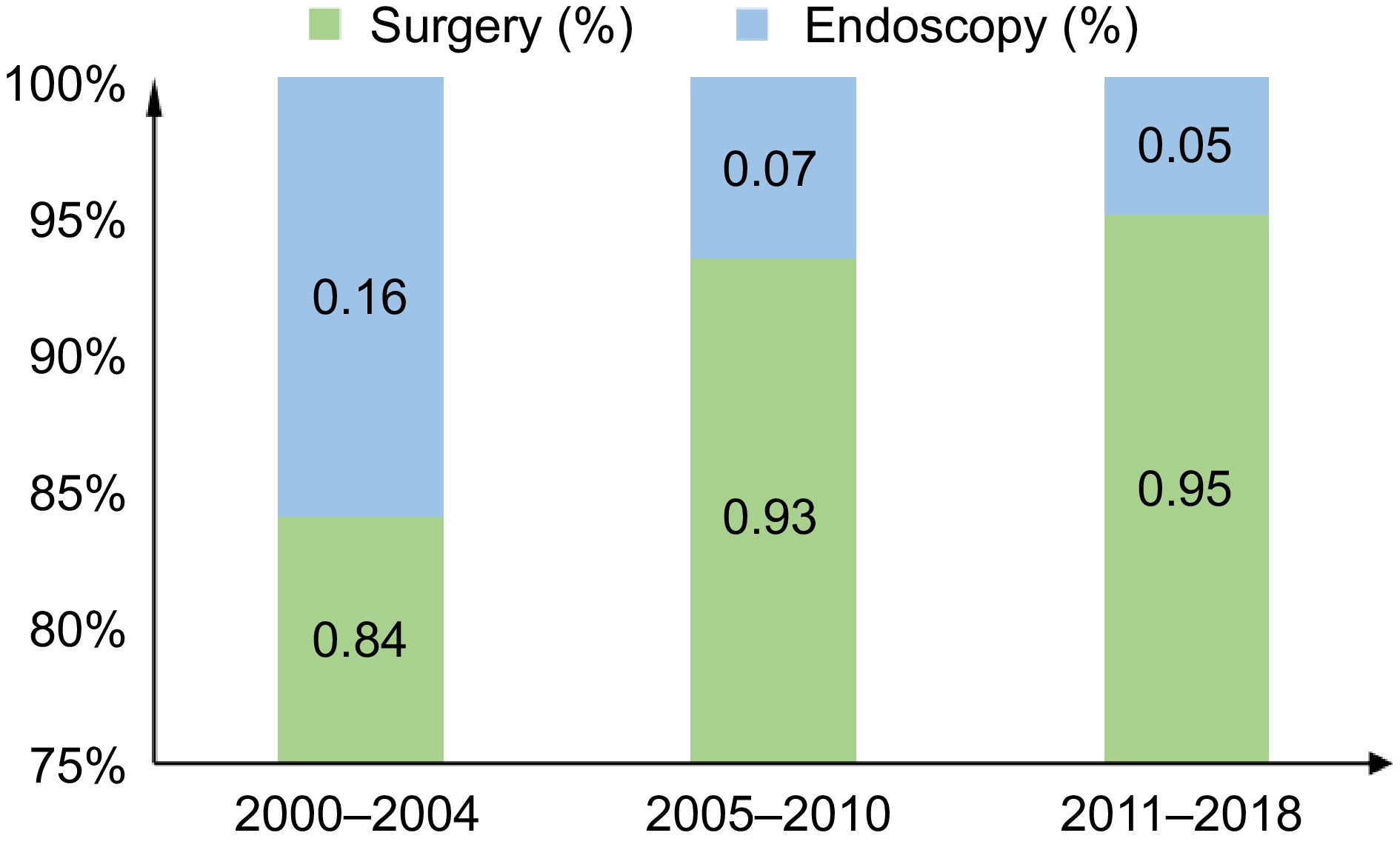
Figure 2.
Proportion of different treatments between 2000-2018.
OS and CSS comparison between ET and surgery groups
-
In this study, 437 patients (60.86%) in the ET group and 2,451 (59.55%) in the surgical group passed away. Among them, 114 patients (15.88%) who underwent ET and 469 patients (11.39%) who underwent surgical treatment were confirmed to have died from colorectal cancer (CRC).
Overall survival (OS) was comparable across the two groups. The median OS for the ET group was 141.0 months, with a 5-year OS rate of 73.3% (n = 191), while the surgery group exhibited a median OS of 146.0 months and a corresponding 5-year OS rate of 76.4% (n = 947) (p = 0.88) (Fig. 3a). However, the 5-year cancer-specific survival (CSS) rates were markedly inferior in the ET group relative to the surgical group, at 90.6% (n = 61) vs 92.9% (n = 262) (p = 0.0022) (Fig. 3b).
