










-
Psychiatric disorders have become highly important health issues for society and people worldwide[1,2]. According to the Global Burden of Disease Study, psychiatric disorders are reported to be strongly associated with premature mortality and serve as the consistent leading causes of lifelong disability[1,3,4]. Glaucoma, as a typical neurodegenerative disease, is a leading cause of irreversible blindness, with a sharply increasing global prevalence, which is projected to affect over 110 million people in 2040[5,6]. Primary open-angle glaucoma (POAG), which is largely influenced by genetic factors, is known to be the most common subtype of glaucoma and threatens the visual health of over 44 million individuals worldwide[7−9]. Both of the diseases impede the independence of individuals, which are gradually considered serious public health problems.
Emerging studies have demonstrated the comorbidity of psychiatric disorders and glaucoma. As a chronic and progressive disease characterized by vision impairment, glaucoma, especially POAG, is reported to impose negative emotional impacts on patients and even force them into psychological disturbances[10−13]. Patients with POAG are found to have different personality profiles and temperaments compared with healthy people[13]. Plenty of studies have reported that patients with glaucoma are prone to suffer from various types of psychiatric disorders. A high prevalence of glaucoma is found in severely mentally ill patients, especially those with schizophrenia[14,15]. The results are also supported by another population-based study, which shows that glaucoma, especially POAG, is associated with an increased risk of schizophrenia, bipolar disorder, and depressive disorder[16]. Furthermore, previous studies also indicate that the frequency of having anxiety and depression episodes is higher in patients with POAG and other subtypes of glaucoma[17−20]. A recent meta-analysis verifies that patients with glaucoma experience a higher prevalence and severity of depression, anxiety, and other psychological conditions[21]. Another meta-analysis also finds that the prevalence of depression is 25% among patients with glaucoma[22]. In reverse, a history of psychiatric disorders will exacerbate the development of glaucoma, suggesting that psychological disturbances would worsen glaucoma progression[23].
These interesting findings of observational studies have brought the potential role of glaucoma in the development of psychiatric disorders into the spotlight. Although some of them indicate a certain amount of pathophysiological and psychosocial risk factors, the insidious development of psychiatric disorders and glaucoma makes it difficult to recognize and prevent them in a timely manner. In addition, the previous observational findings might be biased by potential confounders. A positive clinical association means only an epidemiological comorbidity, while whether there is a causal relationship remains unexplored. As we already noted, there remain considerable limitations of the explanatory power of the observational results; therefore, a major breakthrough for current research will be to investigate the relevance of the potential risk exposures to the causation of these diseases using an innovative approach[24].
Through recent advances in genetics, psychiatric disorders and POAG were found to be highly polygenic and with an extensive biological pleiotropy[24−31]. The polygenic bases and the advances of genetic technologies provide an opportunity to explore their potential causal relationship at a number of both genetic and epidemiological levels. In the absence of convincing randomized controlled trials, Mendelian randomization is considered an alternative to estimate the causal association between two traits[32−36]. Based on the principle that genetic variants are randomly assigned, Mendelian randomization analysis can minimize the influences of confounding factors and reverse causality, which are considered to be limitations of observational epidemiological studies[37,38]. Therefore, a Mendelian randomization study estimating the potential causal relationship between psychiatric disorders and POAG is warranted.
In this study, we performed bi-directional two-sample Mendelian randomization analyses to evaluate the potential causal associations between a genetic liability to psychiatric disorders and glaucoma. By investigating the genetic causality, we aimed to provide new insights into the observed comorbidity in previous studies, serving as new evidence for early-stage prevention and diagnosis of psychiatric disorders and glaucoma.
-
Summary statistics of genome-wide association studies (GWASs) of the selected psychiatric disorders (i.e., schizophrenia, attention deficit/hyperactivity disorder [ADHD], anxiety disorder, bipolar disorder, and depressive disorder) and POAG were collected (Supplementary Table S1)[29,39−42]. Genetic information on schizophrenia was obtained from the GWAS summary statistics released by the Schizophrenia Working Group of the Psychiatric Genomics Consortium (PGC), which consisted of 15,358,497 single-nucleotide polymorphisms (SNPs) from 33,640 cases and 43,456 controls[40]. The GWAS summary-level dataset of ADHD was also obtained from the PGC, which contained 8,047,420 SNPs derived from 20,183 cases and 35,191 controls[41]. For anxiety disorder, summary statistics were acquired from FinnGen, including 12,513 cases and 198,110 controls[42]. The GWAS summary statistics for bipolar disorder were derived from a GWAS meta-analysis, which contained 9,483,147 SNPs, 7,647 cases, and 27,303 controls[39] The GWAS dataset for depressive disorder was sourced from FinnGen, which was based on 16,380,457 SNPs and consisted of 23,424 cases and 192,220 controls[42]. The summary statistics of the POAG discovery dataset were obtained from a GWAS meta-analysis, which included 15,229 cases and 177,473 controls[29]. Furthermore, an independent replication cohort (FinnGen, including 3,412 cases and 210,201 controls) was accessed and analyzed to confirm the findings in the discovery dataset when there was a positive result[42].
Detailed information about the study designs, including sample collection, quality control, and method imputation, was reported in each publication and was manually checked to avoid sample overlap[29,39−42]. All analyses in our study were conducted using publicly accessible, de-identified, and summary-level data; therefore, no additional ethical approval or informed consent was required.
Selection of genetic instrumental variables
-
A workflow of the general Mendelian randomization analysis process of this study is shown in Fig. 1. After collecting the abovementioned GWAS datasets for POAG and the five selected psychiatric disorders, we then selected SNPs as independent genetic instrumental variables (IVs) of exposure from them.
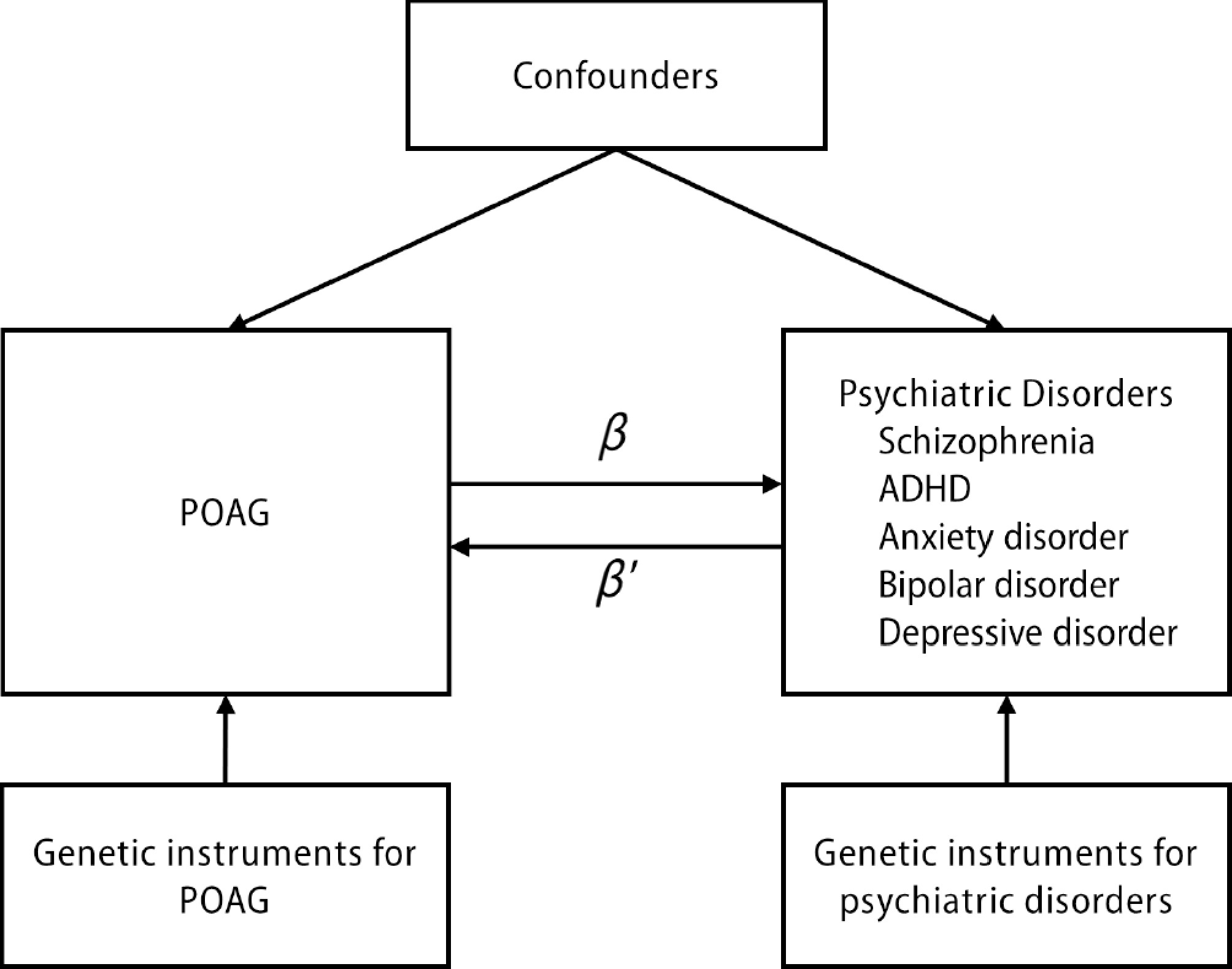
Figure 1.
