








-
Pulmonary arterial hypertension (PAH) is a progressive, fatal vascular disorder marked by remodeling of small pulmonary arteries (PAs), mainly caused by hyperproliferation of pulmonary arterial smooth muscle cells (PASMCs) in the tunica media and a mesenchymal-like transition of pulmonary arterial endothelial cells (PAECs) in the tunica intima[1]. Over three decades, PAH's global incidence and mortality increased by 85.6% and 48.36%, respectively[2,3]. PAH's prevalence and mortality are 2.28 and 0.27 cases per 100,000 person-years, respectively, and the survival rates at 1, 2 and 3 years are 92%, 84%, and 79%[4,5]. Clinical drugs include endothelin receptor blockers, phosphodiesterase-5 (PDE-5) inhibitors, and prostacyclin analogs[6]. Treprostinil (TRE), a common prostacyclin analog, targets the prostacyclin receptors (IP receptors) on PASMCs and promotes the phosphorylation Smad1/5 and upregulation of DNA-binding inhibitory protein 1 in a cyclic adenosine monophosphate (cAMP)-dependent manner, inhibiting PASMCs' proliferation[7]. Because of its vasodilatory effects, TRE is used for severe or rapidly progressing disease. European Society of Cardiology/European Respiratory Society (ESC/ERS) guidelines for the diagnosis and treatment of PAH indicate the main clinical sign of severe PAH is World Health Organization Functional Class IV (WHO-FC IV), defined by an inability to perform activity, symptoms like dyspnea and fatigue at rest, and right heart failure[8]. Rapid progression is defined as a multisymptom decline in clinical, hemodynamic, or functional status over a short period. Both rely on WHO-FC and status changes to guide intervention strategies[9].
However, TRE requires continuous subcutaneous (SC) or intravenous (IV) infusion with external or implanted pump systems, burdening patients and physicians and decreasing adherence[10]. SC infusion causes site pain, reducing tolerability; IV infusion may induce life-threatening catheter-associated IV infections[11,12]. Moreover, pump management is complex, especially with external delivery[13,14]. Maintaining therapy demands managing the settings, ensuring sterility, diluting the medication, and refilling the pumps at intervals. Treatment must be provided at specialized centers by trained staff, limiting accessibility[15,16]. Additionally, pump systems also increase the cost of TRE. Risks and complications affect physicians' willingness to apply parenteral TRE therapy[17]. Thus, a new dosage form is needed to reduce the burden of pump delivery and improve compliance.
Drug microcrystals or microparticles, from nanoscale to micrometer-scale, are simple aggregates that can have a high drug load with controlled release through slow dissolution, making them suitable for sustained-release depots[18−20]. However, direct injection causes a burst release, abrupt changes in the plasma concentration, and adverse effects[21]. Hydrogels, three-dimensional crosslinked networks, restrict diffusion, reduce burst releases, and extend the duration of drug release[22]. Thermosensitive hydrogels transition from a sol to a gel with changes in physiological temperature, allowing minimally invasive administration and in situ depot formation. Methylcellulose (MC) is widely used, as it rapidly forms stable gels at physiological temperatures, and it is regulated by salts, sugars, or copolymers[23]. Drug microparticles in hydrogels form a stable depot after injection[24,25], limiting burst release and prolonging drug release[26−28].
In this study, we developed an injectable in situ-forming TRE depot (TRE-MPs-Gel) with an extended vasodilation response by loading pure TRE microparticles (TRE-MPs) into a thermosensitive hydrogel. An intramuscular (IM) injection of the formulation allowed rapid transitions to an in situ gel depot, reducing the initial burst release. A single injection maintained stable plasma drug concentrations, demonstrated a 3- to 4-d reduction in mean pulmonary arterial pressure (mPAP), and ameliorated disease progression. TRE-MPs-Gel represents a promising strategy to improve TRE therapy by avoiding pump delivery and the burdens associated with its administration, demonstrating translational potential as a long-acting, user-friendly therapeutic approach to enhance the clinical management of PAH, as shown in Fig. 1.