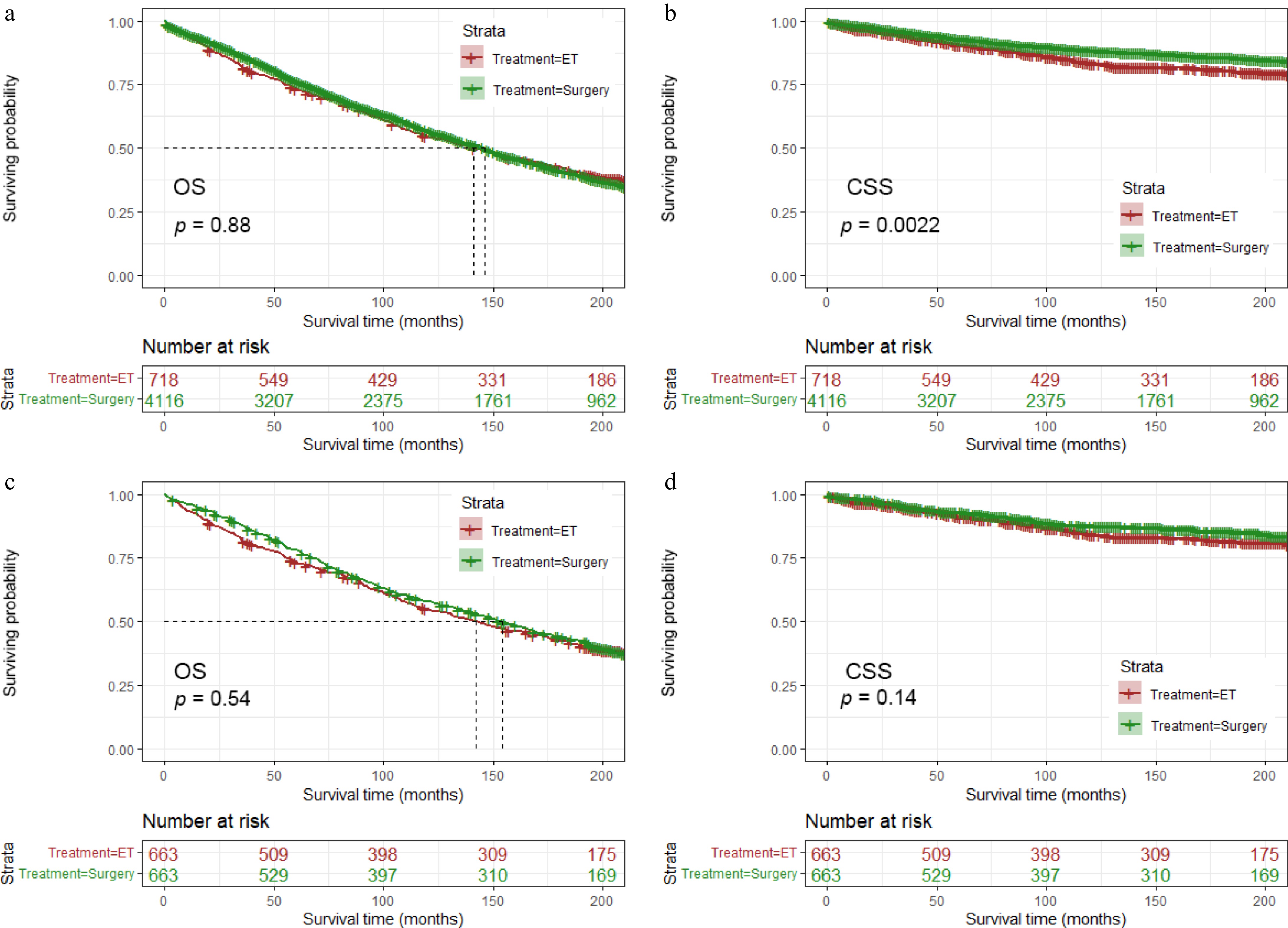
Figure 3.
Kaplan–Meier curves of overall and cancer-specific survival according to treatment methods (a), (b) before PSM, and (c), (d) after PSM.