Workflow figure of the bi-directional two-sample Mendelian randomization analysis process of this study. β and β' are the beta coefficients for the corresponding estimated causal effects.
The IVs for the five psychiatric disorders and POAG were selected using the same criteria. The IVs were extracted on the basis of the arbitrary p-value cut-off. All relevant SNPs at the GWAS significance threshold (p < 5 × 10−6) were selected from each trait with the aim of obtaining more IVs. Thereafter, all the selected SNPs were clumped by linkage disequilibrium with an r2 threshold of < 0.001 and a 10-Mb window to ensure that the IVs for the exposure datasets were independent. PhenoScanner V2 database (
http://phenoscanner.medschl.cam.ac.uk ) was applied to avoid potential confounding by calculating each IV and its proxies (r2 > 0.8)[43]. SNPs with indirect linkage disequilibrium effects (r2 > 0.8) were excluded to prevent association with the outcome. All the IVs selected needed to meet the following assumptions: (1) SNPs, as IVs, are strongly associated with the exposure. The F-statistic for each SNP was calculated as F = (beta_exposure/se_exposure)2, and the instrument strength > 10 was considered sufficient for analysis; (2) IVs are not associated with any confounding factors; (3) IVs are not directly associated with outcome (no horizontal pleiotropy)[44].Two-sample Mendelian randomization analysis
-
For the analysis of the causal relationship between POAG and the five common psychiatric disorders, bi-directional two-sample Mendelian randomization analysis was employed in our study. Mendelian randomization analysis was conducted first in one direction to investigate whether POAG has a genetically causal association with five common psychiatric disorders (schizophrenia, ADHD, anxiety disorder, bipolar disorder, and depressive disorder). Thereafter, Mendelian randomization analysis in the opposite direction was conducted to assess the reverse causality of these five common psychiatric disorders on POAG.
Inverse variance weighted (IVW) regression with multiplicative random effects method was adopted as the primary causal inference, since the IVW method provides robust causal estimations of the two traits and is most widely used in Mendelian randomization analyses[44]. Meanwhile, three alternative Mendelian randomization methods, including the Mendelian randomization–Egger (MR-Egger), the weighted median, and the weighted mode methods, were additionally performed in our analyses to complement and improve the reliability of the IVW results. The MR-Egger method uses the slope coefficient of the Egger regression to show the causal effect, which could provide a more robust estimation when there are no invalid IVs[45]. The weighted median method can even identify a positive causal estimation when up to 50% of IVs are invalid[46]. The weighted mode method estimates the evidence of causality by classifying the IVs into groups, which relaxes the assumptions of Mendelian randomization and is able to identify the causality even with a majority of invalid IVs[47]. The Mendelian randomization results aRE all reported as odds ratios (OR) with 95% confidence intervals (CIs), which were interpreted as the estimated causal effect per standard deviation (1 SD) of change in exposure on the outcome risk.
Sensitivity analysis
-
For validation of our putative causal association between POAG and the five common psychiatric disorders, sensitivity analyses were performed for IV quality control based on the results of Mendelian randomization.
Although the IVW method is generally recognized as a better method of causal inference, the validity of these Mendelian randomization results would be reliable only when all of the IVs are without heterogeneity and horizontal pleiotropy[47]. Therefore, for the traits with an IVW with p < 0.05 and IVs > 2, we performed heterogeneity tests using Cochran's Q test and the I2 index to detect the outlier IVs and adjust them[48]. The presence of heterogeneity was considered when p < 0.05 in Cochran's Q test and I2 index > 50%. The detected outliers were then discarded from the analyses.
Meanwhile, the Mendelian randomization pleiotropy residual sum and outlier (MR-PRESSO) global test and the MR-Egger regression test were performed to detect the presence of any horizontal and directional pleiotropy, respectively[45,49]. The MR-PRESSO method indicates the potential pleiotropic outliers through a correction test. Therefore, to reduce the effect of horizontal pleiotropy, potential pleiotropic outlier IVs detected by the MR-PRESSO outlier test would undergo stepwise removal. While in MR-Egger regression test results, the intercept was used to show the mean pleiotropic effects. The presence of pleiotropy was indicated by the MR-Egger regression method, and the IVW results were invalid at p < 0.05. In addition, leave-one-out analysis was also executed for traits with multiple IVs to check whether the reported causality was obviously driven by a single IV. Similarly, the indicated outlier IVs were detected to improve the results of Mendelian randomization. A value with p < 0.05 was considered as an outlier and removed from the analyses.
Bi-directional Mendelian randomization analysis
-
After investigating the causal association between POAG and the five common psychiatric disorders separately, we explored the reverse causality by extending the MR analysis above to bi-directional causal inference. As mentioned above, forward Mendelian randomization analyses were conducted by using POAG as the exposure and the psychiatric disorders as the outcomes. Conversely, the reverse Mendelian randomization analyses used individual psychiatric disorders as the exposure and POAG as the outcome to explore the potential causal association between POAG and psychiatric disorders. The standards of the parameters and the Mendelian randomization methods were set the same for the forward and reverse analyses, as well as the discovery and replication datasets.
A causality between the exposure and the outcome was accepted when the IVW result was significant and one of the following conditions was satisfied: (1) no heterogeneity was detected when the causal effects of the MR-Egger, weighted median, and weighted mode methods were in the same direction; (2) heterogeneity was detected but corrected by the MR-PRESSO global test (< 50% of IVs were considered as outliers); or (3) heterogeneity was detected and > 50% of the outliers were detected by MR-PRESSO global test, but the causal effects of the MR-Egger, weighted median, and weighted mode methods were significant and in the same direction[49−51].
A p-value of < 0.01 after Bonferroni correction was considered statistically significant, and a p-value between 0.01 and 0.05 was considered suggestively significant in our Mendelian randomization analyses. All two-sample Mendelian randomization analyses were performed using the TwoSampleMR R package in the R software (version 4.1.1)[52].
-
The GWAS summary statistics on the selected psychiatric disorders and POAG used in our study were carefully compared for database quality control. We manually checked the sample description of every GWAS summary dataset to make sure that the samples of the exposure were different from those of the outcome. Therefore, our Mendelian randomization results were unlikely to be influenced by sample overlap between each exposure–outcome pair. The list of IVs used for the Mendelian randomization analyses of POAG on psychiatric disorders of interest in this study is provided in Table 1.
Table 1. Detailed information of SNPs in the Mendelian randomization analysis of POAG and the psychiatric disorders of interest.
