







-
Smoking tobacco continues to be a significant worldwide public health issue, greatly adding to the incidence of illness and death[1]. It is a significant risk factor for various cancers, such as those affecting the lungs, mouth, bladder, cervix, liver, kidneys, and pancreas, in addition to chronic obstructive pulmonary disease (COPD), and heart-related issues[1]. Smoking ranks among the top contributors to preventable deaths globally, accounting for around seven million deaths each year, and increasing susceptibility to six out of the eight most common causes of mortality[1].
The overall deaths linked to tobacco are anticipated to increase from 5.4 million in 2005, to 6.4 million in 2015, and reach 8.3 million in 2030, with around 600,000 deaths due to secondhand smoke[1,2]. These forecasts rely on models indicating a three- to four-decade delay between the increase in smoking rates and the subsequent rise in mortality attributable to smoking. A 50-year study revealed that smokers tend to have a lifespan that is approximately 10 years shorter than that of non-smokers. Recent scientific findings indicate that smoking not only harms the smoker, but also poses risks to those nearby, increasing the chances of lung cancer and various other ailments[3].
In 2012, approximately 207 million women and 928 million men were smokers. In 2021, it was estimated that more than 1.3 billion people smoked cigarettes worldwide, with 80% of these smokers living in low- and middle-income countries[4]. The highest rates of male smoking are currently found in East and Southeast Asia, along with Eastern Europe. The highest percentages of female smokers are located in North and South America, Oceania, and Europe[1,2,4,5].
The use of tobacco is increasing by approximately 8% each year in developing countries; Asia, and Southern and Eastern Europe[6]. Nonetheless, tobacco use is declining by approximately 1% annually in numerous developed countries, primarily due to the implementation of robust anti-smoking campaigns[7]. The exact date, duration, and intensity of the smoking epidemic vary significantly from country to country, similar to other outbreaks that involve a major behavioral aspect. Approximately 20% of men and 2% of women in Iran, a country neighboring Iraq, use tobacco products[8]. According to the health survey conducted in Turkey in 2022, prevalence increased by 20% between 2012 and 2022, to 32.1%, and the frequency of women using tobacco products increased by 38.3%[9]. In Iraq, several small studies were conducted investigating the smoking prevalence in some groups, such as students. One study conducted, recruiting preparatory and secondary schools revealed that 21.8% of Iraqi adolescents smoke tobacco, with 27.1% being males, and 12.7% females. A nationwide online questionnaire survey conducted in 2021 showed that the overall smoking rate in Iraq within our sample was 22.44%[4]. The only similar study in Zakho is a cross-sectional study examining prevalence and predictors of smoking among school adolescent males, where 51.7% of participants were daily smokers, and the most critical factors associated with the initiation of smoking were age, peer influence, and if participants' fathers smoked[10]. This, however, does not represent the general population of the region, and, to the best of our knowledge, no population-based study has been conducted in our region to investigate the prevalence of smoking and associated factors. The aim of our study was to investigate the prevalence and associated factors of smoking in Zakho city, Kurdistan Region, Iraq.
-
An observational cross-sectional study was conducted within a single day in January 2024 among adults aged 18 years and above who met the eligibility criteria. In the first stage of a multistage sampling method, six districts were randomly selected from the main residential areas of Zakho city. According to the most recent demographic statistics from the Kurdistan Region Statistics Office, these districts are comparable to the overall population of Zakho (398,878) in terms of household size, age distribution, and socioeconomic characteristics, supporting their representativeness. In the second stage, households within each selected district were chosen using a computer-generated random number sequence. A minimum sample size of 384 participants was calculated using a proportion of p = 0.5 to maximize sample variability. Adults aged ≥ 18 years who agreed to participate were included, while individuals younger than 18 years, or those who declined participation were excluded. A total of 537 participants were ultimately enrolled, with a mean age of 35.73 ± 13.95 years.
Data collection
-
A structured questionnaire administered by an interviewer, which was pretested for clarity and reliability, was utilized to collect data. The questionnaire aimed to gather information regarding the participants' clinical characteristics, behavioral tendencies, and sociodemographic attributes.