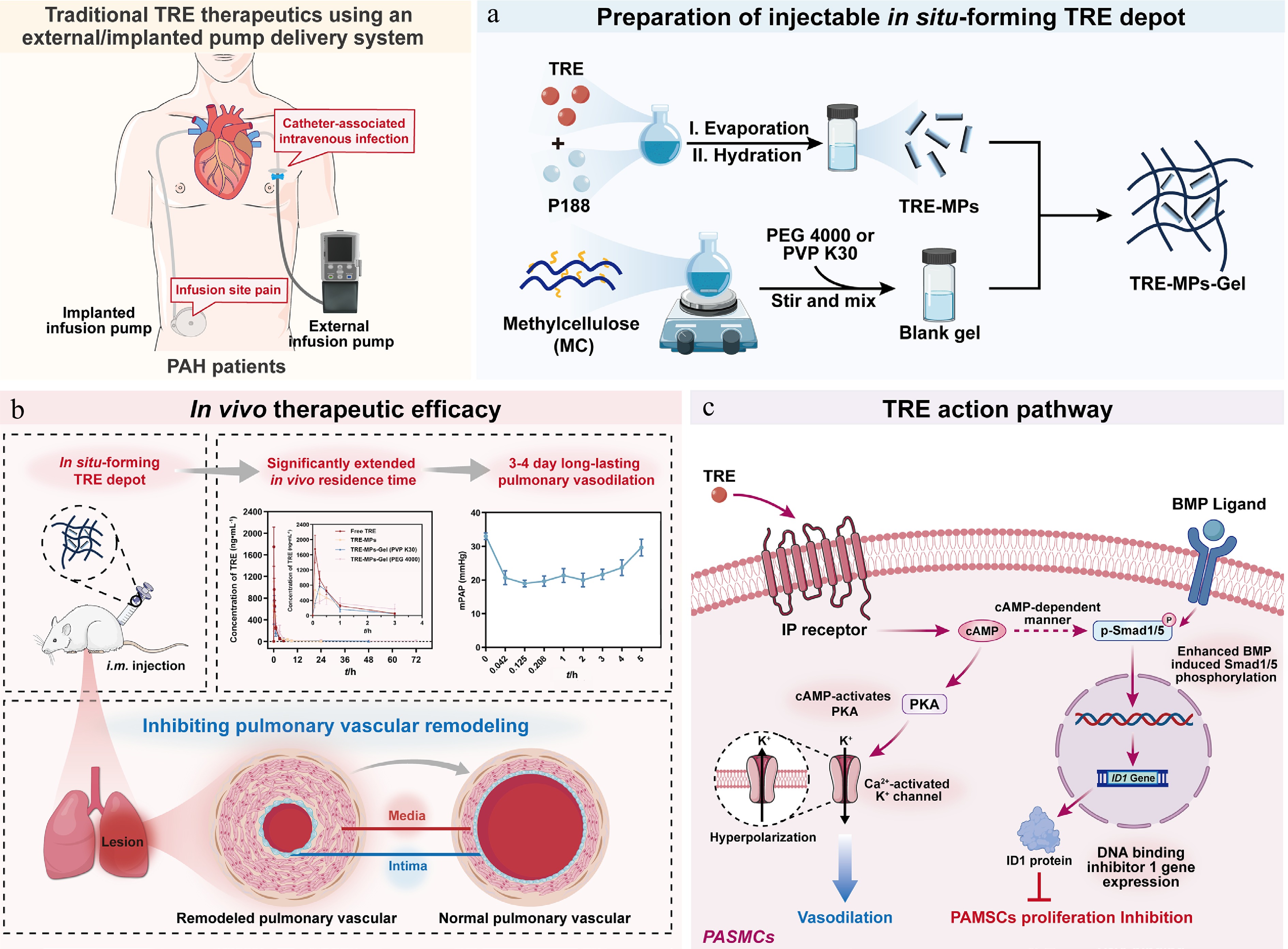
Figure 1.
(a) Preparation of injectable in situ-forming TRE depot. TRE-MPs were prepared using thin-film hydration and TRE-MPs-Gel was prepared using a simple physical mixing method with Methylcellulose as the thermosensitive gel matrix. (b) In vivo therapeutic efficacy. TRE-MPs-Gel, administered via intramuscular injection, forms an in situ gel depot, significantly extending in vivo residence time and enabling 3−4 d long-lasting pulmonary vasodilation for the treatment of pulmonary arterial hypertension. (c) The action pathway of TRE. TRE targets IP receptors on PASMCs, activating PKA and promoting both Smad1/5 phosphorylation and the upregulation of DNA-binding inhibitory protein 1 in a cAMP-dependent manner, via which induces vasodilation and inhibits PASMCs proliferation.