SNP Chr Location Association with SCZ Association with ADHD Association with AD Association with BD Association with DD β SE p β SE p β SE p β SE p β SE p rs10151220 14 34715465 / / / −0.204 0.182 0.262 / / / 0.198 0.295 0.501 / / / rs10160502 11 45376816 −0.030 0.146 0.838 −0.368 0.169 0.029 / / / −0.405 0.301 0.179 / / / rs10248136 7 39077397 −0.146 0.123 0.236 −0.120 0.152 0.430 −0.074 0.162 0.647 −0.283 0.255 0.266 −0.137 0.124 0.271 rs10268299 7 48105158 −0.261 0.171 0.126 −0.386 0.212 0.068 0.295 0.238 0.216 −0.542 0.343 0.114 0.079 0.183 0.667 rs10448285 9 129397014 0.064 0.096 0.505 −0.231 0.121 0.056 −0.197 0.124 0.110 −0.087 0.201 0.666 0.018 0.095 0.853 rs10517281 4 54027595 −0.062 0.139 0.653 −0.010 0.165 0.951 0.163 0.164 0.320 −0.067 0.288 0.817 −0.144 0.126 0.253 rs10800155 1 165723770 0.058 0.057 0.309 0.097 0.073 0.180 −0.025 0.063 0.684 −0.118 0.117 0.313 0.003 0.048 0.954 rs10906230 10 12851181 −0.030 0.169 0.861 −0.101 0.208 0.627 0.021 0.223 0.926 0.001 0.346 0.997 −0.284 0.171 0.097 rs109467 7 83278893 0.125 0.136 0.357 0.024 0.167 0.885 0.130 0.173 0.453 −0.800 0.277 0.004 0.188 0.134 0.160 rs1139795 22 19867771 0.074 0.106 0.487 0.130 0.133 0.330 −0.080 0.171 0.639 −0.011 0.213 0.961 / / / rs113985657 6 597203 −0.053 0.146 0.718 −0.152 0.168 0.367 0.020 0.171 0.905 −0.096 0.285 0.736 0.153 0.131 0.245 rs114367221 16 51601948 −0.155 0.138 0.262 / / / / / / −0.279 0.271 0.304 / / / rs11606709 11 46730522 0.566 0.169 0.001 0.034 0.201 0.867 0.017 0.222 0.939 0.310 0.341 0.363 −0.277 0.171 0.106 rs11658334 17 58830188 0.229 0.148 0.121 −0.336 0.183 0.067 0.032 0.193 0.868 0.094 0.304 0.757 −0.159 0.148 0.283 rs11694522 2 228085471 −0.068 0.168 0.683 0.003 0.205 0.990 −0.070 0.201 0.729 −0.083 0.351 0.813 0.039 0.155 0.803 rs117907084 8 8094540 −0.268 0.196 0.173 / / / 0.219 0.154 0.157 −0.359 0.426 0.400 0.069 0.118 0.561 rs11968883 6 158971411 0.053 0.152 0.730 0.000 0.191 1.000 −0.482 0.197 0.014 −0.337 0.316 0.287 −0.159 0.151 0.291 rs12133258 1 247990141 −0.098 0.159 0.537 0.012 0.196 0.950 / / / 0.069 0.321 0.831 / / / rs12208086 6 36586070 0.181 0.120 0.132 0.003 0.151 0.985 0.274 0.145 0.059 0.015 0.246 0.952 0.030 0.112 0.785 rs12238998 1 92052303 0.003 0.159 0.986 −0.108 0.198 0.587 −0.258 0.218 0.237 0.255 0.322 0.428 0.126 0.169 0.455 rs12421242 11 102066240 −0.022 0.155 0.889 0.069 0.188 0.716 0.089 0.199 0.656 0.170 0.314 0.589 0.043 0.153 0.779 rs12540035 7 116159526 −0.085 0.113 0.449 0.151 0.139 0.280 −0.028 0.183 0.877 0.068 0.227 0.764 −0.075 0.141 0.594 rs12548263 8 124498734 0.247 0.174 0.156 / / / −0.219 0.230 0.341 1.046 0.357 0.003 −0.001 0.177 0.994 rs12969002 18 11724979 0.411 0.161 0.011 0.060 0.197 0.761 −0.116 0.216 0.591 0.027 0.336 0.937 0.029 0.165 0.859 rs13022278 2 35862610 0.169 0.181 0.351 0.041 0.177 0.816 −0.329 0.225 0.143 0.184 0.299 0.539 −0.232 0.172 0.179 rs13085037 3 124312984 −0.005 0.163 0.977 0.299 0.200 0.135 0.060 0.186 0.749 0.182 0.337 0.589 −0.050 0.143 0.726 rs1385069 6 134374204 0.194 0.154 0.210 0.076 0.195 0.698 0.032 0.201 0.872 −0.020 0.314 0.950 0.365 0.154 0.018 rs1422174 5 92194417 −0.019 0.171 0.909 / / / −0.093 0.289 0.748 −0.579 0.386 0.133 0.065 0.221 0.770 rs145556337 2 200444431 0.118 0.133 0.372 / / / 0.030 0.171 0.862 0.092 0.362 0.800 0.217 0.131 0.097 rs150372522 18 65972342 0.179 0.168 0.285 −0.077 0.204 0.705 −0.201 0.251 0.425 −0.060 0.335 0.859 −0.235 0.194 0.227 rs1577488 1 101078400 −0.044 0.129 0.733 −0.025 0.163 0.879 0.259 0.150 0.085 0.096 0.265 0.718 −0.018 0.116 0.878 rs1649068 10 60304864 0.158 0.103 0.123 0.289 0.125 0.021 0.072 0.135 0.595 0.089 0.208 0.671 0.048 0.104 0.643 rs17125973 14 53415359 0.114 0.168 0.498 0.283 0.204 0.164 0.192 0.231 0.405 0.293 0.345 0.395 0.034 0.177 0.847 rs1743080 14 92020604 0.061 0.151 0.684 −0.008 0.184 0.967 −0.242 0.216 0.261 0.814 0.304 0.007 0.029 0.166 0.860 rs17527016 4 111963719 −0.133 0.125 0.287 / / / 0.123 0.147 0.404 0.113 0.237 0.633 −0.076 0.113 0.500 rs190835765 4 38483655 0.019 0.133 0.889 / / / 0.323 0.133 0.015 0.311 0.259 0.230 0.076 0.102 0.453 rs2027312 9 129920463 −0.094 0.132 0.474 0.077 0.161 0.630 0.082 0.178 0.644 −0.038 0.266 0.888 0.153 0.137 0.265 rs2113818 2 12890860 0.255 0.155 0.101 −0.172 0.189 0.363 0.236 0.205 0.249 0.124 0.317 0.696 0.054 0.158 0.732 rs2207441 6 164325217 −0.127 0.154 0.410 0.305 0.189 0.107 0.023 0.193 0.905 −0.200 0.322 0.535 −0.246 0.148 0.097 rs2439386 15 67025403 −0.072 0.164 0.662 0.340 0.200 0.090 0.035 0.224 0.877 −0.101 0.345 0.770 −0.010 0.171 0.955 rs2472494 9 107695539 0.104 0.059 0.076 −0.026 0.074 0.724 0.031 0.078 0.695 −0.019 0.118 0.872 −0.044 0.060 0.463 rs2514879 8 108273318 −0.172 0.135 0.203 −0.014 0.162 0.929 −0.236 0.176 0.178 0.352 0.273 0.197 0.089 0.135 0.508 rs2526100 7 11677778 −0.010 0.159 0.952 −0.091 0.190 0.631 −0.147 0.212 0.489 0.190 0.324 0.558 −0.223 0.163 0.171 rs257336 16 65055840 −0.210 0.132 0.112 0.115 0.161 0.476 / / / 0.656 0.270 0.015 / / / rs2579998 6 51477322 0.021 0.084 0.803 0.157 0.101 0.121 0.143 0.104 0.172 0.087 0.173 0.616 0.189 0.080 0.018 rs2667477 12 84023388 0.120 0.101 0.234 −0.137 0.123 0.266 −0.008 0.140 0.953 0.393 0.204 0.054 −0.111 0.108 0.305 rs2735114 6 29910034 0.568 0.196 0.004 −0.006 0.166 0.970 −0.075 0.181 0.679 0.422 0.278 0.128 0.227 0.138 0.101 rs28497695 15 57023951 0.284 0.126 0.025 / / / −0.157 0.164 0.337 0.481 0.254 0.058 −0.273 0.125 0.030 rs286487 10 90030119 −0.082 0.165 0.620 0.284 0.198 0.151 0.001 0.224 0.995 −0.091 0.338 0.787 −0.136 0.172 0.427 rs2875238 11 130282078 −0.033 0.158 0.832 −0.057 0.211 0.785 −0.107 0.203 0.599 0.206 0.319 0.519 −0.151 0.156 0.334 rs31916 5 14814883 0.150 0.171 0.381 0.064 0.208 0.758 −0.021 0.227 0.925 −0.422 0.355 0.235 0.013 0.174 0.941 rs33155 12 30985442 / / / −0.245 0.179 0.170 0.280 0.182 0.125 −0.132 0.304 0.663 0.249 0.140 0.077 rs33912345 14 60976537 / / / / / / 0.145 0.088 0.099 0.016 0.127 0.901 −0.007 0.067 0.920 rs34163217 1 178586984 0.080 0.173 0.643 −0.001 0.205 0.995 −0.275 0.233 0.238 −0.591 0.350 0.092 0.239 0.180 0.182 rs34508066 3 66837509 0.126 0.157 0.423 0.130 0.196 0.506 0.104 0.215 0.630 −0.128 0.322 0.691 −0.091 0.165 0.580 rs35592623 8 120702717 0.048 0.177 0.788 0.042 0.225 0.850 0.313 0.222 0.159 0.069 0.374 0.854 0.253 0.171 0.138 rs35666652 11 86491772 −0.141 0.163 0.385 −0.050 0.199 0.802 0.416 0.227 0.068 0.379 0.336 0.259 / / / rs3825942 15 74219582 / / / −0.275 0.150 0.066 0.114 0.153 0.455 0.075 0.251 0.766 0.183 0.117 0.120 rs3909355 5 120654808 −0.148 0.176 0.399 −0.056 0.215 0.794 −0.502 0.203 0.014 −0.151 0.362 0.676 −0.346 0.156 0.026 rs4076000 1 68837169 / / / 0.058 0.188 0.757 0.003 0.197 0.989 0.348 0.310 0.263 0.112 0.152 0.462 rs41283694 10 60156574 0.218 0.171 0.202 0.055 0.226 0.807 −0.127 0.450 0.777 0.836 0.327 0.011 0.329 0.350 0.347 rs4142696 12 26800201 −0.153 0.172 0.374 0.107 0.210 0.611 −0.271 0.203 0.181 0.049 0.352 0.890 −0.158 0.155 0.310 rs41543317 17 44087500 / / / 0.142 0.167 0.395 0.039 0.169 0.817 −0.142 0.275 0.605 0.001 0.130 0.993 rs4307771 2 213723819 −0.067 0.154 0.666 / / / 0.323 0.238 0.175 −0.380 0.325 0.242 0.305 0.183 0.096 rs4414666 2 66537344 0.098 0.152 0.518 0.097 0.187 0.605 −0.057 0.202 0.779 0.425 0.319 0.182 −0.188 0.155 0.223 rs4441044 11 69500363 −0.016 0.158 0.918 −0.158 0.194 0.416 −0.152 0.220 0.488 0.229 0.319 0.473 −0.205 0.168 0.224 rs4612174 6 136462744 −0.020 0.097 0.837 −0.142 0.121 0.241 −0.051 0.124 0.680 0.144 0.200 0.472 −0.103 0.095 0.279 rs4652964 1 38078300 −0.226 0.157 0.150 −0.300 0.190 0.113 −0.203 0.208 0.331 0.270 0.319 0.397 −0.322 0.159 0.044 rs4653159 1 36579215 / / / 0.298 0.156 0.056 −0.057 0.167 0.733 0.102 0.270 0.707 −0.004 0.128 0.977 rs4775427 15 61951235 0.126 0.145 0.383 0.148 0.176 0.400 −0.214 0.189 0.257 0.088 0.297 0.767 0.125 0.145 0.388 rs4842316 12 79974565 −0.180 0.157 0.252 −0.251 0.192 0.191 −0.007 0.220 0.976 0.602 0.318 0.058 −0.129 0.169 0.446 rs55882252 2 153361700 0.131 0.110 0.237 0.159 0.136 0.241 0.033 0.144 0.816 0.067 0.224 0.765 −0.079 0.110 0.474 rs56233426 3 186128816 0.089 0.109 0.416 0.116 0.157 0.462 −0.061 0.138 0.660 0.284 0.224 0.204 / / / rs565066 11 56871325 −0.218 0.160 0.172 0.123 0.195 0.528 −0.057 0.228 0.803 0.269 0.324 0.405 −0.230 0.176 0.191 rs5750494 22 38176979 0.072 0.156 0.646 0.474 0.191 0.013 0.072 0.199 0.718 0.236 0.312 0.449 0.007 0.153 0.964 rs58073046 11 120248493 0.202 0.103 0.050 0.245 0.121 0.043 0.186 0.131 0.155 0.374 0.207 0.071 −0.061 0.101 0.543 rs58265464 5 149408929 0.065 0.147 0.658 0.243 0.188 0.197 / / / 0.288 0.298 0.334 / / / rs6117318 20 6507717 −0.115 0.127 0.363 0.144 0.151 0.343 / / / 0.134 0.253 0.595 / / / rs62283811 3 171820890 0.168 0.143 0.239 −0.201 0.181 0.265 0.043 0.167 0.797 −0.012 0.370 0.975 0.026 0.128 0.842 rs6475604 9 22052734 −0.005 0.042 0.913 0.008 0.051 0.882 −0.012 0.054 0.824 0.115 0.085 0.177 0.019 0.042 0.656 rs6490697 13 22679011 −0.003 0.119 0.978 0.007 0.144 0.963 0.083 0.144 0.563 −0.096 0.248 0.699 −0.154 0.111 0.167 rs6519133 22 39096602 0.099 0.154 0.523 −0.308 0.205 0.134 0.112 0.193 0.562 0.312 0.310 0.315 −0.189 0.148 0.201 rs6602453 10 10840849 0.246 0.145 0.089 0.242 0.177 0.172 −0.067 0.196 0.731 −0.026 0.293 0.929 −0.140 0.150 0.351 rs6729430 2 11934756 −0.096 0.210 0.649 / / / / / / 0.388 0.314 0.217 / / / rs6845653 4 7899379 0.027 0.067 0.688 0.130 0.084 0.122 −0.046 0.085 0.589 0.040 0.138 0.771 −0.055 0.065 0.400 rs686768 11 86361508 0.173 0.129 0.180 −0.259 0.157 0.099 0.195 0.163 0.231 −0.041 0.268 0.879 0.120 0.126 0.338 rs687914 2 45878760 / / / −0.090 0.212 0.672 −0.061 0.241 0.802 −0.426 0.338 0.207 0.156 0.185 0.399 rs6920127 6 92582660 −0.047 0.172 0.785 −0.063 0.210 0.765 −0.024 0.223 0.916 −0.375 0.353 0.288 −0.108 0.171 0.527 rs6951875 7 103632175 / / / −0.280 0.223 0.209 −0.029 0.227 0.900 −0.341 0.360 0.344 0.038 0.174 0.827 rs7099316 10 126469005 0.017 0.152 0.912 0.402 0.184 0.029 0.120 0.201 0.550 0.474 0.309 0.126 −0.153 0.155 0.322 rs7137828 12 111932800 −0.006 0.116 0.957 0.136 0.144 0.346 0.009 0.150 0.950 0.203 0.234 0.386 −0.050 0.116 0.665 rs72637444 13 97876689 0.149 0.192 0.436 −0.159 0.222 0.472 0.080 0.232 0.729 −0.413 0.372 0.268 −0.021 0.179 0.909 rs7275118 20 18010447 0.155 0.155 0.317 −0.214 0.197 0.276 −0.028 0.197 0.886 −0.407 0.321 0.204 −0.111 0.151 0.464 rs73071655 20 1121939 −0.082 0.173 0.636 0.027 0.217 0.901 0.685 0.243 0.005 0.154 0.354 0.663 0.105 0.187 0.574 rs735379 2 34257592 −0.213 0.173 0.219 −0.192 0.214 0.369 0.089 0.228 0.697 0.337 0.361 0.350 0.011 0.175 0.948 rs754634 14 75097431 0.070 0.174 0.686 0.053 0.214 0.805 0.233 0.226 0.304 −0.016 0.354 0.964 0.144 0.174 0.409 rs7739648 6 1540483 0.167 0.091 0.067 −0.174 0.110 0.116 0.054 0.116 0.639 −0.242 0.186 0.193 −0.092 0.089 0.300 rs782610 2 55935395 −0.142 0.155 0.359 0.330 0.189 0.080 −0.353 0.231 0.126 −0.254 0.315 0.420 −0.082 0.177 0.645 rs78914827 5 133415082 −0.023 0.153 0.880 −0.066 0.183 0.718 0.026 0.226 0.907 −0.321 0.317 0.312 −0.104 0.173 0.549 rs7946009 11 128387422 0.083 0.155 0.593 0.086 0.192 0.655 0.061 0.200 0.760 −0.393 0.315 0.213 0.102 0.154 0.507 rs7969703 12 18218609 0.097 0.176 0.581 0.298 0.210 0.155 0.163 0.192 0.396 −0.191 0.368 0.604 0.154 0.148 0.297 rs929218 7 117653665 −0.186 0.151 0.218 0.156 0.186 0.401 −0.538 0.194 0.005 −0.802 0.304 0.008 −0.120 0.150 0.424 rs9470997 6 39166247 0.165 0.157 0.294 0.235 0.193 0.224 0.124 0.205 0.544 0.769 0.330 0.020 −0.048 0.157 0.762 rs9544017 13 76247179 −0.099 0.135 0.463 −0.296 0.166 0.074 0.309 0.176 0.078 0.104 0.272 0.703 0.163 0.135 0.226 rs9819278 3 85144350 0.033 0.121 0.785 0.260 0.150 0.083 0.065 0.156 0.676 −0.363 0.249 0.145 0.029 0.120 0.811 rs9913911 17 10031183 0.024 0.074 0.745 −0.024 0.094 0.799 0.025 0.096 0.791 −0.064 0.159 0.689 0.117 0.074 0.111 rs993471 1 103385373 / / / 0.059 0.158 0.711 −0.449 0.176 0.011 −0.537 0.265 0.043 −0.277 0.135 0.040 All - Inverse variance weighted 0.035 0.013 0.008 0.021 0.017 0.214 0.016 0.016 0.325 0.040 0.027 0.143 −0.008 0.013 0.526 All - MR Egger 0.047 0.034 0.172 0.019 0.047 0.686 0.077 0.042 0.069 0.054 0.072 0.458 0.046 0.033 0.165 ADHD, attention deficit/hyperactivity disorder; AD, anxiety disorder; BD, bipolar disorder; Chr, chromosome; DD, depressive disorder; POAG, primary open-angle glaucoma; SCZ, schizophrenia; SE, standard error; SNP, single-nucleotide polymorphism. The putative causal effect of POAG on psychiatric disorders
-
According to the current epidemiological findings on glaucoma and psychiatric disorders, glaucoma patients are prone to developing psychiatric disorders during disease progression. As such, we first performed the forward Mendelian randomization analysis of POAG on each psychiatric disorder of interest to investigate the causality. The summarized results of all forward Mendelian randomization analyses are shown in Table 2, Fig. 2, and Supplementary Fig. S1. More detailed information on the forward Mendelian randomization analyses, such as the results of the assessment of heterogeneity, as well as the MR-Egger regression test and the MR-PRESSO outlier test, is provided in Table 2 and Table 3.
