








-
Tobacco use has a long history in East Asian societies since around the 17th century. Historically, tobacco's medicinal use was explored by traditional medicinal regimes; tobacco's cultural significance spread well before the modern biochemical regime revealed its profound damage to health[1]. In South Korea, smoking caused 1.7- and 1.6-times higher hazard of death among men and women[2]. In China, the hazard of death among smokers is 1.37 times higher compared to non-smokers[3]. The recognition of tobacco harm to public health and the administrative efforts to control tobacco use are an important element in the history of modernization in East Asian countries.
Given the burden of tobacco-related disease, countries in East Asia have gradually adopted the tobacco control conventions issued by the World Health Organization and different countries on the consumption of tobacco products. However, at the grassroots level, smoking cessation often faces challenging reactions rooted in the social and cultural fabrics as tobacco use had a profound cultural significance in social interaction in East Asian societies[4]. Tobacco use rates remained high in East Asian countries due to a mix of cultural acceptance and limited regulation. Conventional cessation interventions with a focus on clinical significance and health information often fall short of effectiveness because the rational benefit-cost analysis, which constitutes the core principles of health promotion strategies, may give way to the cultural considerations of why people use tobacco in the first place[5].
China and South Korea serve as two representative East Asian countries for comparison. Compared to the global average, China has a high male smoking prevalence at about 45%; South Korea's male smoking prevalence at over 30% is significantly higher than the OECD countries' average at 20%; hidden female smokers may exceed 20% of all Korean females[6−8]. However, in both countries, female smoking rates were significantly lower than their reference groups, as patriarchal gender ideology may have a significant influence[9].
Cessation in China and South Korea
-
Cessation rates in China were reported to be low. A 1996 national survey[10] found only 9.5% of ever-smokers had managed to quit, and over 70% of current smokers had no intention of quitting. Although cessation has improved in recent surveys, only about 19% of Chinese smokers reported a quit attempt in the past year, and even fewer followed through with concrete action[11]. However, the situation seems to have improved as practitioners and scientists based in China design increasingly effective cessation intervention techniques[12].
South Korea has seen a marked decline in smoking prevalence due to strong tobacco control and cessation initiatives. In 1998, 66% of Korean men smoked, but by 2022, this prevalence had dropped to 30%[7]. Compared to Chinese smokers, 50% of Korean smokers had made a quit attempt in the past 12 months[11]. Korean smokers receive more encouragement to quit from healthcare providers: 74% of smokers in Korea reported receiving advice to quit from a physician during visits, compared to 56% in China[11].
Cessation-oriented behaviors have seen unequal progress among different demographic groups[13]. Female cessation attempts and success rates were higher in South Korea and China. About 26% of male smokers stated they have attempted to quit in the past year, but 31% of female smokers stated the intention[14]. Cessation remains low and clinical assistance is infrequently utilized among Chinese male smokers, and some scholars speculate that using tobacco for socialization purposes became a main reason for the self-exemption from attempting cessation[15,16].
Sociocultural factors in smoking cessation
-
Understanding what factors led smokers to attempt quitting is crucial for designing effective tobacco control and improving public health. Extant research has thoroughly explored the proximate psychological processes and background demographic factors associated with cessation but relatively overlooked the importance of cultural and social attitudinal factors embedded in the normative context that enabled and encouraged certain people to smoke in the first place.
Individual substance users embody a constellation of motifs and beliefs that make them more susceptible to the influence of risk behaviors, or alternatively, more compliant to follow the advice of medical authorities, such as smoking cessation advice. These motifs and beliefs were not innately grown but habitually formed during the socialization process, relating to a network of background social characteristics such as family integrity, peer deviance, and class subculture[17]. Compared to the clinically-oriented paradigm on addictive substances, which narrows in on the micro-level psychological processes and proximate biomedical factors leading to smoking, the sociology of drug use critically evaluates how the societal structure and organization put certain populations at a greater risk of substance use[18−20].
Among various dimensions of background societal characteristics, some conceptually belong to the more distant causal upstream (e.g., class, occupation, nativity), while others are more proximately linked to how an individual is socialized into habitual thinking and behaviour[21]. Sociocultural factors such as gender ideology, authoritarian-liberal beliefs, and social trust are intermediate proximate causal antecedents to behaviors. These factors may directly influence several important decision-making and trigger the events involved in smoking cessation: whether continuing smoking is appropriate in one's gender script; whether official health information should be accepted without reservation; whether medical professionals, families, and other members in society are trust-worthy.
Social trust represents an important contextual and relational factor influencing health behaviors in East Asia. Social trust is conceptualized as a component of social capital that facilitates cooperative norms that encourage compliance with collective rules. Higher social trust has been associated with greater engagement in preventive behaviors, adherence to medical advice, and adoption of healthier lifestyles[22]. However, specialty literature from East Asia has pointed out that, due to the social desirability and peer pressure of smoking, social capital and trust may encourage the adoption and maintenance of tobacco smoking[4].