-
Polyvinylpyrrolidone K30 (PVP K30) was purchased from Steckredemeler (Chongqing, China). Monocrotaline (MCT), polyethylene glycol 4000 (PEG 4000), and hyaluronic acid (HA) were obtained from McLean (Shanghai, China). TRE was purchased from Biochempartner (Shanghai, China). Poloxamer 188 (P188) and Poloxamer 407 (P407) were purchased from Wuhan New Land Environmental Protection Materials (Wuhan, China). Thiazolyl blue tetrazolium bromide (MTT) was provided by Shanghai Aladdin Reagent (Shanghai, China). Methylcellulose 4000 cP (MC) was procured from Beyotime Biotechnology (Shanghai, China). Tween 20 and Tween 80 were obtained from Nanjing Chemical Instrument Reagent (Nanjing, China). Bovine serum albumin (BSA) was purchased from Sigma-Aldrich (Missouri, USA). Cy5.5-COOH was obtained from Guangzhou Weihua Biotechnology (Guangzhou, China). The Ki67 monoclonal antibody was purchased from Proteintech (Wuhan, China), and the α-smooth muscle actin (α-SMA) monoclonal antibody was purchased from Abcam (Shanghai, China).
Preparation of TRE-MPs
-
TRE-MPs were prepared using two distinct methods: the antisolvent precipitation–ultrasonication method and the thin-film hydration method[29]. First, TRE-MPs were prepared using the antisolvent precipitation–ultrasonication method. For this, 4 mg of TRE was dissolved in 200 μL of acetone to obtain the organic phase. Then antisolvent solutions of PEG 4000, PVP K30, Tween 80, and Tween 20 were prepared at 1% (W/V). The organic phase was rapidly added to the countersolvent in an ice-water bath. After precipitation of the countersolvent, the suspension was immediately sonicated with an ultrasonic probe sonicator (SCIENTZ-IID, Ningbo Scientz Biotechnology Co., Ltd.) at 100 W for 5 min.
To facilitate a comparison of the methods, the thin-film hydration method was also used , as previously reported[30,31]. TRE and different stabilizers (PVP K30, Tween 80, P188, P407) were codissolved in anhydrous ethanol at a mass ratio of 1 : 3, then evaporated under reduced pressure at 40 °C and 100 rpm for 30 min. The samples were then left to dry at 37 °C for 6 h to remove trace solvents. After further hydration at 37 °C for 1 h, TRE-MPs were obtained by dispersing the samples using an ultrasonic probe sonicator at 100 W for 5 min. TRE-MPs with different mass ratios of TRE to P188 (1 : 2, 1 : 3, and 1 : 4) were prepared using the same method, and samples were either freeze-dried or stored at 4 °C for 24 h.
Preparation and characterization of TRE-MPs-Gel
-
TRE-MPs-Gel was prepared by first dispersing a specified amount of MC in water at 70 °C with stirring until uniform dispersion was achieved. Subsequently, cold water was added with thorough mixing to dilute the mixture, which was then stored at 4 °C for 48 h[32]. The blank gel solution was then incorporated into the freeze-dried TRE-MPs powder, yielding a homogeneous dispersion of TRE-MPs-Gel. The morphological characteristics of the hydrogel were examined using scanning electron microscopy (SEM) (SIGMA HD SEM, Zeiss, Germany).
Determination of gelation temperature and gelation time
-
The gelation temperature and gelation time of the hydrogel were assessed using the inverted test tube method. The hydrogel solution was placed in a constant-temperature water bath (25–60 °C) and gradually heated at a rate of 0.5 °C·min–1. If the substance in the tube remained stationary for 30 s without flowing, the corresponding temperature was taken as the sol–gel transition temperature. Additionally, the hydrogel solution was placed in a constant-temperature water bath at 25 °C for 10 min, then quickly transferred to a constant-temperature water bath at 37 °C. The solution was inverted every 30 s to monitor flowability, and the time to cessation of flow was taken as the gelation time.