Participants' physical health was assessed through anthropometric measurements alongside the questionnaire. To maintain consistency, height was measured with participants standing straight, and weight was documented with a precise weighing scale to ensure accuracy. Body Mass Index (BMI) was calculated from this information using the standard method, which involves weight (kg) divided by height (m). Waist circumference was determined by positioning a tape measure at the area between the lowest rib margin and the upper part of the iliac crest around the body. A waist circumference of 94 cm or less in men, and 80 cm or less in women was deemed normal, whereas a waist circumference exceeding 94 cm in men, and 80 cm in women was considered high. Physical activity refers to any movement of the body produced by skeletal muscles that results in energy expenditure. Individuals who had an education level of middle school or higher were categorized as educated, and participants who reported actively smoking at the time of the interview were classified as current smokers. HBA1c was measured by the high-performance liquid chromatography (HPLC) method, and a level equal to, or more than 6.5% was regarded as diabetic.
Statistical analysis
-
The dataset was subjected to coding, cleaning, and verification prior to its entry into Microsoft Excel for preliminary processing. It was subsequently moved to IBM SPSS Statistics (Version 26.0, launched in 2019) for an in-depth statistical evaluation using binary logistic regression to generate odds ratios (OR), 95% confidence intervals (95% CI), and p-values. Variables exhibiting a p-value < 0.2 were chosen for incorporation into a multivariable logistic regression model. A p-value < 0.05 was deemed statistically significant, suggesting substantial evidence of a relationship between independent variables and the outcomes of interest.
-
Socio-demographic and clinical characteristics of study participants are presented in Table 1. A total of 537 participants were included in the analysis, of which 345 (64.2%) were males, and 192 (35.8%) were females. Their age ranged from 18 to 90 years, with a mean of 35.73 ± 13.95 standard deviation. More than two-thirds (68%) of the participants were educated, about 60.3% were married, and 53.1% were employed.
Table 1. Characteristics of study participants.