Authoritarian beliefs refer to the volitional acceptance and agreement with traditional legitimate power structures, including obeyance to traditional roles and collective activities[23]. Authoritarian beliefs in the East Asian cultural background may be positively associated with complacency in smoking and may weaken cessation motivation and attempt[15]. Obeyance of traditional authority and order makes people less likely to challenge the predominant smoking culture in workplace, particularly when smokers are more senior in social status. The meticulous organization of implicitly recognized rites and etiquette in daily interactions in Asian culture, highly competitive and ritualized work routines, and the shame/honor-based codes of conduct, led some people, particularly men, to use tobacco in gift-exchange and as a social lubricant[4]. However, it is also possible that authoritarian beliefs are positively associated with compliance with medical authority, contradicting the predominant smoking-friendly peer network and the subcultures associated with it. Respect and submission to family authorities may foster taking advice from family members, whose cessation pressure became more effective among smokers[24].
In addition, traditional gender ideology, which regulates a complementary role assignment and distinct privilege between males and females, may also negatively affect smoking cessation[13]. Under traditional gender ideology, males are encouraged to engage in more at-risk behaviors to exhibit the perceived masculinity associated with carelessness and audacity, while females are advised to acquiesce to the male-dominated smoking culture and even comply with the behavior when asked to[25]. Another study found that cities with a higher male-female sex ratio (a proxy used for traditional gender ideology) tend to have higher male smoking prevalence and lower female prevalence[26]. More modern social development and less reliance on traditional societal arrangement is shown to be associated with lower risks of smoking and drinking in China.
Scholars have found that most people continued smoking while acknowledging the health consequences, citing its necessity in social functioning as an exempting belief. In China, cigarette gifting and shared smoking are ingrained in business and social interactions, creating cultural pressure to continue smoking or at least making it hard to refuse cigarettes[4]. For example, a man who quit might be offered a cigarette in a business meeting and feel obliged to accept, risking relapse. This incident exemplified the normalization of tobacco use in culturally appropriate settings and posed an obstacle to tobacco control in China.
South Korea also has a historically entrenched male smoking culture due to a similar patriarchal Confucianism culture[27,28], but also as a result of the social bonding created by the military culture. South Korea remains one of the most gender-unequal countries within the OECD, despite rapid economic development and widespread educational attainment among younger generations[29]. Persistent disparities in earnings, labor force participation, and political representation reflect the ongoing strength of traditional gender systems[30]. These structural inequalities continue to shape social expectations surrounding responsibility, conformity, and health behaviors[27,28]. Superiority based on age and organizational hierarchy is a prominent feature in Korean culture and shapes daily interactions. Junior members, particularly those within the same organizational context (e.g., corporate, academic, or military), are routinely expected to defer to their seniors through ritualized displays of submission. Tobacco use and drinking gatherings that involve individuals of different hierarchical ranks are common, and subordinates often feel compelled to participate rather than refuse these activities. Consequently, it is plausible that traditional gender role perceptions still meaningfully influence health-related behaviors such as smoking cessation among Korean young adults[31]. The enduring influence of gendered social expectations may make gender ideology a particularly important factor in understanding smoking cessation patterns in Korea.
Study rationale
-
To close the gap that few have studied on how the sociocultural factors relevant in the East Asian context are related to smoking cessation. This study conducted survival analysis on two samples of young adults from China and South Korea, respectively. We tested whether gender ideology, authoritarian belief, and social trust are associated with lower odds of cessation by comparing current smokers with ex-smokers, and by comparing two national samples.
The focal independent variables for survival hazards are authoritarian belief (negatively associated with cessation), traditional gender attitudes (negatively associated with cessation), and social trust (positively associated with cessation). The dependent variable was the time until smoking cessation, calculated as odds using survival analysis. This study conducted a Cox survival model to test the associations between cessation and the independent variables.
-
A cross-sectional survey was conducted at the same time in South Korea and four Chinese regions during 2022–2023 using the same questionnaire. The target population was young adults aged 18 to 25 years, with a focus on their substance use behaviors and beliefs. This age range, as a part of emerging adulthood, is a critical period for both habit formation and cessation behaviors related to tobacco use.
Sampling in the Chinese survey were primarily drawn using multi-stage clustered sampling at school-level. The survey selected four ideal-typical cultural zones: the Yangtze Delta, the Pearl Delta, northern China, and the Southwest. In comparison to South Korea, China exhibits significant heterogeneity and a vast population size, which complicates its classification as a single sampling unit. Consequently, ensuring population representativeness presents a substantial challenge, impeding our ability to accurately identify and analyze distinct demographic patterns across different groups[32]. Thus, this survey focused on cultural representativeness, a strategy often deployed in comparative research to highlight the unique pattern represented in each ideal-typical cultural group. These four regions, while all situated within China proper, possess their own languages and cultural practices that are often mutually unintelligible. Their diversity and distinctions make a perfect case for using them as the ideal types of Chinese culture. At least one municipality in each region exclusively sampled rural districts. The survey imposed a quota to ensure that each region sampled all four types of schools: high school, vocational high school, college, and vocational college. Within each school, at least two classes of similar sizes were selected by local teacher coordinators. The survey returned with 2,800 respondents, of which 2,554 were valid after data cleaning.