Table 2. Mendelian randomization analysis for the causal effects of POAG on psychiatric disorders of interest.
Exposure Outcome Method SNPs Mendelian randomization Heterogeneity OR LL UL p Q Q_p POAG SCZ IVW 97 1.035 1.009 1.062 0.008 101.545 0.330 MR-Egger 97 1.048 0.980 1.121 0.172 101.383 0.308 Weighted median 97 1.026 0.986 1.067 0.214 Weighted mode 97 1.028 0.973 1.087 0.328 MR PRESSO 97 1.035 1.009 1.062 0.008 ADHD IVW 96 1.022 0.988 1.056 0.214 113.915 0.090 MR-Egger 96 1.019 0.930 1.117 0.686 113.911 0.079 Weighted median 96 1.009 0.957 1.065 0.732 Weighted mode 96 1.028 0.948 1.115 0.505 MRPRESSO 96 1.022 0.988 1.056 0.214 AD IVW 99 1.016 0.984 1.049 0.325 103.610 0.330 MR-Egger 99 1.080 0.995 1.171 0.069 101.019 0.370 Weighted median 99 1.020 0.970 1.073 0.443 Weighted mode 99 1.000 0.935 1.070 0.994 MR-PRESSO 99 1.016 0.984 1.049 0.325 BD IVW 107 1.040 0.987 1.097 0.143 128.276 0.070 MR-Egger 107 1.055 0.916 1.215 0.458 128.222 0.061 Weighted median 107 1.048 0.972 1.129 0.222 Weighted mode 107 1.048 0.938 1.171 0.407 MR-PRESSO 107 1.040 0.987 1.097 0.143 DD IVW 96 0.992 0.967 1.017 0.526 104.871 0.229 MR-Egger 96 1.047 0.982 1.116 0.165 101.382 0.283 Weighted median 96 1.002 0.964 1.042 0.914 Weighted mode 96 0.996 0.946 1.049 0.883 MR-PRESSO 96 0.992 0.967 1.017 0.526 ADHD, attention deficit/hyperactivity disorder; AD, anxiety disorder; BD, bipolar disorder; DD, depressive disorder; IVW, inverse variance weighted; LL, lower limits of odds ratio; OR, odds ratio; POAG, primary open-angle glaucoma; SCZ, schizophrenia; SNP, single-nucleotide polymorphism; UL, upper limits of odds ratio. 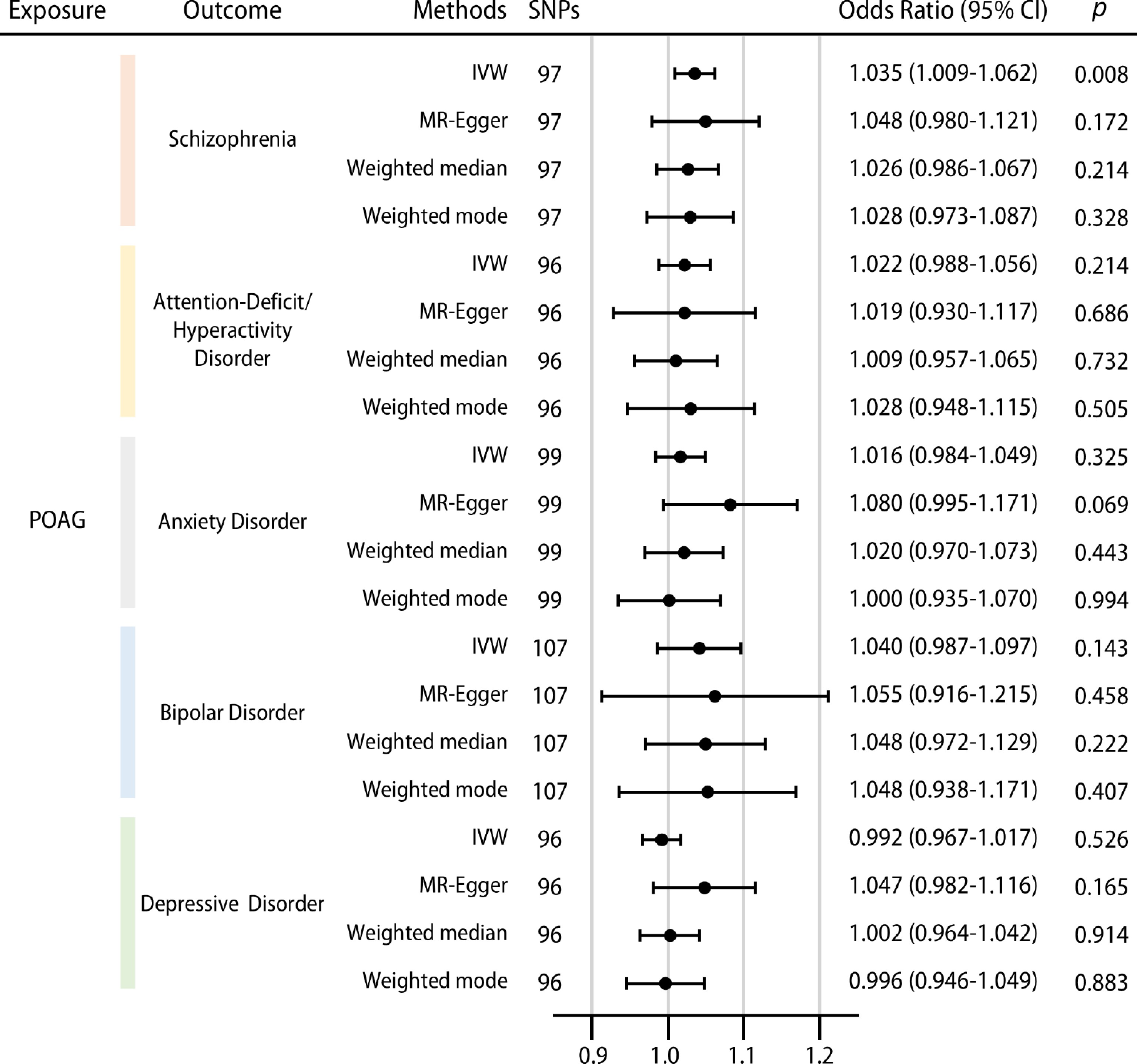
Figure 2.
The causal effects of POAG on schizophrenia (SCZ), ADHD, anxiety disorder (AD), bipolar disorder (BD), and depressive disorder (DD). Error bars represent the 95% confidence intervals[39] for the estimated effects. IVW, inverse variance weighting.
Table 3. Assessment of the pleiotropy of the Mendelian randomization analysis for the causality of POAG on the psychiatric disorders of interest.