Multivariable cox regression
-
No significant difference in mortality risk was observed between the ET and surgical groups after adjusting for other variables, including OS (HR) and CSS (HR). Older age (60–79 years HR: 3.363, 95% CI 2.963–3.816, p < 0.001; ≥ 80 years HR: 9.797, 95% CI 8.513–11.273, p < 0.001), male (HR: 1.302, 95% CI 1.205–1.407, p < 0.001), married patients (HR: 0.780, 95% CI 0.720–0.846, p < 0.001), greater tumor size (HR: 1.101, 95% CI 1.021–1.188), T stage (HR: 0.123, 95% CI 0.039–0.385) and higher stage (stage 1: HR: 7.463, 95% CI 2.362–23.580; stage 2: HR: 7.942, 95% CI 2.443–25.822; stage 3: HR: 32.986, 95% CI 2.877–387.235) exhibited a strong correlation with OS, while older age (60–79 years HR: 1.857, 95% CI 1.477–2.335, p < 0.001; ≥ 80 years HR: 3.757, 95% CI 2.866–4.926, p < 0.001), male (HR: 1.270, 95% CI 1.069–1.508, p = 0.007), married patients (HR: 0.751, 95% CI 0.628–0.897, p = 0.002), larger tumor size (HR: 1.362, 95% CI 1.153–1.610, p < 0.001), higher histological grade (Grade III–IV HR: 1.627, 95% CI 1.193–2.219, p = 0.002), tumor location in rectum (HR:1.238, 95% CI 1.041–1.473, p = 0.016) and endoscopic treatment (HR: 1.474, 95% CI 1.184–1.834) constituted independent risk factors for CSS (Table 2).
Table 2. Univariate and multivariate analyses of OS and CSS in patients with T1 stage colorectal cancer treated with surgery and endoscopy before propensity score matching.
Variables Univariate analysis Multivariate analysis CSS OS CSS OS HR (95% CI) p-value HR (95% CI) p-value HR (95% CI) p-value HR (95% CI) p-value Age (years) 20–59 Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 60–79 1.818 (1.448–2.283) < 0.001 3.409 (3.004–3.867) < 0.001 1.857 (1.477–2.335) < 0.001 3.363 (2.963–3.816) < 0.001 ≥ 80 3.818 (2.934–4.968) < 0.001 10.286 (8.963–11.805) < 0.001 3.757 (2.866–4.926) < 0.001 9.797 (8.513–11.273) < 0.001 Sex Female Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Male 1.075 (0.914–1.265) 0.384 1.073 (0.998–1.155) 0.058 1.270 (1.069–1.508) 0.007 1.302 (1.205–1.407) < 0.001 Race Non–API Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 API 1.181 (0.874–1.596) 0.278 0.774 (0.658–0.910) 0.002 1.327 (0.980–1.796) 0.068 0.918 (0.780–1.080) 0.302 Marital status Unmarried Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Married 0.685 (0.581–0.807) < 0.001 0.660 (0.612–0.710) < 0.001 0.751 (0.628–0.897) 0.002 0.780 (0.720–0.846) < 0.001 Tumor size ≤ 3 cm Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 > 3 cm 1.404 (1.193–1.652) < 0.001 1.182 (1.097–1.273) < 0.001 1.362 (1.153–1.610) < 0.001 1.101 (1.021–1.188) 0.013 Histological
gradeGrade I Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Grade II 1.177 (0.962–1.439) 0.113 1.025 (0.941–1.117) 0.569 1.156 (0.942–1.418) 0.166 1.014 (0.930–1.106) 0.753 Grade III–IV 1.725 (1.270–2.343) < 0.001 1.097 (0.942–1.276) 0.234 1.627 (1.193–2.219) 0.002 1.085 (0.931–1.265) 0.295 LNM Negative Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Positive 1.864 (1.383–2.511) < 0.001 1.004 (0.841–1.198) 0.966 0.595 (0.053–6.709) 0.674 0.248 (0.059–1.047) 0.058 T stage Tis Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 T1 0.726 (0.552–0.954) 0.022 0.836 (0.733–0.953) 0.007 0.165 (0.023–1.194) 0.074 0.123 (0.039–0.385) < 0.001 Stage 0 Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 1 0.732 (0.552–0.970) 0.030 0.858 (0.750–0.980) 0.024 4.779 (0.646–35.344) 0.125 7.463 (2.362–23.580) 0.001 2 0.669 (0.377–1.189) 0.171 0.825 (0.621–1.095) 0.183 4.965 (0.630–39.152) 0.128 7.942 (2.443–25.822) 0.001 3 1.359 (0.915–2.019) 0.129 0.849 (0.683–1.055) 0.140 16.551 (0.252–1087.739) 0.189 32.986 (2.877–387.235) 0.005 Location Colon Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Rectum 1.246 (1.056–1.472) 0.009 0.851 (0.787–0.921) < 0.001 1.238 (1.041–1.473) 0.016 0.934 (0.861–1.014) 0.101 Treatment
optionSurgery Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 ET 1.375 (1.120–1.687) 0.002 0.992 (0.896–1.098) 0.878 1.474 (1.184–1.834) 0.001 1.080 (0.970–1.203) 0.159 CI, confidence interval; CSS, cancer–specific survival; OS, overall survival; HR, hazard ratio; API, Asian Pacific Islander. Propensity score matching
-
To minimize potential biases, propensity score matching (PSM) at a 1:1 ratio with a caliper of 0.001 was implemented, yielding two well-balanced cohorts of 663 patients each in the endoscopic therapy (ET) and surgical groups. Post-PSM, no notable discrepancies were detected between the two groups regarding the baseline characteristics (p > 0.05) (Table 3).