Data from the Korean survey were collected via an anonymous online questionnaire facilitated by a professional survey research firm. Respondents were recruited through email invitations sent to a nationwide survey panel (n = 1,018), with 700 valid responses for this study. All 17 provinces and special cities were covered, with over 50% from the Seoul-Incheon metropolitan area. The invitations provided general information about the survey, its purpose, and included a consent statement. Eligibility criteria included: (1) being aged between 18 and 25 years; (2) residing in South Korea; and (3) being Korean speakers. A proportional and quota sampling method based on age, gender, and geographic region was used to ensure a representative sample. The different sample sizes for China and South Korea were considered based on the population sizes of the two countries. China has a population of approximately 1.4 billion, whereas South Korea's population is around 51 million. This proportional adjustment ensures our study captures a representative sample that accurately reflects the demographics and diversity of each country.
For the survival analysis used in this study, only ever-smokers and current smokers were retained for the model (n = 418; 209 Chinese, 209 Korean). The Schoenfeld equation for sample size and power[33] is
$ E=\dfrac{{\left({Z}_{\frac{a}{2}}+{Z}_{1-\beta }\right)}^{2}}{logH{R}^{2}*p(1-p)} $ Measurement
-
Survival hazard event: The primary event of interest in this study was cessation of tobacco use, inclusive of vaping electronic cigarettes and smoking combustible cigarettes. An event was considered to have occurred if a participant reported a combined status of 'not currently smoking/vaping' and 'smoked/vaped before' in the questionnaire. Participants who were smoking or vaping during the study period were right-censored. Censoring occurred at the current age of the tobacco users.
Time Origin and Survival Time: The time origin (t = 0) was defined as the respondent-reported age of first use. Survival time was calculated as the duration from this age to the age of the cessation event or censoring.
Authoritarian beliefs were measured on the simplified authoritarian-traditionalism scale. The idea conveyed by this scale was inspired by a previous study on obedience to order and authority[23]. Psychometric studies have attempted to adopt the authoritarianism scale in Asian cultures, with tests showing its internal reliability ranging from 0.67 to 0.77[34,35]. This study focused on individual's agreement on submitting to authorities and obeying the traditional order. Respondents rated their agreement on three Likert-type scales adopted from the Chinese General Social Survey: 'children should stay silent when adults are talking', 'the harmony of the family is more important than an individual's success', 'it is everyone's duty to observe and celebrate traditional festivals'. The authoritarian beliefs scale had a Cronbach's alpha of 0.66, a moderate internal reliability given the small number of items.
Gender ideology on a spectrum from egalitarianism to traditionalism were measured using the 5-point Likert-scale that captures how respondents viewed the roles and rights of each gender in society[36]. Respondents rated their level of agreement to three questions: 'men should prioritize their career, women should prioritize family', 'women are less competent than men in their jobs', 'sons should inherit money more than daughters'. The gender ideology scale showed a high Cronbach's alpha of 0.86.
Social trust is measured by a common question[37] rated on a 5-point scale: 'in general, people in this society are trying to take advantage of me'. Covariates to control for potential confounding effects on both the survival hazard and key independent variables include gender, current age, income (standardized and log-transformed), and the highest parental educational level.
Statistical model
-
To examine the factors associated with smoking cessation, we employed a Cox proportional hazards model using age as the time scale. The outcome of interest was the duration of smoking prior to cessation, measured from the age of smoking initiation to either the age at which the respondent reported quitting (for ex-smokers) or their current age (for current smokers). Respondents who continued smoking at the time of survey administration were treated as right-censored observations. Although the data are cross-sectional, retrospective reports of age at initiation and cessation allow for reconstructing individual event histories and are widely used in population-level studies[21,38].
We constructed a survival dataset by calculating each individual's observed time-to-event. Specifically, for individuals who quit smoking, the event time was defined as their reported age at smoking cessation. For current smokers, the censoring time was defined as their current age. The binary event indicator was coded as 1 for those who had quit smoking and 0 for those who had not. We then estimated the Cox model specified as:
$ h\left(t\right)={h}_{0}{\left(t\right)}^{\boldsymbol{\beta }\boldsymbol{X}} $ where, h(t) is the hazard of cessation at time t, and h0(t) is the baseline hazard function, X is a vector of covariates. To examine how sociocultural risk factors differ between Chinese and Korean smokers, we created interaction terms between nationality and the three sociocultural variables and tested their effects on survival hazards (cessation).
Survival analysis was first conducted using the Kaplan–Meier method to display the survival function[39]. For the effect of covariates, we conducted Cox proportional hazards regression models. The global and local tests of Schoenfeld residuals (rho) were conducted to verify the proportional hazards assumption. Although retrospective recall allows reconstruction of event history, this approach does not establish temporality and should be interpreted as associative rather than causal. As a robustness check, we estimated logistic regression models comparing current and former users of combustible and electronic tobacco. All analyses were conducted in Stata 18.