Exposure Outcome MR-Egger intercept MR-PRESSO global test Intercept SE p RSSobs p POAG SCZ −1.406E-03 3.620E-03 0.699 103.453 0.357 ADHD 2.562E-04 4.768E-03 0.957 116.353 0.095 AD −6.995E-03 4.435E-03 0.118 105.523 0.349 BD −1.589E-03 7.535E-03 0.833 130.448 0.079 DD −6.239E-03 3.469E-03 0.075 106.935 0.252 ADHD, attention deficit/hyperactivity disorder; AD, anxiety disorder; BD, bipolar disorder; DD, depressive disorder; POAG, primary open-angle glaucoma; SCZ, schizophrenia; SE, standard error. Our results showed that genetically predicted POAG was significantly and positively associated with schizophrenia when considering the best causal estimation (IVW OR = 1.035, 95% CI: 1.009−1.062, p = 0.008; all results from four different methods were directionally consistent) (Table 2, Fig. 2). A p-value of 0.008 < 0.01 (adjusted p-value with Bonferroni correction for multiple testing) was considered significant. A forest plot visually displayed the positive association between genetic liability to POAG and schizophrenia risk (Supplementary Fig. S1a). Cochran's Q test revealed no heterogeneity across the recruited IVs (Q = 101.545, p = 0.330) (Table 2). The MR-PRESSO global test and MR-Egger regression test detected no presence of any horizontal pleiotropy or directional pleiotropy (MR-Egger intercept = −1.406 × 10−3, SE = 3.620 × 10−3, p = 0.699; MR-PRESSO global test, p = 0.357) (Table 3). The leave-one-out test detected no outliers, and the result was stable and would not be significantly altered by any individual SNP (Supplementary Fig. S2a). This is also presented in the funnel plot (Supplementary Fig. S3a). The scatter plot of genetic association with POAG versus genetic association with schizophrenia showed a significantly positive causality between the two diseases (Fig. 3a).
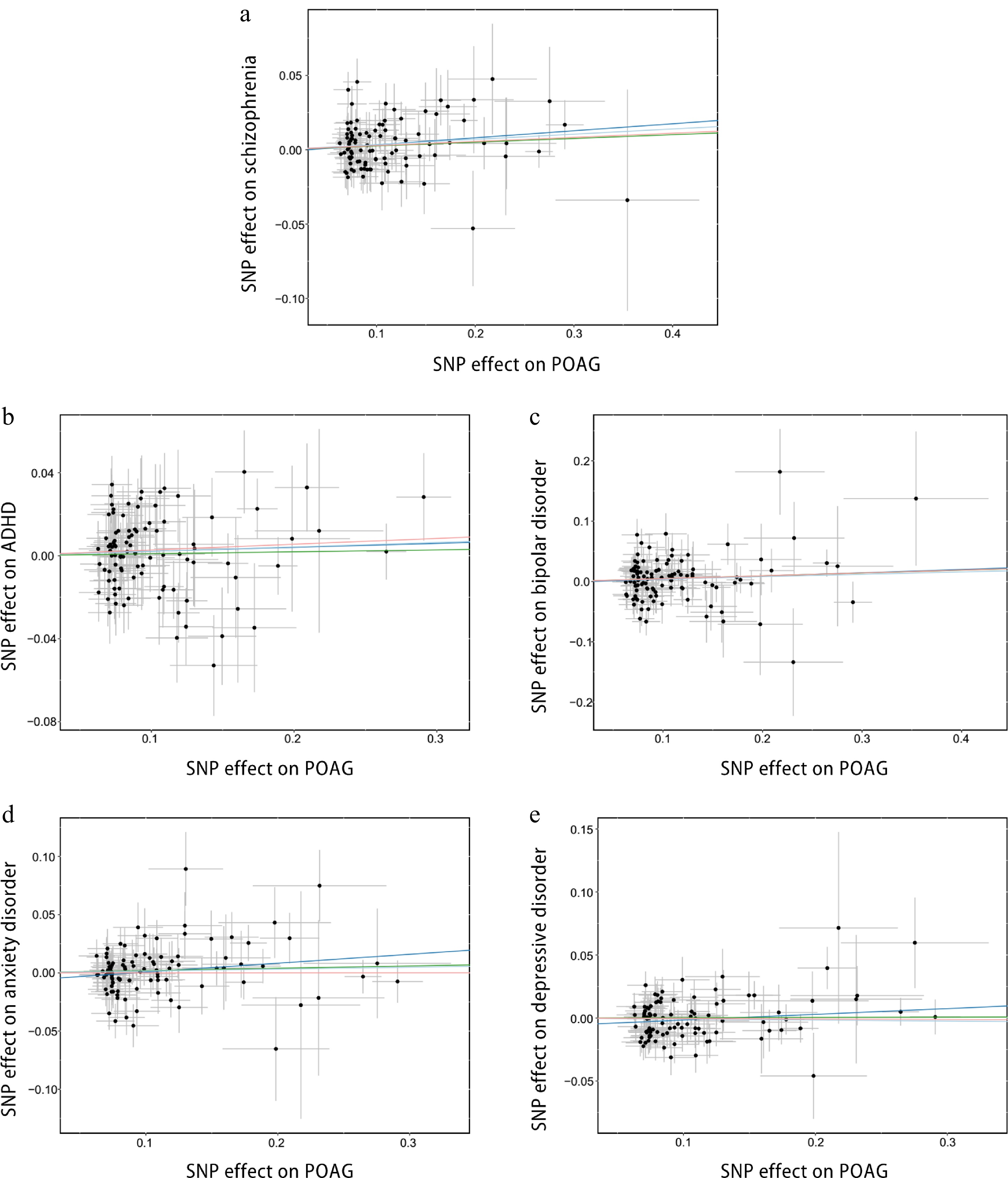
Figure 3.
Scatter plots of the causal effects of POAG on the psychiatric disorders of interest. (a) Effects of POAG on schizophrenia (SCZ); (b) effects of POAG on ADHD; (c) effects of POAG on anxiety disorder (AD); (d) effects of POAG on bipolar disorder (BD); (e) effects of POAG on depressive disorder (DD). The slope of each line indicates the causal effects estimated by each method. Light blue, inverse variance weighted (IVW) method; dark blue, MR-Egger method; green, weighted median method; pink, weighted mode method. SNP, single nucleotide polymorphism.
As for the other psychiatric disorders, the estimated causality consistently suggested that genetic predisposition to POAG was not related to any of them. Our results showed no evidence of the causal associations of POAG with ADHD (IVW OR = 1.022, 95% CI: 0.988−1.056, p = 0.214) (Table 2, Fig. 2). All four models suggested consistent results of no causality, even though no heterogeneity and pleiotropy were detected (Q = 113.915, p = 0.090; MR-Egger intercept = 2.562 × 10−4, SE = 4.768 × 10−3, p = 0.957; MR-PRESSO global test, p = 0.095) (Table 2, Table 3). This estimated effect was stable with no outliers, as detected by the leave-one-out test (Supplementary Fig. S2b) and shown in the funnel plot (Supplementary Fig. S3b). The scatter plot and forest plot also show a lack of association between POAG and ADHD (Fig. 3b, Supplementary Fig. S1b). Similarly, other causal association estimations suggested that genetic predisposition to POAG was not related to anxiety disorder (IVW OR = 1.016, 95% CI: 0.984−1.049, p = 0.325), bipolar disorder (IVW OR = 1.040, 95% CI: 0.987−1.097, p = 0.143), or depressive disorder (IVW OR = 0.992, 95% CI: 0.967−1.017, p = 0.526) (Table 2, Fig. 2), and were not disturbed by any heterogeneity or pleiotropy (Tables 2, 3). In addition, no outliers were found by the leave-one-out test (Supplementary Fig. S2c–e), and the corresponding results were demonstrated individually by funnel plots (Supplementary Fig. S3c–e). The scatter plots and forest plots presented no evidence of the causal effect of POAG on anxiety disorder, bipolar disorder, and depressive disorder (Fig. 3c–e and Supplementary Fig. S1c–e).
The putative causality of psychiatric disorders on POAG
-
After conducting the forward analyses, we found that only schizophrenia was genetically caused by POAG, while the other disorders were not. Nevertheless, whether this was a unidirectional causality remained inconclusive. Therefore, we performed the reverse analyses by extending the forward ones to the corresponding bi-directional causal inferences. Through using individual psychiatric disorders as the exposure and POAG as the outcome, we further explored whether there was any reverse causality from a genetic liability to psychiatric disorders to POAG. A summary of the reverse causality results is shown in Table 4 and Supplementary Fig. S4. Other results, such as the assessment of heterogeneity, as well as the MR-Egger regression test and the MR-PRESSO outlier test, are demonstrated in Table 4 and Supplementary Table S2 .