Variables Male n (%) Female n (%) Total n (%) Smoking status Smoker 165 (47.8%) 15 (7.8%) 180 (33.5%) Non-smoker 180 (52.2%) 177 (92.2%) 357 (66.5%) Age (years) 18–30 126 (36.5%) 93 (48.4%) 219 (40.8%) 31–40 97 (28.1%) 50 (26%) 147 (27.4%) 41–50 69 (20%) 26 (13.5%) 95 (17.7%) 51–60 36 (10.4%) 11 (5.7%) 47 (8.8%) 61–70 10 (2.9%) 6 (3.1%) 16 (3%) > 70 7 (2%) 6 (3.1%) 13 (2.4%) Education status Uneducated 111 (32.2%) 61 (31.8%) 172 (32%) Educated 234 (67.8%) 131 (68.2%) 365 (68%) Marital status Single 114 (33%) 99 (51.6%) 213 (39.7%) Married 231 (67%) 93 (48.4%) 324 (60.3%) Employment status Unemployed 112 (32.5%) 140 (72.9%) 252 (46.9%) Employed 233 (67.5%) 52 (27.1%) 285 (53.1%) Physical activity Yes 154 (44.6%) 64 (33.3%) 218 (40.6%) No 191 (55.4%) 128 (66.7%) 319 (59.4%) Sleep disturbance Yes 127 (36.8%) 69 (35.9%) 196 (36.5%) No 218 (63.2%) 123 (64.1%) 341 (63.5%) Hypertension Yes 31 (9%) 20 (10.4%) 51 (9.5%) No 314 (91%) 172 (89.6%) 486 (90.5%) Hyperlipidemia Yes 58 (16.8%) 17 (8.9%) 75 (14%) No 287 (83.2%) 175 (91.1%) 462 (86%) Ischemic heart disease Yes 15 (4.3%) 5 (2.6%) 20 (3.7%) No 330 (95.7%) 187 (97.4%) 517 (96.3%) Thyroid disease Yes 10 (2.9%) 6 (3.1%) 16 (3%) No 335 (97.1%) 186 (96.9%) 521 (97%) Waist circumference Normal 188 (54.5%) 75 (39.1%) 263 (49%) High 157 (45.5%) 117 (60.9%) 274 (51%) Body mass index (BMI) Underweight 10 (2.9%) 8 (4.2%) 18 (3.4%) Normal 116 (33.6%) 63 (32.8%) 179 (33.3%) Overweight 146 (42.3%) 63 (32.8%) 209 (38.9%) Obese 73 (21.2%) 58 (30.2%) 131 (24.4%) Diabetes Non-diabetic 10 (2.9%) 8 (4.2%) 18 (3.4%) Diabetic 335 (97.1%) 184 (95.8%) 519 (96.6%) Prevalence of smoking and related factors
-
The overall prevalence of smoking was 180 (33.5%). About half of males, 165 (47.8%), were smokers, while only 15 (7.8%) females were smokers (Fig. 1). The distribution of smoking status across age groups showed no significant association (p > 0.05 for all comparisons) (Table 1). Participants aged ≤ 30 years represented the largest group (70.8% non-smokers, 29.2% smokers) (Fig. 2). Various factors were examined for potential association with smoking habits, and the following factors were significantly associated with smoking: gender, education, employment status, physical activity, and hypertension (p = 0.001, 0.016, 0.001, 0.016, and 0.03), respectively. Marital status was significantly associated with smoking in univariate analysis (p = 0.002), but the association was lost after taking it into multivariate analysis (p = 0.423). No association was found between smoking and a history of hyperlipidemia, ischemic heart disease, thyroid disorders, diabetes, waist circumference, and BMI (p > 0.05). Table 2 illustrates the factors that are potentially associated with smoking behavior.
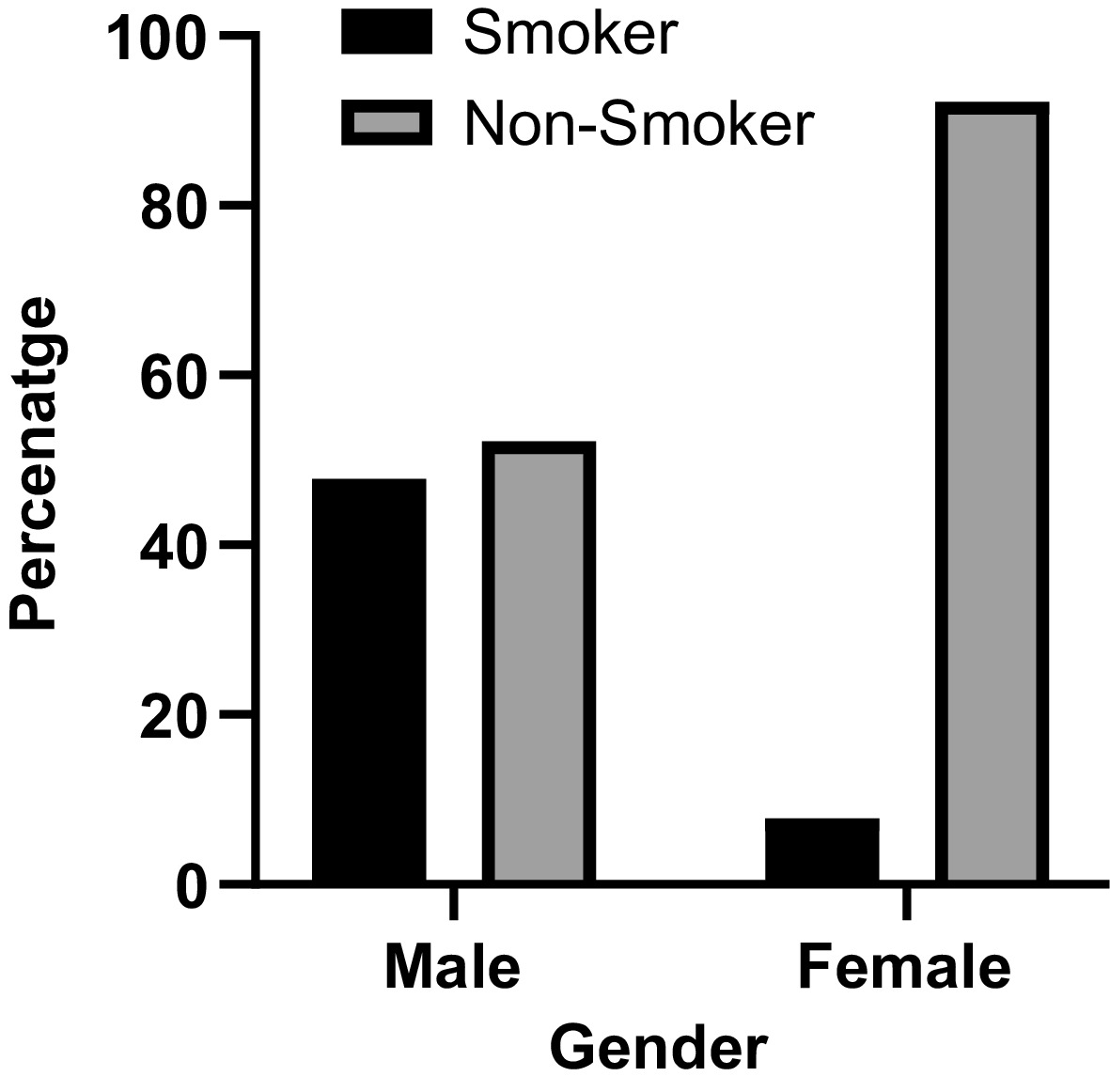
Figure 1.