-
Table 1 presents the descriptive statistics of our sample. The sample included 3,254 respondents, of whom 21.5% were from South Korea, and 48.3% were male, and the rest were Chinese samples and females. The mean age was 19.36 years (SD = 2.79). Regarding tobacco use, 7.2% were current combustible cigarette smokers, and 6.1% had smoked before; 4.2% were currently using electronic cigarettes, and 7.3% claimed they had vaped before. Regarding the sociocultural variables, the respondents expressed moderate levels of authoritarian belief (3.38, SD = 0.85) and generalized social trust (3.11, SD = 1.08), but they scored low on gender traditionalism (1.79, SD = 0.93).
Table 1. Descriptive statistics of the full sample.
China South Korea t-test/Chi2 n (%);
mean (SD)n (%);
mean (SD)n 2,554 700 Electronic tobacco 258.9, p < 0.001 −Never used e-cigarettes 2,198 (93.4%) 505 (72.1%) −Previously used e-cigarettes 115 (4.9%) 108 (15.4%) −Currently using e-cigarettes 40 (1.7%) 87 (12.4%) Combustible tobacco 634.5, p < 0.001 −Never smoked 2,288 (90.7%) 100 (72.4%) −Previously smoked 97 (3.8%) 93 (14.3%) −Currently smoking 138 (5.5%) 93 (13.3%) Age 18.37 (2.06) 22.98 (1.96) −54.5, p < 0.001 Income (log standardized) 0.04 (1.01) −0.00 (1.0) 0.94, p = 0.350 Male 1,205 (47.2%) 368 (52.6%) 6.18, p < 0.05 Parental education 601.3, p < 0.001 −Elementary school 160 (6.3%) 4 (0.6%) −Junior high 836 (33.0%) 4 (0.6%) −Senior high 827 (32.7%) 202 (28.9%) −Vocational school 279 (11.0%) 94 (13.4%) −University and above 428 (16.9%) 396 (56.6%) Authoritative belief 3.47 (0.86) 3.02 (0.71) 14.16, p < 0.001 Gender ideology 1.75 (0.91) 1.93 (0.97) −4.41, p < 0.001 Social trust (reverse) 2.92 (1.05) 3.79 (0.91) −21.64, p < 0.001 Table 2 shows the survival analysis using Kaplan–Meier estimation. Among the total sample (n = 3,254), 418 participants were included in the survival analysis. The probabilities revealed a steady decline in the number of tobacco users in both national subsamples. Among Chinese respondents, the probability of remaining a tobacco user fell from 0.98 at time 1 to 0.59 by time 12. For South Koreans, the probability of remaining a tobacco user declined from 0.95 at time 1 to 0.64 at time 12.
Table 2. Kaplan–Meier survival estimates.
Survival time At risk Event (cessation) Net lost Survivor function SE China 1 209 4 25 0.98 0.01 2 180 12 30 0.91 0.02 3 138 12 23 0.83 0.03 4 103 3 33 0.81 0.03 5 67 4 16 0.76 0.04 6 47 2 10 0.73 0.04 7 35 2 9 0.68 0.05 8 24 2 4 0.63 0.06 9 18 0 1 0.63 0.06 10 17 1 5 0.59 0.07 11 11 0 1 0.59 0.07 12 10 0 1 0.59 0.07 South Korea 1 209 10 29 0.95 0.01 2 170 9 24 0.90 0.02 3 137 7 23 0.85 0.03 4 107 6 27 0.80 0.03 5 74 7 18 0.73 0.04 6 49 2 23 0.70 0.04 7 24 2 7 0.64 0.06 8 15 0 4 0.64 0.06 9 11 0 8 0.64 0.06 10 3 0 1 0.64 0.06 11 2 0 1 0.64 0.06 12 1 0 1 0.64 0.06 Conversely, Fig. 1 illustrates the cumulative hazard of tobacco cessation by gender and country. This figure shows a complex pattern of gender and contextual variations in cessation probabilities. The Chinese females (yellow dashed line) showed the fastest and steepest increase in cessation, reaching their maximum cessation hazard at time 4 ahead of other demographic groups. Chinese males (yellow solid line) took a longer time to quit, reaching their maximum hazard of cessation almost 4 periods later than Chinese females. Among Koreans, males increased cessation rate faster than Chinese males but slower than Chinese females. However, Korean females are the least likely group to quit using tobacco: their maximum hazard of cessation is only 0.20 and stopped at time 5. Cumulative hazard estimates gave us a general idea of the demographic differences in cessation rate, but the results cannot account for the effects of covariates and group sizes. So, we turned to the Cox proportional hazard models next.