Table 4. Mendelian randomization analysis for the causal effect of the psychiatric disorders of interest on POAG.
Exposure Outcome Method SNPs Mendelian randomization Heterogeneity OR LL UL p Q Q_p SCZ POAG IVW 62 1.034 0.983 1.088 0.192 67.835 0.256 MR-Egger 62 1.022 0.847 1.232 0.823 67.815 0.228 Weighted median 62 1.042 0.971 1.118 0.250 Weighted mode 62 1.068 0.923 1.235 0.381 MR PERSSO 62 1.034 0.983 1.088 0.192 ADHD POAG IVW 41 0.941 0.880 1.006 0.074 47.089 0.205 MR Egger 41 0.824 0.615 1.104 0.202 46.107 0.202 Weighted median 41 0.951 0.869 1.042 0.282 Weighted mode 41 0.976 0.811 1.176 0.803 MR-PRESSO 41 0.941 0.880 1.006 0.074 47.089 0.205 AD POAG IVW 14 1.085 0.970 1.213 0.153 7.889 0.851 MR-Egger 14 1.039 0.798 1.354 0.779 7.767 0.803 Weighted median 14 1.109 0.960 1.281 0.159 Weighted mode 14 1.113 0.902 1.372 0.337 MR-PRESSO 14 1.085 0.970 1.213 0.153 BD POAG IVW 28 1.039 0.997 1.083 0.068 13.929 0.982 MR-Egger 28 1.037 0.945 1.139 0.450 13.927 0.974 Weighted median 28 1.041 0.979 1.107 0.198 Weighted mode 28 1.034 0.951 1.123 0.441 MR-PRESSO 28 1.039 0.997 1.083 0.068 DD POAG IVW 25 1.084 0.977 1.202 0.129 25.029 0.404 MR-Egger 25 0.995 0.795 1.245 0.967 24.280 0.388 Weighted median 25 1.132 0.970 1.321 0.115 Weighted mode 25 1.208 0.911 1.602 0.202 MR-PRESSO 25 1.084 0.977 1.202 0.129 ADHD, attention deficit/hyperactivity disorder; AD, anxiety disorder; BD, bipolar disorder; DD, depressive disorder; IVW, inverse variance weighted; LL, lower limits of odds ratio; OR, odds ratio; POAG, primary open-angle glaucoma; SCZ, schizophrenia; SNP, single-nucleotide polymorphism; UL, upper limits of odds ratio. Our results reported that genetic susceptibility to schizophrenia failed to be associated with POAG (IVW OR = 1.034, 95% CI: 0.983−1.088, p = 0.192) (Table 4). All four models consistently demonstrated the same. The forest plot did not display any causal associations (Supplementary Fig. S4a). After performing Cochran's Q test, no heterogeneity was detected (Q = 67.835, p = 0.256) (Table 4). No horizontal and directional pleiotropy was indicated by the MR-PRESSO global test (MR-PRESSO global test p = 0.278) and the MR-Egger regression test (MR-Egger intercept = 1.042 × 10−3, SE = 7.863 × 10−3, p = 0.895), respectively (Supplementary Table S2). The leave-one-out test and funnel plot showed no outliers; therefore, the estimated causal effect of schizophrenia on POAG was stable and would not be significantly influenced by any SNP (Supplementary Figs S5a and S6a). The invalid causal effect was also demonstrated in the scatter plot (Supplementary Fig. S7a).
As for the other psychiatric disorders, including ADHD (IVW OR = 0.941, 95% CI: 0.880−1.006, p = 0.074), anxiety disorder (IVW OR = 1.085, 95% CI: 0.970−1.213, p = 0.153), bipolar disorder (IVW OR = 1.039, 95% CI: 0.997−1.083, p = 0.068), and depressive disorder (IVW OR = 1.084, 95% CI: 0.977−1.202, p = 0.129), our results indicated that there was a lack of a causal effect of these psychiatric disorders on POAG (Table 4 and Supplementary Fig. S4b−e). No evidence of heterogeneity and pleiotropy was found among them (Table 4 and Supplementary Table S2). Other results, such as those of the leave-one-out tests, funnel plots, and scatter plots, are presented in Supplementary Figs S5b−e, S6b−e, and S7b−e.
Validation of the putative causality between POAG and schizophrenia
-
Since a genetic predisposition to POAG was positively associated with the incidence of schizophrenia, a validation dataset was introduced to further validate the putative causal relationship. Repeatedly, as the discovery dataset, we performed both a bi-directional two-sample Mendelian randomization analysis to investigate the existence and direction of the putative causality. The summarized results of the validation dataset are shown in Supplementary Tables S3 and S4.
A significantly and positively causal effect of the genetic predisposition to POAG on the risk of schizophrenia was reported and validated when considering the best causal estimation in the validation dataset (IVW OR = 1.062, 95% CI: 1.016−1.109, p = 0.007; all results from four different methods were directionally consistent) (Supplementary Table S3). A p-value of 0.007 < 0.01 (adjusted p-value after Bonferroni correction) was considered to be significant. The forest plot and scatter plot presented the positive association between POAG and the risk of schizophrenia visually (Supplementary Fig. S8a, b). No evidence of heterogeneity and pleiotropy was revealed by the Cochran's Q test (Q = 2.009, p = 0.919) (Supplementary Table S3), or the MR-PRESSO global test (MR-PRESSO global test p = 0.916) and MR-Egger regression test (MR-Egger intercept = 1.125 × 10−3, SE = 2.382 × 10−2, p = 0.964) (Supplementary Table S5). The leave-one-out plot and funnel plots are presented in Supplementary Fig. S8c, d.
In contrast, no causal effect of schizophrenia on POAG was found in the reverse analysis of the validation dataset (IVW OR = 0.970, 95% CI: 0.887−1.061, p = 0.510) (Supplementary Table S4). Detailed information is shown in the corresponding tables and figures (Supplementary Table S6 and Supplementary Fig. S9a−d). This result served as a good validation of our discovery dataset.
-
Psychiatric diseases and glaucoma are increasingly prevalent, accounting for continual rises in healthcare costs, which are becoming a substantial share of disability cases in the general population worldwide[1−5,53,54]. Currently, increasing studies remind us of the comorbidity between psychiatric diseases and glaucoma[10−13]. A significantly higher prevalence of psychiatric disorders was observed in patients with glaucoma, and vice versa[14−20,23,55]. These epidemiological findings suggested that psychiatric disorders and glaucoma may be closely correlated. However, given the limitations of the observational studies, simply and superficially relying on the observational studies will never be satisfactory. Current understandings have been restricted to observing their comorbidity rather than extending to a causality study.
To the best of our knowledge, our study comprehensively explored the causal associations between psychiatric disorders and glaucoma. We suggest that genetically predicted POAG is mildly associated with the risk of schizophrenia, whereas schizophrenia was not causally associated with POAG. No evidence of a causal association between POAG and other psychiatric disorders, including ADHD, anxiety disorder, bipolar disorder, and depressive disorder, was found.
Our findings add updated knowledge to the observational findings for POAG and schizophrenia. This is consistent with the recent studies demonstrating that a diagnosis of glaucoma preceded a diagnosis of schizophrenia[16,56]. Several studies also found that patients with glaucoma have a higher prevalence of schizophrenia[14−16]. The retinal vascular trajectory, which was related to retinal nerve fiber layer thinning and retinal vasculature, was closely related to schizophrenia and might explain the causal association[57]. In addition, microvascular dysfunction in the retinal arterioles was also observed in both glaucoma and schizophrenia, indicating their connections[58−60]. More importantly, CAV1 and CAV2, which are significantly associated with POAG, were also indicated to be involved in the development of schizophrenia[61−65]. The involvement of neurodegenerative disease-related factors should also be given careful consideration. Higher polygenic risk for schizophrenia was reported to be associated with a thinner ganglion cell inner plexiform layer (GC-IPL) thickness[66]. Patients with schizophrenia were also found to show measurable differences in retinal neural integrity, such as reduced macular GC-IPL and retinal nerve fiber layer (RNFL) thicknesses, which are hallmarks of glaucoma's development and progression[67]. One of the neurotrophic factors, called brain-derived neurotrophic factor (BDNF), was found to be associated with schizophrenia[68]. BDNF supports the survival and functional maintenance of retinal ganglion cells, whose degeneration is a hallmark of glaucoma[69]. However, the causal association is mild in our study, and larger-scale datasets are required to further validate the findings. The latest literature has also reported that sleep-related factors, such as getting up easily in the morning and sleep duration, are associated with a higher risk of POAG[70]. We believe that future analyses using more comprehensive datasets will provide valuable evidence of the potential mediators in the complex mechanisms between POAG and psychiatric disorders.