Rheological properties of the blank hydrogel
-
The rheological properties of the blank hydrogel were evaluated using an oscillatory rheometer (MCR102e Anton Paar). First, the linear viscoelastic region (LVR) was determined. Then the storage modulus (G') and loss modulus (G'') of the sample were measured as a function of temperature. The temperature at the intersection of G' and G'' was the gelation temperature of the sample. The settings were as follows: angular frequency, 1 rad·s–1; strain, 3.2%; temperature range, 10–40 °C; heating rate, 2 °C·min–1; plate spacing, 0.104 mm.
In vitro degradation behavior of hydrogels
-
The weight method was used to investigate the in vitro degradation behavior of the hydrogel[33]. After allowing the hydrogel solution to stand at 37 °C for 10 min to form a gel, 1 mL of PBS was added, and the mixture was placed in a constant-temperature shaker (100 r·min–1, 37 °C). At predetermined time points, the supernatant was removed, and the remaining gel was weighed. Fresh medium was then added to the initial volume. This process was repeated until the hydrogel was completely hydrolyzed. The remaining gel weight (%) was calculated using Eq. (1):
$ \text{Remaining gel weight}\;({\text{%}})=\dfrac{{W}_{t}}{{W}_{0}}\times 100{\text{%}} $ (1) where, Wt and W0 represent the gel weight at different time points and the initial gel weight, respectively.
In vitro release behavior of hydrogels
-
The in vitro release behavior of free TRE, TRE-MPs, and TRE-MPs-Gel was evaluated using dynamic membrane dialysis. A PBS buffer solution (pH 7.2, containing 0.5% sodium dodecyl sulfate [SDS]) was prepared as the release medium, following previously reported methods[34]. Briefly, each formulation containing 1.6 mg of TRE was placed in dialysis bags (molecular weight cut off [MWCO], 3,500 Da) and incubated in 30 mL of the release medium at 37 °C in a water bath with a constant temperature and shaking (100 r·min–1). At predetermined time points, the release medium was removed and immediately replenished with an equal amount of fresh release medium. TRE content was determined by high-performance liquid chromatography (HPLC), and the cumulative release rate was calculated.
Cell culture
-
Normal pulmonary arterial smooth muscle cells (N-PASMCs) were isolated from the pulmonary arteries of healthy Sprague–Dawley rats. Pulmonary arterial hypertension-associated pulmonary arterial smooth muscle cells (PAH-PASMCs) were extracted from rats with PAH induced by MCT. Cells were cultured in Roswell Park Memorial Institute 1640 (RPMI 1640) medium (Solarbio Life Sciences, Beijing, China) supplemented with 10% fetal bovine serum (FBS) and 100 U·min–1 penicillin + 100 μg·min–1 streptomycin at 37 °C in a 5% CO2 humidified incubator. Cells were detached by trypsin and centrifuged at 1,000 r·min–1 for 3 min. All experiments were conducted during the third and fifth passages.
Cell experiments
-
For the investigation of the cytotoxicity of TRE on N-PASMCs and PAH-PASMCs, the MTT assay was used. Log-phase PAH-PASMCs and N-PASMCs were cultured in a 96-well plate (5 × 103 cells/well) for 24 h at 37 °C. Subsequently, complete TRE medium at different concentrations (10–400 μg·mL–1) was added and cultured for 24 h. Then 20 μL of the MTT solution (5 mg·mL–1) was added, and the mixture was incubated in the dark for 4 h. Dimethyl sulfoxide (DMSO) was added, and the mixture was gently shaken to ensure complete dissolution of the methylene blue crystals. The absorbance (Abs) at 570 nm was measured using a microplate reader. Cell viability was calculated using Eq. (2):
$ \text{Cell viability} \;({\text{%}}) =\dfrac{{\text{Abs}}\,\left( \text{Treated}\right)- {\text{Abs}} \, ({\text {Blank}})}{\text{Abs}\left( \text{Untreated}\right)- \text{Abs (Blank)}} \times 100{\text{%}} $ (2) where, Abs (Treated), Abs (Untreated), and Abs (Blank) represent the absorbance values for the test, control, and blank wells, respectively.