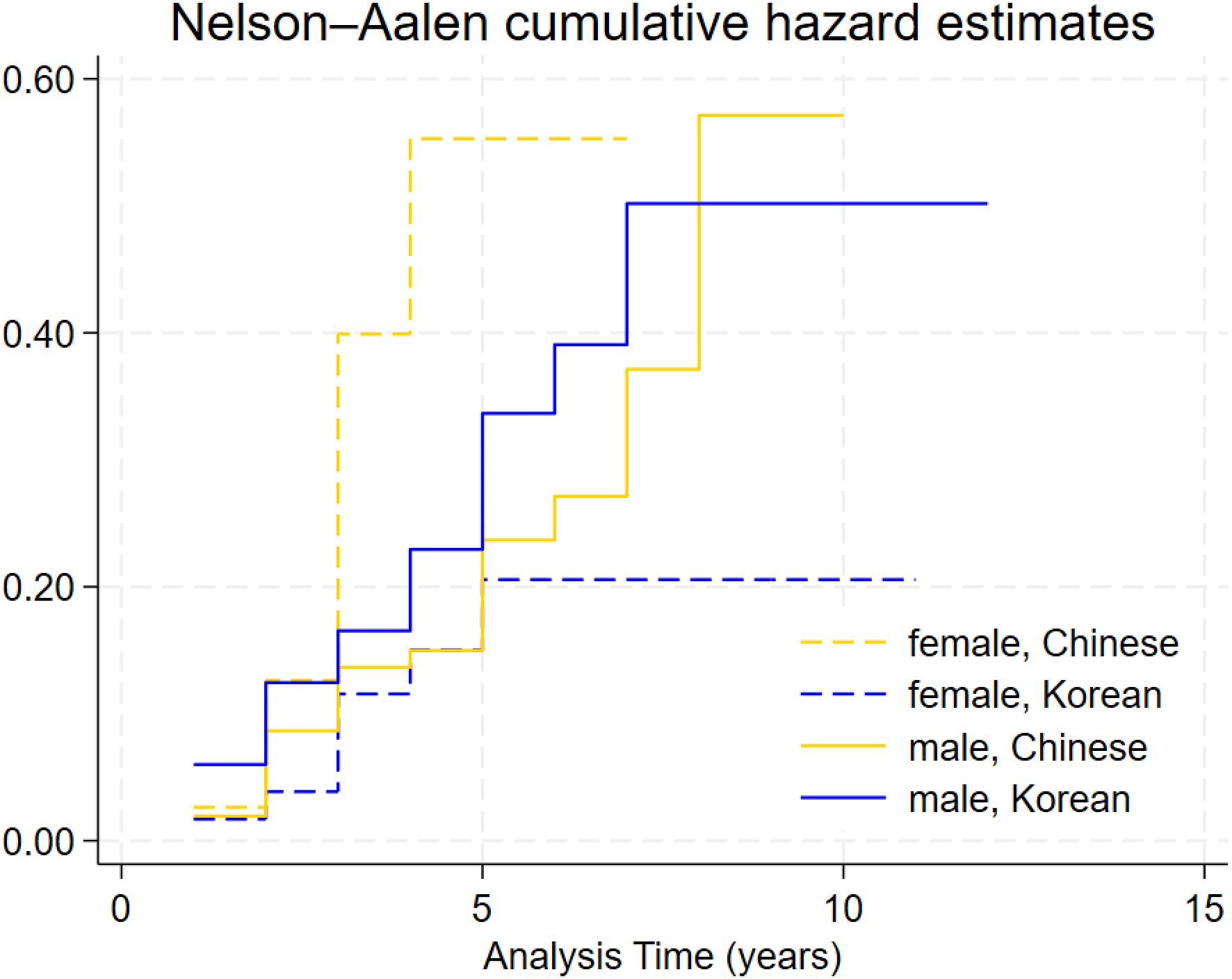
Figure 1.
Cumulative hazards of cessation by country and gender.
Finally, Table 3 presents three Cox regression models predicting the hazard of tobacco cessation. Model 1 controlled for the basic demographic markers: country, gender, and age. South Korean was associated with a significantly higher hazard of cessation (HR = 3.40, SE = 1.29, p < 0.001), while gender was not a significant predictor, possibly due to the small number of female smokers. The global and local tests of Schoenfeld residuals (rho) indicated that the proportional hazards assumption was not violated. Model 2 introduced sociocultural variables and covariates. The South Korean effect remained robust (HR = 3.63, SE = 1.53, p < 0.01). Age continued to show a negative effect on cessation (HR = 0.81, SE = 0.05, p < 0.001). To our disappointment, we found in Model 2 that none of the three sociocultural variables were significantly associated with cessation hazards. Yet, we noticed that the p-value in the global test of proportional hazards assumption had declined considerably from 0.46 to 0.25 upon inclusion of these variables. This finding suggests that sociocultural factors may influence cessation differently across national contexts, an idea further explored in Model 3 through interaction terms.
Table 3. Cox proportional hazard models.