Intriguingly, our findings are in contrast to other studies that reported the associations between other psychiatric disorders and glaucoma[17−20]. Nevertheless, those observed associations might be due to unmeasured confounding factors and biases of the observational research, and the current evidence is not adequate to support the existence of a causal association. Furthermore, psychiatric disorders are among the comorbid conditions that are often present among patients with chronic diseases[71,72]. Since patients with glaucoma often suffer from a chronic disease process and are continuously afraid of blindness, they are prone to developing psychiatric disorders, such as anxiety and depression[12,73,74]. In addition, there are several clinical studies implying that the anticholinergic effects of antipsychotics used among patients with psychiatric diseases could increase the intraocular pressure and contribute to the development of glaucoma[75,76]. All of these serve as confounders that reduce the explanatory power of the observational results.
One of the strengths of our study lies in the bi-directional two-sample Mendelian randomization design. Mendelian randomization is thought to offer a 'natural' randomized trial for large-scale populations, and is considered to be Mother Nature's randomized controlled trial, ranking at the top in the hierarchy of the scientific evidence pyramid[37]. This approach makes our study less susceptible to confounders, reverse causality, and error measurement. Additionally, we are able to estimate the bi-directional causal associations with a validation dataset to prevent the possibility of false positive results. We also performed a series of sensitivity analyses to ensure the consistency of our causal estimation and the absence of any heterogeneity or pleiotropy, making our findings more credible. Investigating the genetic causal association could help to further understand how genetic variants contribute to the disease's development and progression. Besides the delivery of high-quality interventions, our identification and quantification of causality are also vital for the implementation of effective prevention strategies. Our study also has limitations. A less stringent threshold (p < 5 × 10−6) was adopted as the trade-off between IV quality and quantity. Although we made efforts to ensure the robustness of the results by implementing rigorous sensitivity approaches, such as the MR-Egger, weighted median, and MR-PRESSO methods, larger-scale datasets are required for further validation in the future. The population only involved individuals of European ancestry, and exploration of ethnic discrepancies could be conducted if data are available. Additionally, while the FinnGen dataset is geographically distinct, residual population stratification still cannot be entirely ruled out to avoid sample overlap issues. Subgroup analyses, including stratifications based on age and sex, could not be performed due to the limitations of the currently available GWAS summary statistics. The current controversy on epidemiological evidence is mainly focused on POAG, and further exploration of other subtypes of glaucoma could be performed.
-
In conclusion, our study suggests a potential causal association of a genetic liability to POAG with schizophrenia, while no evidence of causality for a genetic predisposition to schizophrenia on POAG was identified. The causal associations of a genetic liability to POAG and other psychiatric disorders, including ADHD, anxiety disorder, bipolar disorder, and depressive disorder, were unfounded, indicating that the previously observed correlations might be affected by potential confounding factors. Optimized strategies for their observed comorbidity should be further developed in clinical practice.
-
No ethical approval was required, as this study has been conducted using publicly available and open-access summary statistics, and no human subjects or animals were enrolled.
This study was supported by National Natural Science Foundation of China (U24A20707, 82171075, 82271125, 82301260, and 82301205), Guangdong Basic and Applied Basic Research Foundation (2023B1515120028), China Postdoctoral Science Foundation (2024T170185), Brolucizumab Efficacy and Safety Single-Arm Descriptive Trial in Patients with Persistent Diabetic Macular Edema (2024-29), the launch fund of Guangdong Provincial People's Hospital for NSFC (8227041127). The funders had no role in the study design, data collection, data analysis, data interpretation, or report writing. The authors sincerely thank the funders for their support.
-
The authors confirm their contributions to the paper as follows: study conception and design: Zheng C, Zeng R, Wu G, Hu Y, Yu H; data collection: Zheng C; analysis and interpretation of results: Zheng C, Zeng R; draft manuscript preparation: Zheng C, Zeng R, Wu G; critical revision of the manuscript for important intellectual content: Hu Y, Yu H; manuscript revision: Zheng C, Zeng R, Wu G; funding acquisition: Yu H; administrative, technical, or material support: Hu Y, Yu H. All authors reviewed the results and approved the final version of the manuscript.
-
GWAS summary statistics are available from the original manuscript of each study in Supplementary Table S1 and the GWAS catalog (www.ebi.ac.uk/gwas). All of the codes used in the study are available upon reasonable request from the corresponding author.
-
The authors declare that they have no conflict of interest.
- Supplementary Table S1 Characteristics of data sources used in this study.
- Supplementary Table S2 Assessment of pleiotropy of the Mendelian randomization analysis for the causal effect of psychiatric disorders of interest on primary open-angle glaucoma (POAG).
- Supplementary Table S3 Mendelian randomization analysis for validation of the causal effect of primary open-angle glaucoma (POAG) on schizophrenia.
- Supplementary Table S4 Assessment of pleiotropy of the Mendelian randomization analysis for the causal effect of primary open-angle glaucoma (POAG) on schizophrenia.
- Supplementary Table S5 Mendelian randomization analysis for validation of the causal effect of schizophrenia on primary open-angle glaucoma (POAG).
- Supplementary Table S6 Assessment of pleiotropy of the Mendelian randomization analysis for the causal effect of schizophrenia on primary open-angle glaucoma (POAG).
- Supplementary Fig. S1 Forest plots for the causal effects of primary open-angle glaucoma (POAG) on psychiatric disorders of interest.
- Supplementary Fig. S2 Leave-one-out sensitivity analysis for primary open-angle glaucoma (POAG) on psychiatric disorders of interest.
- Supplementary Fig. S3 Funnel plots for detecting any asymmetry of primary open-angle glaucoma (POAG) on psychiatric disorders of interest.
- Supplementary Fig. S4 Scatter plots for the causal effects of psychiatric disorders of interest on primary open-angle glaucoma (POAG).
- Supplementary Fig. S5 Forest plots for the causal effects of psychiatric disorders of interest on primary open-angle glaucoma (POAG).
- Supplementary Fig. S6 Leave-one-out sensitivity analysis for psychiatric disorders of interest on primary open-angle glaucoma (POAG).
- Supplementary Fig. S7 Funnel plots for detecting any asymmetry of psychiatric disorders of interest on primary open-angle glaucoma (POAG).
- Supplementary Fig. S8 Validation of the causal effect of primary open-angle glaucoma (POAG) on schizophrenia.
- Supplementary Fig. S9 Validation of the causal effect of schizophrenia on primary open-angle glaucoma (POAG).
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Zheng C, Zeng R, Wu G, Hu Y, Yu H. 2025. Investigating causal associations between the genetic liability to primary open-angle glaucoma and psychiatric disorders. Visual Neuroscience 42: e017 doi: 10.48130/vns-0025-0016 

Investigating causal associations between the genetic liability to primary open-angle glaucoma and psychiatric disorders
- Received: 14 January 2025
- Revised: 18 April 2025
- Accepted: 22 July 2025
- Published online: 09 September 2025
Abstract: Current observational evidence on psychiatric diseases and primary open-angle glaucoma (POAG) is controversial. Our study aims to evaluate the putative causal associations between the genetic liability to psychiatric disorders and POAG, and add updated evidence to their linkage. Summary statistics of genome-wide association studies (GWASs) involving 192,702 participants (15,229 cases and 177,473 controls) were used for POAG. Large-scale GWAS summary datasets for psychiatric disorders of interest were also collected. Bi-directional two-sample Mendelian randomization analyses were performed, and sensitivity analyses were conducted to evaluate the robustness of our results. Genetically predicted POAG was causally associated with a slightly increased risk of schizophrenia (odds ratio [OR] = 1.035, 95% confidence interval [CI]: 1.009−1.062, p = 0.008). No evidence of causality was found for POAG and other selected psychiatric disorders (OR = 1.022, 95% CI: 0.988−1.056, p = 0.214 for attention deficit hyperactivity disorder; OR = 1.016, 95% CI: 0.984−1.049, p = 0.325 for anxiety disorder; OR = 1.040, 95% CI: 0.987−1.097, p = 0.143 for bipolar disorder; OR = 0.992, 95% CI: 0.967−1.017, p = 0.526 for depressive disorder) and vice versa. Our findings indicate the mild causal effect of a genetic predisposition to POAG on schizophrenia, and the effects on other psychiatric disorders are not significant. Optimized strategies for their observed comorbidity should be further developed in clinical practice.
-
Key words:
- Glaucoma /
- Psychiatric disorder /
- Genome-wide association study /
- Causal association