Prevalence of smoking according to gender.
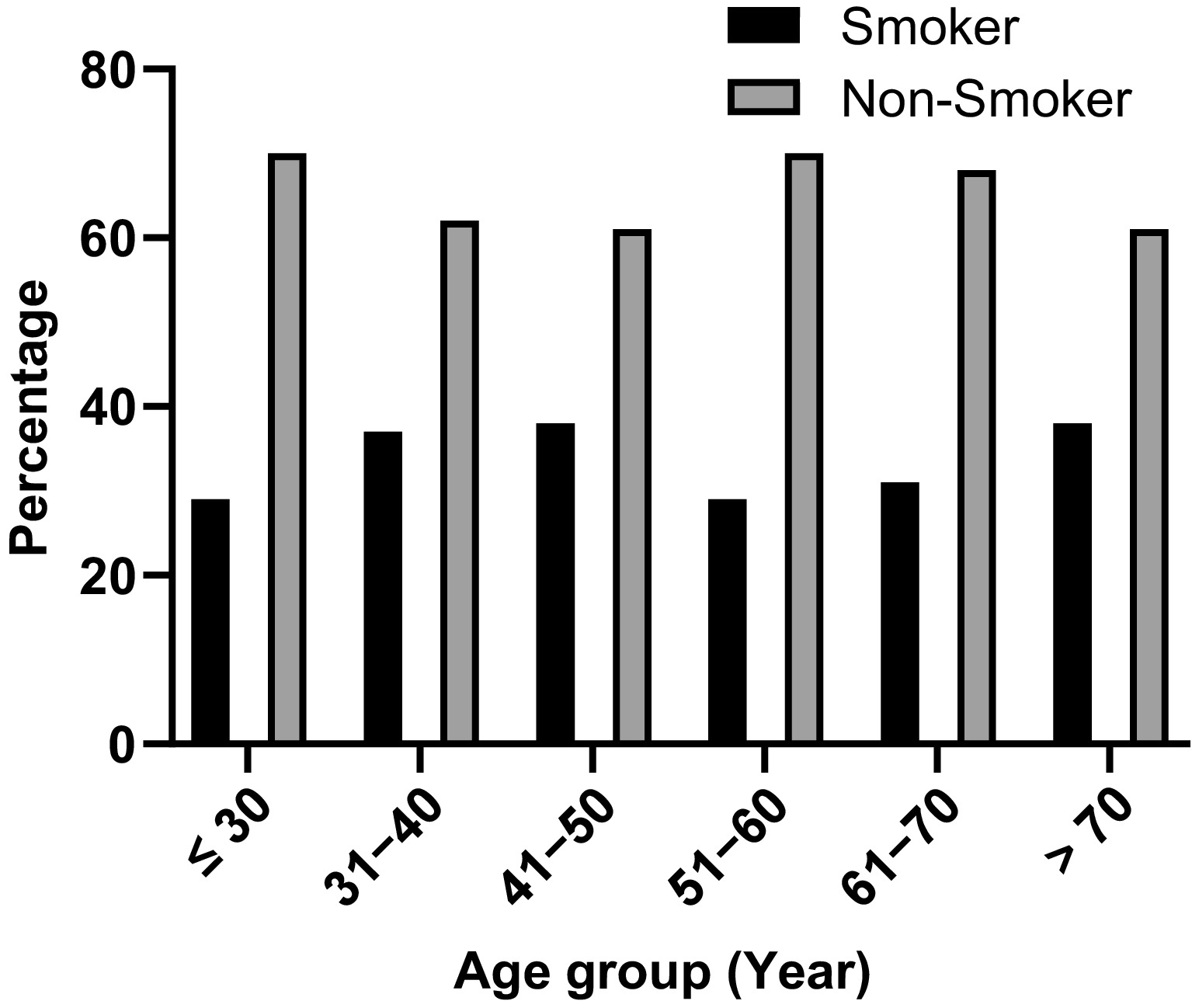
Figure 2.