M1 M2 M3 Hazard ratio SE p (rho) Hazard ratio SE p (rho) Hazard ratio SE p (rho) Korean 3.40 1.29*** 0.12 3.63 1.53** 0.19 2.33 3.13 0.79 Male 0.80 0.21 0.80 0.87 0.24 0.72 0.79 0.22 0.98 Age 0.78 0.05*** 0.13 0.81 0.05*** 0.03 0.81 0.05** 0.05 Income 0.91 0.09 0.21 0.94 0.09 0.31 Parental education 0.85 0.09 0.65 0.85 0.09 0.80 Gender ideology 0.95 0.12 0.54 0.69 0.14 0.43 Authoritative 0.92 0.13 0.09 1.16 0.21 0.05 Social trust 0.97 0.11 0.31 0.88 0.13 0.18 Gender ideo × Korean 2.08 0.54** 0.37 Authoritative × Korean 0.46 0.14* 0.30 Trust × Korean 1.42 0.32 0.35 n 418 412 412 n. event 85 85 85 Time at risk 1,710 1,646 1,646 Global proportional hazard test 0.46 0.25 0.34 * p < 0.05, ** p < 0.01, *** p < 0.001. Therefore, we added interaction terms between sample country and sociocultural variables in Model 3. The interaction between gender traditionalism and being Korean is significant at the 0.01 level and positively associated with cessation hazard (HR = 2.08). This means that gender traditionalism has a stronger effect on cessation hazards among Koreans, compared to the Chinese. Figure 2 visualizes the multiplicative contrasts: compared to Koreans holding low level of gender traditionalism (blue dashed line), cessation hazards at each time period were higher among Koreans holding high level of gender traditionalism (blue solid); however the trend is reversed among Chinese, where high level of gender traditionalism (yellow solid) was associated with lower cessation hazards compared to low level of gender traditionalism (yellow dashed).
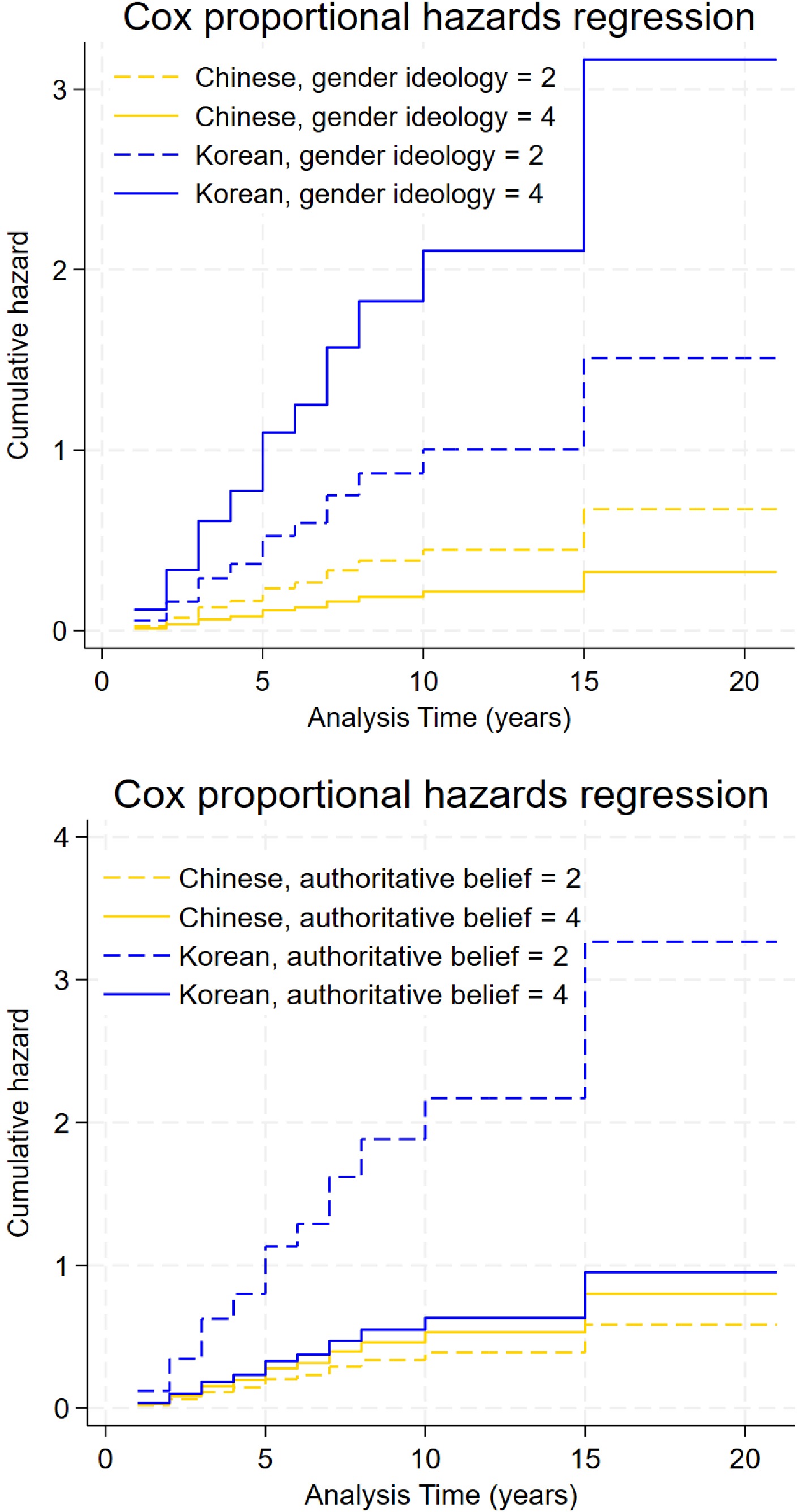
Figure 2.