Table 3. Baseline characteristics of patients treated with surgery and ET for T1 stage colorectal cancer after PSM.
Variables Surgery
(n = 663) n (%)Endoscopy
(n = 663) n (%)p-value Age (years) 20−59 170 (50) 170 (50) 0.991 60−79 367 (49.9) 369 (50.1) ≥ 80 126 (50.4) 124 (49.6) Marital status Unmarried 248 (49.8) 250 (50.2) 0.955 Married 415 (50.1) 413 (49.9) Sex Male 341 (49.8) 344 (50.2) 0.912 Female 322 (50.2) 319 (49.8) Race Non-API 632 (50.0) 633 (50.0) 1.000 API 31 (50.8) 30 (49.2) Tumor size ≤ 3 cm 511 (50.0) 511 (50.0) 1.000 > 3 cm 152 (50.0) 152 (50.0) Histological
gradeGrade I 198 (50.0) 198 (50.0) 1.000 Grade II 430 (50.1) 429 (49.9) Grade III-IV 35 (49.3) 36 (50.7) LNM Negative 662 (50.0) 662 (50.0) 1.000 Positive 1 (50.0) 1 (50.0) Location Colon 301 (50) 301 (50) 1.000 Rectum 362 (50) 362 (50) Stage 0 69 (49.6) 70 (50.4) 0.988 1 583 (50.1) 581 (49.9) 2 10 (47.6) 11 (52.4) 3 1 (50) 1 (50) T stage Tis 69 (49.6) 70 (50.4) 1.000 T1 594 (50) 593 (50.0) Following PSM, no substantial difference was observed in the 5-year overall survival rate and median OS between ET and surgery group (5-year OS rate: 73.3% (n = 176) vs 78.0% (n = 143), median OS: 142.0 months vs 153.0 months; p = 0.540) (Fig. 3c). Meanwhile, The 5-year CSS rates were 91.3% (n = 52) in ET group and 92.9% (n = 43) in surgery group (p = 0.14) (Fig. 3d).
In the PSM Cox regression model, the ET group exhibited no significant differences in overall survival (HR: 1.074, 95% CI 0.934–1.235, p = 0.316) and cancer-specific survival (HR: 1.273, 95% CI 0.947–1.710, p = 0.110) when compared to the surgical group. Following matching, the multivariable analysis revealed that advanced age (60–79 years HR: 3.677, 95% CI 2.892–4.675, p < 0.001; ≥ 80 years HR: 11.638, 95% CI 8.883–11.248, p < 0.001), male (HR: 1.257, 95% CI 1.079–1.465, p = 0.003) and married patients (HR: 0.762, 95% CI 0.650-0.894, p = 0.001) were significantly correlated with OS (Table 4, Fig. 4a), while older age (60–79 years HR: 1.898, 95% CI 1.269–2.838, p = 0.002; ≥ 80 years HR: 4.286, 95% CI 2.625–6.999, p < 0.001), male (HR: 1.480, 95% CI 1.072–2.044, p = 0.017), Asian Pacific Islander (API) (HR: 2.004, 95% CI 1.126–3.569, p = 0.018) and higher histological grade (Grade II HR:1.560, 95% CI 1.070–2.275, p = 0.021; Grade III–IV HR: 2.170, 95% CI 1.143–4.120, p = 0.018) were independent risk factors of CSS (Table 4, Fig. 4b).
Table 4. Univariate and multivariate analyses of OS and CSS in patients with T1 stage colorectal cancer treated with surgery and ET after PSM.