Prevalence of smoking according to age group.
Table 2. Factors related to smoking.
Univariate analysis Multivariate analysis Factors Non smoker Smoker Crude OR (95% CI) p-Value Adjusted OR (95% CI) p-Value Gender Female 177 (92.2%) 15 (7.8%) 1 1 Male 180 (52.2%) 165 (47.8%) 10.817 (6.13−19.085) 0.001 8.594 (4.673−15.803) 0.001 Age (years) ≤ 30 155 (70.8%) 64 (29.2%) 1 1 31–40 92 (62.6%) 55 (37.4%) 1.448 (0.93−2.255) 0.102 0.963 (0.5−1.856) 0.911 41–50 58 (61.1%) 37 (38.9%) 1.545 (0.933−2.56) 0.091 0.704 (0.329 1.509) 0.367 51–60 33 (70.2%) 14 (29.8%) 1.027 (0.516−2.048) 0.939 0.523 (0.207−1.32) 0.17 61–70 11 (68.8%) 5 (31.3%) 1.101 (0.368−3.296) 0.864 0.847 (0.218−3.296) 0.81 > 70 8 (61.5%) 5 (38.5%) 1.514 (0.477−4.803) 0.482 1.434 (0.306−6.73) 0.648 Education status Educated 255 (69.9%) 110 (30.1%) 1 1 Uneducated 102 (59.3%) 70 (40.7%) 1.591 (1.091−2.321) 0.016 2.416 (1.457−4.006) 0.001 Marital status Single 158 (74.2%) 55 (25.8%) 1 1 Married 199 (61.4%) 125 (38.6%) 1.804 (1.234−2.638) 0.002 1.286 (0.695−2.379) 0.423 Employment status Unemployed 201 (79.8%) 51 (20.2%) 1 1 Employed 156 (54.7%) 129 (45.3%) 3.259 (2.216−4.793) 0.001 2.177 (1.315−3.606) 0.002 Physical activity No 225 (70.5%) 94 (29.5%) 1 1 Yes 132 (60.6%) 86 (39.4%) 1.559 (1.085−2.242) 0.016 1.655 (1.07−2.562) 0.024 Sleep disturbance No 229 (67.2%) 112 (32.8%) 1 1 Yes 128 (65.3%) 68 (34.7%) 1.086 (0.75−1.574) 0.662 1.112 (0.718−1.724) 0.634 Hypertension Yes 41 (80.4%) 10 (19.6%) 1 1 No 316 (65%) 170 (35%) 2.206 (1.078−4.513) 0.03 2.457 (1.044−5.779) 0.039 Hyperlipidemia No 312 (67.5%) 150 (32.5%) 1 1 Yes 45 (60%) 30 (40%) 1.387 (0.84−2.289) 0.201 1.155 (0.613−2.178) 0.656 Ischemic heart disease Yes 14 (70%) 6 (30%) 1 1 No 343 (66.3%) 174 (33.7%) 1.184 (0.447−3.134) 0.734 2.014 (0.568−7.15) 0.279 Thyroid disease No 347 (66.6%) 174 (33.4%) 1 1 Yes 10 (62.5%) 6 (37.5%) 1.197 (0.428−3.346) 0.732 1.555 (0.437−5.532) 0.496 Waist circumference High 189 (69%) 85 (31%) 1 1 Normal 168 (63.9%) 95 (36.1%) 1.257 (0.878−1.8) 0.211 0.896 (0.519−1.544) 0.691 Body mass index (BMI) Normal 118 (65.9%) 61 (34.1%) 1 1 Underweight 12 (66.7%) 6 (33.3%) 0.967 (0.346−2.703) 0.949 1.263 (0.368−4.336) 0.711 Overweight 133 (63.6%) 76 (36.4%) 1.105 (0.728−1.679) 0.639 0.728 (0.42−1.26) 0.257 Obese 94 (71.8%) 37 (28.2%) 0.761 (0.466−1.243) 0.276 0.639 (0.311−1.315) 0.224 Diabetes Non-diabetic 346 (66.7%) 173 (33.3%) 1 1 Diabetic 11 (61.1%) 7 (38.9%) 1.273 (0.485−3.341) 0.624 2.15 (0.62−7.456) 0.228 -
This population-based cross-sectional study was conducted to identify the prevalence of smoking and related factors among adults more than 18 years old in Zakho City of Kurdistan Region of Iraq. The overall prevalence of current smoking in Zakho city was 33.5%, a rate that is higher than the national average (22.44%) in 2021[4], the global prevalence of tobacco use (22.3%) in 2020[11], and the prevalence of tobacco use in Iran (14.01%) in 2021[12], but close to what was found in Turkey (30.6%) in 2022[13]. Use of tobacco in any shape or form kills and causes a wide array of diseases among millions of people every year, and thus, such a high prevalence of smoking in Zakho city is expected to contribute to a high burden of preventable complications. In developed countries, the reduction of smoking rates can be the result of increased cost, local laws, and education about the effects of smoking, thus such strategies should be employed in Zakho city to reduce smoking rates. Men were