Cumulative hazard curves by country and sociocultural factors.
The interaction between authoritarian beliefs and being Korean is significant at the 0.05 level but is negatively associated with cessation hazard (HR = 0.46). The second graph in Fig. 2 shows that Koreans holding a low level of authoritarianism (blue dashed) is associated with higher hazards of cessation and shows the most rapid increase in cessation rate. In contrast, Chinese holding low level of authoritarianism (yellow dashed) showed the lowest rate of cessation. Taken together, the sub-group with the highest likelihood of cessation comprised Koreans with high gender traditionalism and low authoritarianism. The sub-group least likely to quit was Chinese with a high level of gender traditionalism.
As a robustness check, we estimated logistic regression models in Supplementary Table S1. Although most associations did not reach statistical significance in these models, the direction of effects remained largely consistent with those observed in the survival analyses. This pattern is expected, as logistic regressions collapse cessation into a current smoking status and do not account for smoking duration, timing of cessation, or right-censoring.
-
Smoking cessation was predominantly discussed and studied in clinical settings, with important sociological and cultural constructs often neglected in terms of their potential in promoting cessation likelihood. The current study examined how sociocultural factors—gender ideology, authoritarian belief, and social trust—shape tobacco cessation among young adults in China and South Korea. Using survival analysis, we focused on cessation timing and hazards of using tobacco products. While the main effects of the sociocultural factors were not significant, their interactions with nationality showcase the complex patterns of how sociocultural factors may affect cessation.
The basic pattern confirmed previous findings that Korean young adults were more likely to quit smoking compared to their Chinese counterparts. This may be due to South Korea's stronger tobacco control policies and better access to cessation services. But our findings also show that the advantage in cessation is not consistent across all groups. Especially, Korean females had the lowest hazard of cessation. There are two potential reasons. Female smokers in Korea still face stronger barriers to quitting, possibly due to hidden smoking behavior and the social stigma around women smoking[6]. Another possibility is that the lower prevalence of female tobacco use had set high the addictiveness and adherence to the behavior, which is related to their lower cessation intention and effort.
The first most important finding is about gender ideology. Among Koreans, holding traditional gender ideology was associated with a higher likelihood of cessation. This might seem surprising, but previous research has documented the trend that some traditional gender and familial values can be utilized to convince cessation efforts[13,40]. Another explanation is that the lower cessation probability and gender traditionalism were both concentrated among the female Korean sample. It is possible that traditional gender ideology may operate through different mechanisms across genders. Among males, traditional gender ideology emphasizing responsibility, self-discipline, and the provider role may have strengthened self-efficacy and the motivation to quit smoking[41]. According to a study of Korean female smokers, the primary reason for enrolling in a smoking cessation outreach program was being asked to quit by family and friends (46.8%)[42]. Traditional gender ideology emphasizing family welfare and caregiving roles could have similarly fostered among Korean females a greater motivation to protect family health by quitting smoking. Yet, stigma and structural barriers from conventional cessation programs, which were deeply rooted in traditional gender ideology, still pose challenges for female Koreans to quit[27].
On the other hand, a reversed trend as opposed to South Korea was observed in China, where traditional gender ideology was negatively associated with cessation likelihood. Existing studies showed that smoking remains a powerful traditional symbolic gesture in China, used for workplace networking and ritualized gift-giving[25,43]. This phenomenon was particularly true among males, but also evident among females in regard to their lack of apathy to secondary smoking[44]. Here, traditional gender beliefs may still sanction smoking as a marker of masculinity and a medium of male socialization, thereby discouraging cessation among those who most strongly endorse gender traditionalism.
The effects of authoritarian beliefs were also significantly contrasted between the Korean and Chinese samples. Low authoritarianism was associated with a much higher likelihood of cessation among Koreans, but it was associated with a slightly lower likelihood of cessation among Chinese. This finding adds nuances to the claim that deviant behaviors such as smoking may not necessarily be rebellious against mainstream society[45,46]. This finding contradicts the previous literature on smoking in China, which argued that cigarette smoking often functions as a performance of authority and maturity[4]. The fact that our study population was young adults suggests that younger Chinese cohorts may no longer subscribe to the authoritarian elements in the smoking subculture. By contrast, in South Korea, where tobacco control has become part of the mainstream authority structure, and smoking is increasingly stigmatized, low authoritarianism becomes conducive to higher cessation rates[47]. This divergence also suggests the different developmental stages of tobacco control: while China is in an earlier phase of shifting authority away from pro-smoking norms, South Korea might have already institutionalized tobacco control as part of mainstream authority.