Additionally, for investigating the cytotoxicity of different formulations on PAH-PASMCs, cells were coincubated with 200 μL of the TRE solution, the TRE-MPs solution, and the TRE-MPs-Gel 24-h extract at different concentrations (10–400 μg·mL–1) (see the Supplementary Text 1). According to the aforementioned method, the long-acting inhibitory effect of TRE-MPs-Gel on PAH-PASMCs' proliferation was evaluated.
Finally, to study the cellular biocompatibility of blank gel extracts at different extraction times, PAH-PASMCs and N-PASMCs were coincubated with blank hydrogel extracts for 24, 48, and 72 h at 37 °C, and cytotoxicity was determined using the aforementioned method.
Animals and the establishment of PAH models
-
The specific pathogen free (SPF)-grade Sprague–Dawley rats (male, weighing 280–300 g, 8–10 weeks old) used in the experiment were purchased from Jiangsu Qinglongshan Biotechnology (Zhenjiang, China). The animals used in all experiments followed the Regulations on the Management of Laboratory Animals and the Jiangsu Province Measures for the Management of Laboratory Animals, as well as the China Pharmaceutical University Institutional Animal Care and Use Committee (No. 202407033). Rats were housed in an SPF environment. The MCT model was induced by a single SC injection of MCT solution (60 mg·kg–1)[35] and the animals were randomly assigned 21 d after modeling. Untreated rats, used as negative controls, were subcutaneously injected with an equal volume of saline.
Pharmacokinetic and residence time studies
-
Pharmacokinetic studies were conducted following IM injection of free TRE, TRE-MPs, TRE-MPs-Gel (PEG 4000), or TRE-MPs-Gel (PVP K30) into the right hindlimb muscles of rats at a TRE dosage of 0.8 mg·kg–1. At predetermined time points, blood was collected via orbital sinus puncture and centrifuged at 3,000 r·min–1 for 15 min to obtain plasma. The plasma concentration of TRE was determined by triple quadrupole liquid chromatography–mass spectrometry (LC-MS/MS). Briefly, after precipitation of the plasma protein with acetonitrile, chromatographic separation was performed on a C18 column (50 mm × 2.1 mm, 3 μm) using an acetonitrile–0.1% formic acid mixture as the mobile phase, with a flow rate of 0.5 mL·min–1 at 35 °C, and detected in negative-ion mode via electrospray ionization (see the Supplementary Text 1). Pharmacokinetic parameters were calculated using the noncompartmental, nonoral model in PKSolver software.
To assess the in vivo residence time of the formulations, a previously reported method was used[36]. Rats were treated with a single IM injection of Cy5.5 fluorescent formulations of free TRE, TRE-MPs, TRE-MPs-Gel (PVP K30), or TRE-MPs-Gel (PEG 4000) at a TRE dosage of 0.8 mg·kg–1, and the image of the treated site was measured at predetermined time points using a small-animal in vivo imaging system. Cy5.5 fluorescence intensity in muscle tissue was quantified using a Tanon System with excitation at 700 nm and emission at 730 nm.
Open-chest hemodynamic and right ventricular hypertrophy measurements
-
PA hemodynamic parameters were measured via open-chest surgery[29]. A microcatheter was inserted into the right ventricle and slowly advanced into the PA after it was filled with heparinized saline and connected to a pressure sensor. The microcatheter position was adjusted and confirmed by the monitor waveform, and the mPAP was recorded. After pressure measurement, the rats were sacrificed to collect the major organs, which were washed with physiological saline, snap-frozen, and maintained at –80 °C until further analysis.
For the investigation of the long-acting antihypertensive effect of TRE-MPs-Gel on PAH model rats, a single IM injection of TRE-MPs-Gel at a TRE dose of 0.8 mg·kg–1 was administered. The mPAP of the rats was measured at predetermined time points after administration using the same method.
The harvested heart was incised along the junction of the right heart and interventricular septum, dissecting the heart into the right ventricle and left ventricle plus the interventricular septum, and weighed separately to determine the right ventricular hypertrophy index (RVHI), which was calculated using Eq. (3):
$ RVHI\;({\text{%}}) =\dfrac{RV}{LV+S}\times 100{\text{%}} $ (3) where, RV refers to the weight of the right ventricle, and LV + S refers to the weight of the left ventricle and interventricular septum.