significantly more likely to be smokers (47.8%) compared to women (7.8%), and this remains true for most of the literature[4,11−13]. There are many factors contributing to higher smoking behaviors among men, including motives, gender roles, and brain sensitivity, among others[12,14]. The highest smoking rates were found among ages 41–50 years (38.9%), but this was not significantly different from other ages in the study. This is similar to other studies, some of which had a significant difference[11,13]. This could be due to the commutative nature of continuous smoking, and increased independence with middle-aged adulthood.
Uneducated people were significantly more likely than educated people to smoke (40.7% compared to 30.1%), similar to a study conducted in Japan, and this might be due to more knowledge about the effects of smoking on health, financial, and social life. Furthermore, employed people were significantly more likely to smoke (45.3%) compared to unemployed people (20.2%). Though we have not stratified our participants into specific occupational categories, other studies have found that manual workers and high-strain job employees are more likely to smoke, possibly due to the relieving nature of smoking, and the financial freedom of employees compared to unemployed participants[15,16]. Married individuals were more likely to smoke (38.6 compared to 25.8%), but this association was no longer significant in the multivariable analysis, possibly due to confounding effects. This is in contrast to the significant association of marriage to smoking in Turkey[13]. Individuals who self-identified as having physical activity were significantly more likely to smoke (39.4% compared to 29.5%), which contradicts another study that found physical exercise to be negatively associated with smoking behaviors[17]. The higher smoking prevalence among physically active individuals may reflect a subgroup of younger adults who engage in both physical activity and recreational or social smoking. Additionally, cultural norms and variations in health messaging or awareness may influence both behaviors and self-reporting. These context-specific factors, however, remain underexplored in our setting. While smoking does cause sleep-related issues[18], our study did not find an association between sleep disturbance and smoking status.
While smoking does cause acute rises in blood pressure and smokers are more likely to develop hypertension, ischemic heart disease[19], and type 2 diabetes[20], our study found that hypertensive participants were less likely to be smokers (19.6% compared to 35%). One explanation may be that individuals diagnosed with hypertension are more likely to quit smoking as part of lifestyle changes. This is supported by studies showing that a hypertension diagnosis often serves as a motivator for smoking cessation[21]. Cultural and social norms in the local context may also influence smoking behavior and self-reporting. We also did not detect an association between diabetes, nor a history of ischemic heart disease and smoking status, possibly due to similar reasons. Additionally, our study did not find a significant association between body weight or waist circumference with smoking. The literature presents inconsistent results on the relationship between smoking and body weight, and the contradictory nature of this factor requires an integrated approach focusing on these specific factors to give concise results[19].