Our findings suggest that sociocultural factors do not operate uniformly across countries. This highlights the limitations of a one-size-fits-all approach to tobacco control, which often overlooks the sociocultural context in which behaviors are embedded. Given the cross-national and gender differences in how sociocultural factors shape cessation, tobacco control policies should be contextualized and differentiated. policies should strengthen gender-sensitive cessation services, including intensive early counseling, physical activity promotion, and family-centered interventions[13,40]. For example, in China, policies should aim to undermine the symbolic value of tobacco associated with male authority, restricting the circulation of cigarettes as gifts. Policies may also promote educational messages to reframe cessation as part of men's responsibility for health, productivity, and leadership. Regarding the implications of authoritarian beliefs on cessation, interventions could be made to frame quitting as an act of autonomy and empowerment. In South Korea, where tobacco control has already been institutionalized within broader public health systems, the next step lies in addressing hidden smoking among women and integrating cessation into holistic mental health and stress management programs for young adults. In both countries, tobacco control strategies that cultivate critical reflection, promote autonomy, and align cessation with culturally valued social roles may offer a more sustainable pathway toward reducing tobacco use[15].
-
First, survival time was based on self-reported age of smoking and quitting, which may involve recall bias. Especially, due to the strong social stigma associated with female smoking in Korea[27], some female participants may have underreported their smoking behavior or overstated their cessation success, leading to potential sample bias or overestimation of cessation rates among women. This pattern of underreporting among Korean female smokers has been consistently documented in previous studies[48]. Second, our items for measuring gender ideology, authoritarianism, and social trust were relatively concise and may not capture the full range of attitudes. Finally, another limitation is that the Chinese sample was collected primarily through classroom-based surveys supplemented with online data, while the Korean sample was collected fully online; thus, differences in survey mode may have introduced biases.
-
Among ever-users of tobacco products (including electronic cigarettes and combustible cigarettes), there is a remarkable national difference in the sociocultural factors associated with cessation hazards. Overall, South Koreans were more likely to quit than the Chinese. There are greater challenges on the long journey towards a smoke-free society in China.
In South Korea, gender traditionalism was associated with higher cessation hazards, but in China, authoritarianism was associated with higher cessation hazards. The role of gender traditionalism in South Korea may be utilized to encourage cessation attempts based on family units. In both countries, cessation programs should address cigarette gifting and shared smoking on social occasions, and reframe masculinity toward responsibility and health. Culturally sensitive approaches that target social norms, gender roles, and authority structures are as important as clinical treatment.
-
The study was conducted in accordance with the Declaration of Helsinki, and all procedures were approved by the ethical review committee of Sun Yat-sen University School of Sociology and Anthropology (SCA21002) on June 25, 2021 and Seoul National University Institutional Review Board (IRB 2202/004-017) on February 25, 2022.
-
The authors confirm their contributions to the paper as follows: conceptualized the study: Yang X, Lee M; drafted the manuscript, and obtained the data: Yang X; obtained the data: Lee M; cleaned and prepared the dataset: Yang F; conducted the analysis: Ren J; assisted the writing of the first draft and revision: Fan W. All authors reviewed the results and approved the final version of the manuscript.
-
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy concerns and ethical restrictions related to human participant data but are available from the corresponding author upon reasonable request.
-
This study has been supported by the US-China Medical Board (#21-436) and the Ministry of Education of China (25YJA840022).
-
The authors declare that they have no conflict of interest.
-
accompanies this paper online at: https://doi.org/10.48130/jsc-0026-0005.
- Supplementary Table S1 Logistic regression on current users vs. ex-users.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Yang X, Yang F, Fan W, Ren J, Lee M. 2026. The sociocultural factors in tobacco cessation in East Asia: a comparative survival analysis of young adults in China and South Korea. Journal of Smoking Cessation 21: e006 doi: 10.48130/jsc-0026-0005 

The sociocultural factors in tobacco cessation in East Asia: a comparative survival analysis of young adults in China and South Korea
- Received: 13 May 2025
- Revised: 18 December 2025
- Accepted: 30 April 2026
- Published online: 23 June 2026
Abstract: This study investigates how three sociocultural factors--gender ideology, authoritarian beliefs, and social trust--are associated with tobacco use cessation among young adults in China and South Korea. We conducted a cross-sectional survey of young adults (ages 18–25) in China and South Korea. Among the 418 ever-users of any tobacco product, retrospective reports of tobacco use were recorded for the initial age of use, the age of last use, and the current use status. Using Cox proportional hazards models, we examined how sociocultural factors are associated with cessation hazards. Kaplan–Meier curves and interactions were used to contrast national differences. A total of 85 ever-users (20%) had quit tobacco use. Koreans were 3.6 times (p < 0.01) more likely to have quit compared to the Chinese. There are significant national differences: gender traditionalism was positively related to cessation odds among Koreans but negatively related among Chinese (HR = 2.08, p < 0.01), while authoritarian beliefs were related to lower cessation among Koreans compared to Chinese (HR = 0.46, p < 0.05). Due to the disparate sociocultural effects, tobacco control in East Asia should consider the contextual sensitivity when tailoring cessation programs.
-
Key words:
- Gender /
- Tobacco /
- Survival analysis /
- International comparison