Variables Univariate analysis Multivariate analysis CSS OS CSS OS HR (95% CI) p-value HR (95% CI) p-value HR (95% CI) p-value HR (95% CI) p-value Age (years) 20–59 Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 60–79 1.811 (1.216–2.699) 0.003 3.698 (2.912–4.696) < 0.001 1.898 (1.269–2.838) 0.002 3.677 (2.892–4.675) < 0.001 ≥ 80 4.070 (2.557–6.476) < 0.001 12.375 (9.527–16.075) < 0.001 4.286 (2.625–6.999) <0.001 11.638 (8.883–11.248) < 0.001 Sex Female Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Male 1.120 (0.834–1.505) 0.452 0.915 (0.975–1.051) 0.209 1.480 (1.072–2.044) 0.017 1.257 (1.079–1.465) 0.003 Race Non–API Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 API 1.531 (0.870–2.692) 0.139 0.720 (0.497–1.043) 0.083 2.004 (1.126–3.569) 0.018 0.937 (0.644–1.362) 0.733 Marital status Unmarried Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Married 0.667 (0.495–0.899) 0.008 0.599 (0.486–0.644) < 0.001 0.733 (0.524–1.024) 0.068 0.762 (0.650–0.894) 0.001 Tumor size ≤ 3 cm Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 > 3 cm 1.242 (0.890–1.733) 0.203 1.042 (0.883–1.229) 0.627 1.164 (0.827–1.640) 0.384 1.027 (0.868–1.217) 0.754 Histological
gradeGrade I Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Grade II 1.534 (1.067–2.204) 0.021 1.043 (0.893–1.218) 0.598 1.560 (1.070–2.275) 0.021 1.145 (0.973–1.348) 0.102 Grade III–IV 2.042 (1.088–3.834) 0.026 1.084 (0.780–1.506) 0.632 2.170 (1.143–4.120) 0.018 1.121 (0.803–1.565) 0.503 Nodal status Negative Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Positive NA NA 0.050 (0.001–44.849) 0.387 NA NA NA NA T stage Tis Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 T1 1.083 (0.657–1.786) 0.754 0.910 (0.729–1.136) 0.403 1.957 (0.563–6.809) 0.291 0.641 (0.202–2.037) 0.451 Stage 0 Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 1 1.077 (0.653–1.776) 0.773 0.916 (0.734–1.143) 0.436 0.473 (0.149–1.507) 0.205 1.445 (0.463–4.511) 0.526 2 1.937 (0.565–6.641) 0.293 0.472 (0.149–1.494) 0.201 NA NA NA NA 3 NA NA NA NA NA NA NA NA Location Colon Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 Rectum 1.150 (0.853–1.550) 0.360 0.860 (0.748–0.989) 0.034 1.103 (0.808–1.505) 0.536 0.879 (0.760–1.017) 0.082 Treatment
optionSurgery Ref 1.0 Ref 1.0 Ref 1.0 Ref 1.0 ET 1.246 (0.927–1.673) 0.145 1.044 (0.908–1.201) 0.541 1.273 (0.947–1.710) 0.110 1.074 (0.934–1.235) 0.316 CI, confidence interval; CSS, cancer–specific survival; OS, overall survival; HR, hazard ratio; API, Asian Pacific Islander. 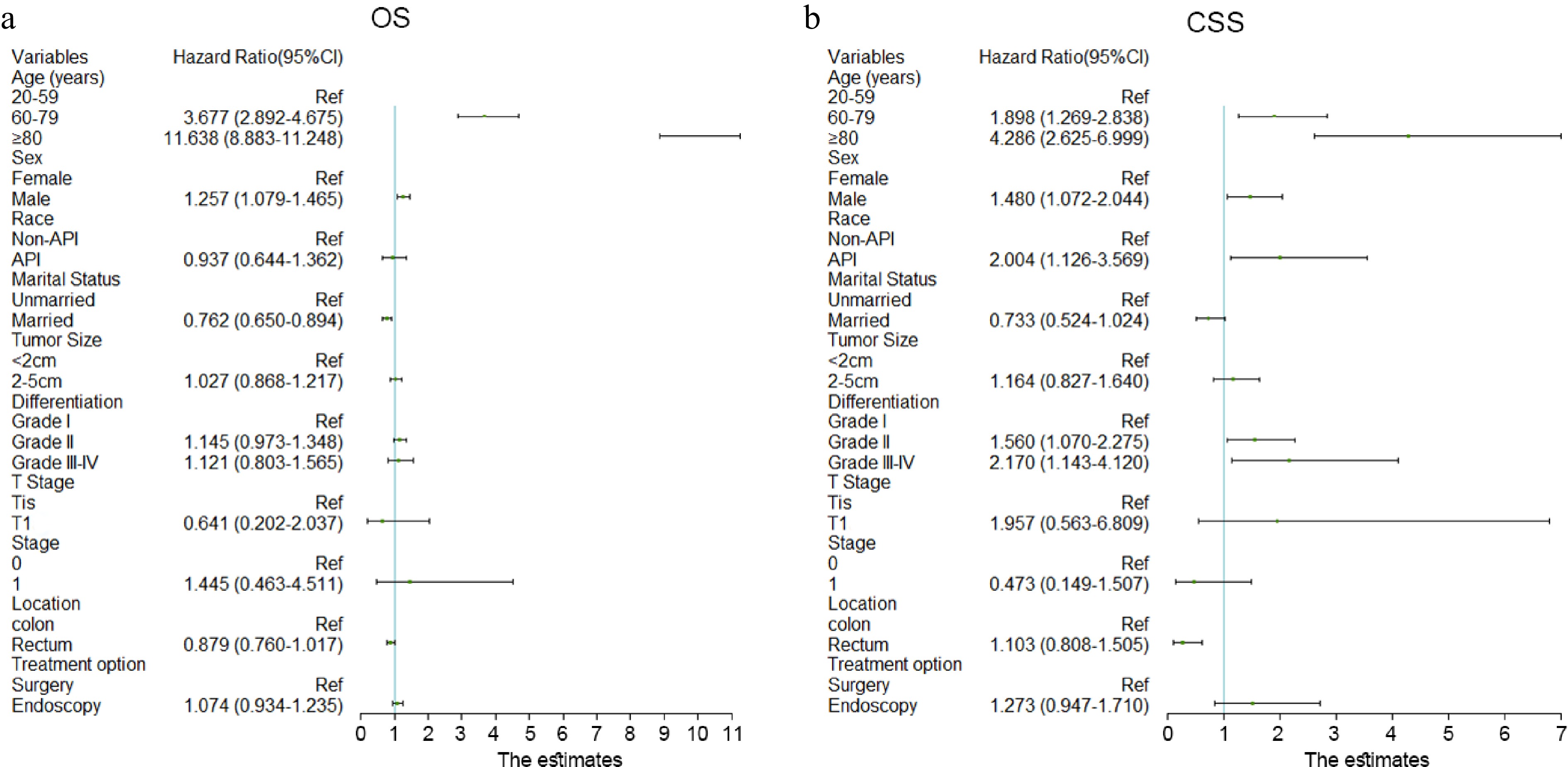
Figure 4.