This study has several limitations. First, as a cross-sectional study, it provides only a snapshot of the associations between variables and does not establish causality. Second, the study was conducted in a single center within a limited geographical area, which may restrict the generalizability of the findings to broader populations. Third, potential sources of bias in the study include nonresponse bias and self-reporting bias. Individuals who declined to participate may have had different smoking behaviors compared to those who took part in the study, and participants may not have provided entirely accurate information due to the self-reported nature of the data. Lastly, ex-smokers were not considered in the analysis, potentially overlooking the long-term effects of smoking cessation on the studied outcomes. These limitations should be taken into account when interpreting the results.
-
This study highlights a concerningly high prevalence of smoking (33.5%) in Zakho, surpassing national and global averages. The elevated smoking rates in men, the uneducated, and the employed indicate a necessity for focused interventions. While this study cannot establish a causal association, we still recommend some actions to tackle this growing health problem, considering the extensively documented health dangers associated with smoking.
We suggest introducing rigorous tobacco control measures such as taxation, prohibitions on public smoking, and awareness initiatives highlighting diseases linked to smoking. Educational initiatives ought to focus on high-risk populations, especially men and laborers, to tackle cultural and job-related smoking prompts. Healthcare professionals ought to incorporate smoking cessation methods into standard medical appointments. Additional long-term studies are required to investigate the effects of smoking on chronic illnesses in Zakho. A thorough, cross-sectoral strategy is crucial for lowering smoking rates and their related impact.
-
The study was conducted in accordance with the Declaration of Helsinki, and ethical approval was obtained from the Research and Ethics Committee at the College of Medicine at University of Zakho (Oct 2023/UoZ e18SS), approval date: 04/09/2023. Participants were made aware of the study, and verbal consent was gathered prior to filling out the questionnaire.
-
The authors confirm contribution to the paper as follows: study conception and design, analysis and interpretation of results, and draft manuscript preparation: Hussein NR, Abozait HJ; data collection: Naqid IA. All authors reviewed the results and approved the final version of the manuscript.
-
The data that support the findings of this study are available upon reasonable request from the corresponding authors.
-
We appreciate the valuable feedback and constructive critique from reviewers and editors.
-
The authors declare that they have no conflict of interest.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Hussein NR, Abozait HJ, Naqid IA. 2026. Prevalence and associated factors of smoking in Zakho City, Kurdistan Region, Iraq: a population-based study. Journal of Smoking Cessation 21: e003 doi: 10.48130/jsc-0026-0002 

Prevalence and associated factors of smoking in Zakho City, Kurdistan Region, Iraq: a population-based study
- Received: 09 March 2025
- Revised: 03 February 2026
- Accepted: 05 March 2026
- Published online: 30 March 2026
Abstract: Smoking remains a significant public health issue globally, contributing to a wide range of preventable diseases and premature mortality. This study aims to assess the prevalence of smoking and its associated factors in Zakho, Kurdistan, Iraq. A cross-sectional study was conducted in January 2024, involving 537 adults aged 18 and older. Participants were randomly selected using a multistage sampling process, and data was collected using a structured questionnaire including clinical, behavioral, and sociodemographic information. Logistic regression was performed in IBM SPSS to identify factors associated with smoking. The mean age of participants was 35.73 ± 13.95 standard deviation. The prevalence of smoking in Zakho was found to be 180 (33.5%), with significantly higher rates among men, 165 (47.8%) compared to women, 15 (7.8%). Factors such as gender, education, employment status, physical activity, and hypertension were significantly associated with smoking. The smoking prevalence in Zakho surpasses both the national and global averages. It is more common among men, the uneducated, and the employed. Targeted tobacco control measures such as public smoking bans, higher taxes, and education are needed. Healthcare professionals should promote cessation strategies to reduce the burden of smoking. Further longitudinal studies must explore long-term health effects.
-
Key words:
- Smoking /
- Prevalence /
- Epidemiology /
- Associated factors /
- Zakho City /
- Kurdistan Region /
- Iraq