Cox regression model of multivariable analyses in (a) OS, and (b) CSS.
Subgroup analysis
-
Subgroup analysis revealed that among older patients (aged 60–79 years), male patients, and those with higher histological grades, the cancer-specific survival (CSS) rates were significantly greater in the surgery group compared to the endoscopic treatment (ET) group (p = 0.0063, 0.018, and 0.00036, respectively; Fig. 5). However, no significant differences in overall survival (OS) rates were observed between the two groups (Supplementary Fig. S1).
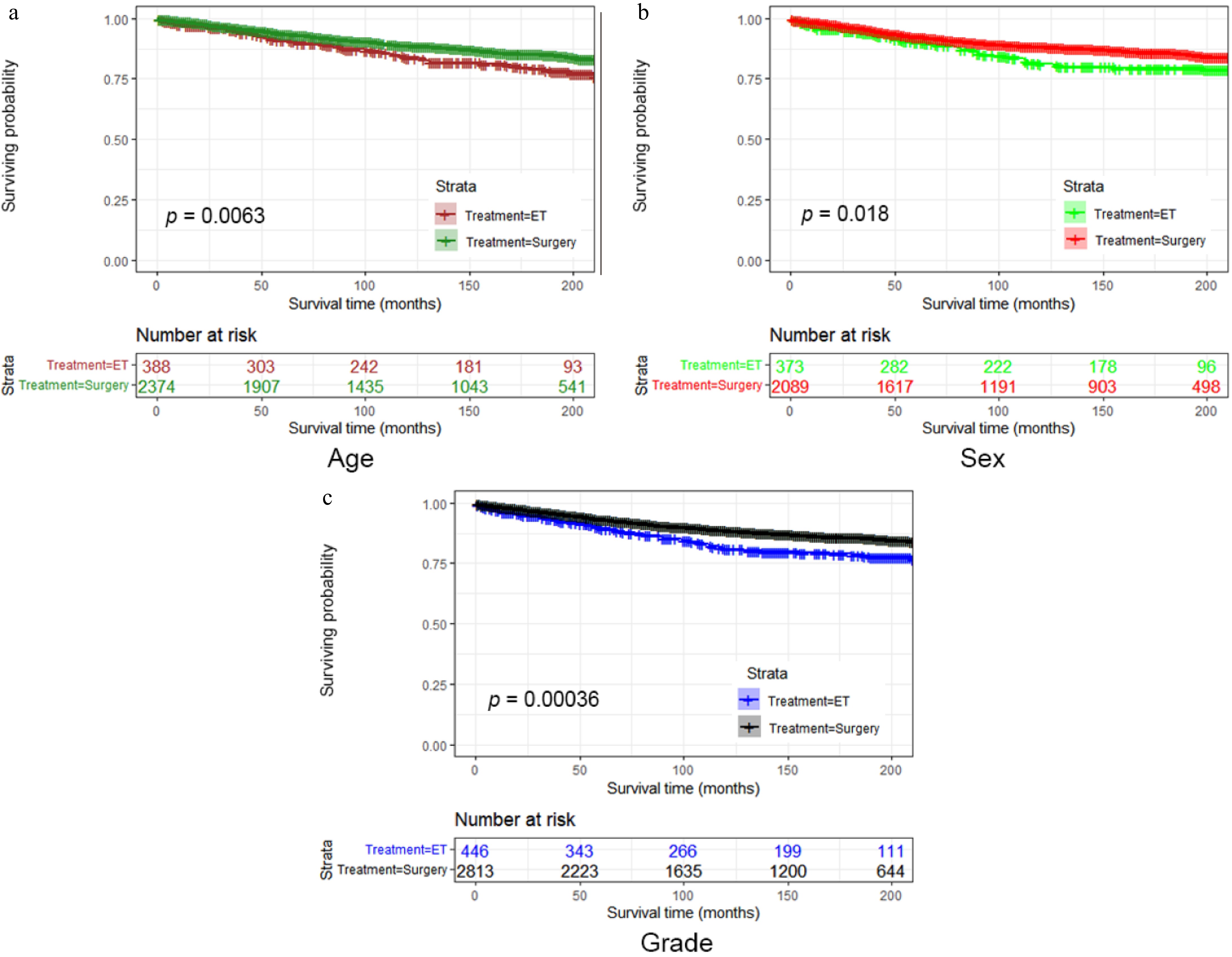
Figure 5.
Subgroup analysis divided by (a) age, (b) sex, or (c) histological grade of the CSS rate by the two treatment options.
For other subgroups, including tumor size, disease stage, and tumor location, no statistically significant differences were identified between the ET and surgery groups in terms of both OS and CSS rates.
-
With the advancement of endoscopic screening methods, endoscopic treatments have become a well-established option for early colorectal cancer (CRC), leading to a higher rate of complete resections[12]. Numerous studies have assessed the effectiveness and safety of endoscopic resection for early CR[13,14]. However, there is limited research directly comparing endoscopic resection with surgical treatment for early-stage CRC, particularly among Western populations. In this study, overall survival (OS) and cancer-specific survival (CSS) were evaluated in patients undergoing endoscopic resection vs surgical treatment. To ensure a more accurate comparison, the following approaches were applied: (1) a propensity score matching (PSM) algorithm to minimize confounding factors, including tumor size, histological grade, lymph node metastasis (LNM), stage, and tumor location; (2) competing risk regression as an alternative to Cox regression, accounting for competing survival outcomes, such as tumor-specific mortality and mortality from other causes.
Surgical resection remains the primary treatment modality for early-stage gastrointestinal cancers due to its advantages in achieving complete tumor removal and lymph node dissection[15]. However, it is often associated with significant postoperative morbidity and mortality rates[16]. In contrast, endoscopic treatment (ET) offers a minimally invasive alternative with lower complication rates, reduced mortality, and better preservation of organ function, thereby enhancing the quality of life. The primary indications for ET include mucosal (Tis) and superficial submucosal (T1a) cancers without lymph node involvement in CRC[17]. Despite the advancements in endoscopic techniques, a declining trend in the use of ET for T1-stage colorectal cancer (CRC) was observed from 2000 to 2018, while surgical treatment rates remained higher. This may be attributed to certain limitations of ET, which can hinder its widespread adoption in Western populations. Endoscopic procedures may pose a higher risk of intraoperative complications, including bleeding and perforation, and may result in positive margins due to the challenges in accurately defining tumor boundaries[18].
A major concern with endoscopic resection of early-stage CRC is the potential for lymph node (LN) metastasis[19]. Studies have reported that approximately 10% of submucosal colon cancers are associated with LN metastasis[20]. According to the guidelines established by the Japanese Society for Cancer of the Colon and Rectum (JSCCR), for CRC cases treated with endoscopic resection, surveillance is recommended in instances where the tumor is a differentiated adenocarcinoma with submucosal invasion of less than 1,000 µm, no vascular invasion, low-grade tumor budding (grade 1), and negative horizontal margins. Conversely, submucosal cancers not meeting these criteria should be considered for additional surgical intervention with lymph node dissection[21].
This study demonstrated that the OS and CSS rates in the endoscopic treatment and surgical resection groups were comparable among Western populations, aligning with findings from prior studies conducted in Asian countries[22−24]. Although initial comparisons before PSM indicated a higher CSS rate in the surgery group, this result may have been influenced by confounding factors due to differences in pathological characteristics between the two groups. After adjusting for these confounding variables, no statistically significant differences in CSS were observed. While previous studies have established the safety and efficacy of ET, with long-term survival outcomes comparable to those of surgical resection, ET remains unsuitable in certain cases. Notably, the subgroup analysis revealed significantly lower CSS rates in the ET group, particularly among older patients, male patients, and those with higher histological grades. These findings suggest that early-stage colorectal cancer (CRC) patients exhibiting these characteristics may benefit more from surgical resection to achieve improved survival outcomes.
This research possesses multiple limitations. Initially, as a retrospective analysis, the selection of subjects is based on historical data rather than random assignment, which may result in samples that are not representative of the actual target population. It is inherently susceptible to selection bias. There were notable imbalances between the two groups in key factors, including tumor size, histological grade, lymph node metastasis, tumor location, and stage. While propensity score matching was implemented to mitigate selection bias, the possibility of residual biases remains, which could have influenced the findings. Second, the absence of certain critical parameters in the dataset, including information on procedure-related complications, tumor resection margins, management of recurrence, detailed depth of infiltration, and details regarding the type of endoscopic (EMR or ESD) or surgical approach (open or laparoscopic), may have impacted the accuracy of this analysis. At the same time, it cannot be ignored that the pathological evaluation after conventional endoscopic surgery (including ESD and EMR) will list the depth of invasion of the lesion in the submucosal layer in more detail (such as T1a and T1b). Unfortunately, the seer database fails to provide such information. Lastly, given the generally high 5-year survival rates for early-stage colorectal cancer, identifying substantial disparities in survival outcomes between the ET and surgical cohorts may have proven difficult. A 10-year survival analysis would provide a more comprehensive evaluation of long-term outcomes. However, the limited follow-up duration within the SEER database restricted the study's ability to assess 10-year survival rates. Despite these limitations, the study is notable for being the first to conduct a direct comparison of long-term survival outcomes between ET and surgical treatment. Additionally, as a population-based study with substantial sample size and extended follow-up duration, the results offer valuable insights and contribute to the existing body of evidence in this field.
-
In conclusion, this study demonstrated no significant difference in long-term survival between the endoscopic treatment (ET) and surgery groups for T1-stage colorectal cancer. Consequently, endoscopic resection could be a suitable alternative for patients ineligible for surgery due to comorbidities or other considerations. However, surgical resection may be a more appropriate choice for older individuals and those with tumors of higher histological grade. Given the limitations of this study, further prospective multicenter investigations are recommended to corroborate these findings and furnish more substantial data.
-
This study utilized public-accessible data from the Surveillance, Epidemiology, and End Results (SEER) database provided by the National Cancer Institute (NCI). Approval from an institutional review board and informed consent were unnecessary for the current investigation due to the public availability of SEER research data and the de-identification of all patient information. Therefore, no ethics committee approval was required for this study.
The authors would like to express their gratitude to the NCI and the SEER program team for providing valuable data resources to researchers. The authors also extend their appreciation to colleagues and collaborators who provided support and guidance during data collection, analysis, and manuscript preparation. This study was supported by a grant from the National Natural Science Foundation of China (Grant No. 82100594).
-
The authors confirm contribution to the paper as follows: conceptualization, project administration: Zhou X, Zhang G; methodology: Su W, Chen H; formal analysis, writing - original draft: Su W, Chen H, Hu D; investigation, writing - review and editing: Su W, Chen H, Hu D, Li X, Si X, Ye B; supervision: Zhou X, Ye B. All authors reviewed the results and approved the final version of the manuscript.
-
Data is included in the manuscript or additional information files. The datasets utilized and examined in this investigation are obtainable from the relevant author upon a reasonable request.
-
The authors declare that they have no conflict of interest.
-
# Authors contributed equally: Wei Su, Han Chen, Die Hu
- Supplementary Table S1 Factors predicting the use of surgery for treatment of T1 stage CRC in multivariable analysis.
- Supplementary Fig. S1 Subgroup analysis divided by age (a), sex (b) or histological grade (c) of the OS rate by the two treatment options.
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Su W, Chen H, Hu D, Li X, Si X, et al. 2025. Endoscopic treatment vs surgery for T1-stage colorectal cancer: a real-world retrospective cohort study. Gastrointestinal Tumors 12: e010 doi: 10.48130/git-0025-0011 

Endoscopic treatment vs surgery for T1-stage colorectal cancer: a real-world retrospective cohort study
- Received: 30 December 2024
- Revised: 07 April 2025
- Accepted: 09 May 2025
- Published online: 30 May 2025
Abstract: Endoscopic treatment is widely used for T1 colorectal cancer, yet there are limited studies that compare the survival outcomes of patients treated with endoscopy and surgery. This study utilized the data from the Surveillance, Epidemiology, and End Results database to evaluate the long-term survival of the two treatment regimens in America. The analysis of T1-stage colorectal cancer patients from 2000 to 2018 was assessed using Kaplan-Meier analyses and log-rank tests. Accounting for the imbalance in covariate distribution between the two groups, a propensity score matching method was employed, followed by a comparison of survival outcomes. Of the 4,834 patients included in this study, 4,116 underwent surgery, while 718 underwent endoscopic procedures. Overall survival did not significantly differ between the groups prior to the use of the propensity score matching method, but the surgery group's cancer-specific survival was noticeably higher (p = 0.0022). Following propensity score matching, there were no discernible variations in overall or cancer-specific survival. Subgroup analysis indicated that older patients, males, and those with higher histological grades had significantly better cancer-specific survival outcomes with surgery compared to endoscopic treatment. According to data from the American population, there was no variation in long-term survival rates for T1-stage colorectal cancer between the two groups.
-
Key words:
- Colorectal cancer /
- T1 stage /
- SEER /
- Surgery /
- Endoscopic treatment