Hematoxylin and eosin staining
-
The lung tissues collected from the experimental groups were fixed in 4% paraformaldehyde and embedded in paraffin for histologic evaluation. After sectioning of the tissue using a microtome, the sections (~3 μm) were stained with hematoxylin and eosin (H&E) and examined under a bright-field upright fluorescence microscope (Leica Microsystems, DM-2500, Wetzlar, Germany) to assess the pulmonary vascular morphology and capture images. The thickness of the pulmonary artery media was calculated using Eq. (4):
$ \begin{split}&{\text{Pulmonary artery media thickness}}\; ({\text{%}} ) \\=\;&\dfrac {\text{Outer vascular wall thickness}}{\text {Outer blood vessel diameter}}\times 100{\text{%}} \end{split}$ (4) To assess right ventricular cardiomyocyte hypertrophy, right ventricles from the experimental group were subjected to H&E staining using the same method. Pathological changes in cardiomyocytes were observed under a bright-field upright fluorescence microscope. The average cross-sectional area (CSA) of the cardiomyocytes was measured using ImageJ to evaluate hypertrophy.
Additionally, to assess the tissue safety of TRE-MPs-Gel, a single IM injection at a TRE dose of 0.8 mg·kg–1 was administered, and the rats were sacrificed on Days 3, 7, and 14 post-administration. The muscle tissue at the injection site was removed and stained with H&E using the same method. Observations and photography were performed using a bright-field upright fluorescence microscope.
Immunohistochemistry
-
The paraffin-embedded lung sections (~3 μm) were dewaxed, rehydrated, and incubated in a peroxidase-blocking solution for 10 min at 25 °C to inhibit endogenous peroxidase activity. Next, the slides were blocked with serum for 10 min at room temperature to inhibit nonspecific binding. Subsequently, the tissues were incubated with anti-α-SMA (1 : 200) or anti-Ki67 (1 : 1,000) primary antibodies overnight at 4 °C, washed with PBS, and incubated with biotinylated secondary antibodies for 10 min at 25 °C. The slides were observed and photographed under a bright-field upright fluorescence microscope. The brown areas were considered to be α-SMA- or Ki67-positive.
Assessment of cell apoptosis by TdT-mediated dUTP nick end labeling staining
-
The TdT-mediated dUTP nick end labeling (TUNEL) assay was used to assess the apoptotic rates in paraffin-embedded lung tissue sections. Briefly, the lung tissue sections were digested with proteinase K (20 μg·mL–1), washed with Tris buffered saline (TBS), and then incubated at 37 °C for 1.5 h with a mixture of TdT Labeling Reaction and TdT Enzyme (Servicebio, Wuhan, China) to initiate the terminal labeling reaction. Finally, the slides were examined under a microscope, and cells showing brown granular precipitates in the nucleus, indicative of DNA fragmentation, were considered to be apoptotic (TUNEL-positive).
Statistical analysis
-
All statistical analyses were performed using GraphPad Prism 10 (GraphPad Software Inc., USA). One-way or two-way analysis of variance (ANOVA) was used to assess the statistical significance of differences between groups. All results are presented as means ± standard deviation (SD), and P < 0.05 is considered to be significant.
-
TRE-MPs were prepared using two methods: antisolvent precipitation–ultrasonication and thin-film hydration (Fig. 2a and c). The results indicated that only TRE-MPs stabilized with P188 and prepared by thin-film hydration were approximately 1 μm in size, with uniform size distributions (polydispersity index [PDI] < 0.3) (Fig. 2b and d). Consequently, P188 was selected as the stabilizer for further development of the formulation. We then optimized the formulation by changing the mass ratio of TRE to P188 from 1 : 2 to 1 : 4. All ratios demonstrated favorable particle sizes and PDIs (Fig. 2e). However, stability tests revealed that storage at 4 °C for 24 h caused rapid particle size increases caused by aggregation (Fig. 2f). After freeze-drying, samples with 1 : 2 and 1 : 3 mass ratios exhibited increased particle size, whereas the 1 : 4 ratio maintained its particle size and PDI close to those of freshly prepared samples (Fig. 2g). These results identified a TRE-to-P188 mass ratio of 1 : 4 as optimal for TRE-MPs' stability, and this formulation was selected for further studies.
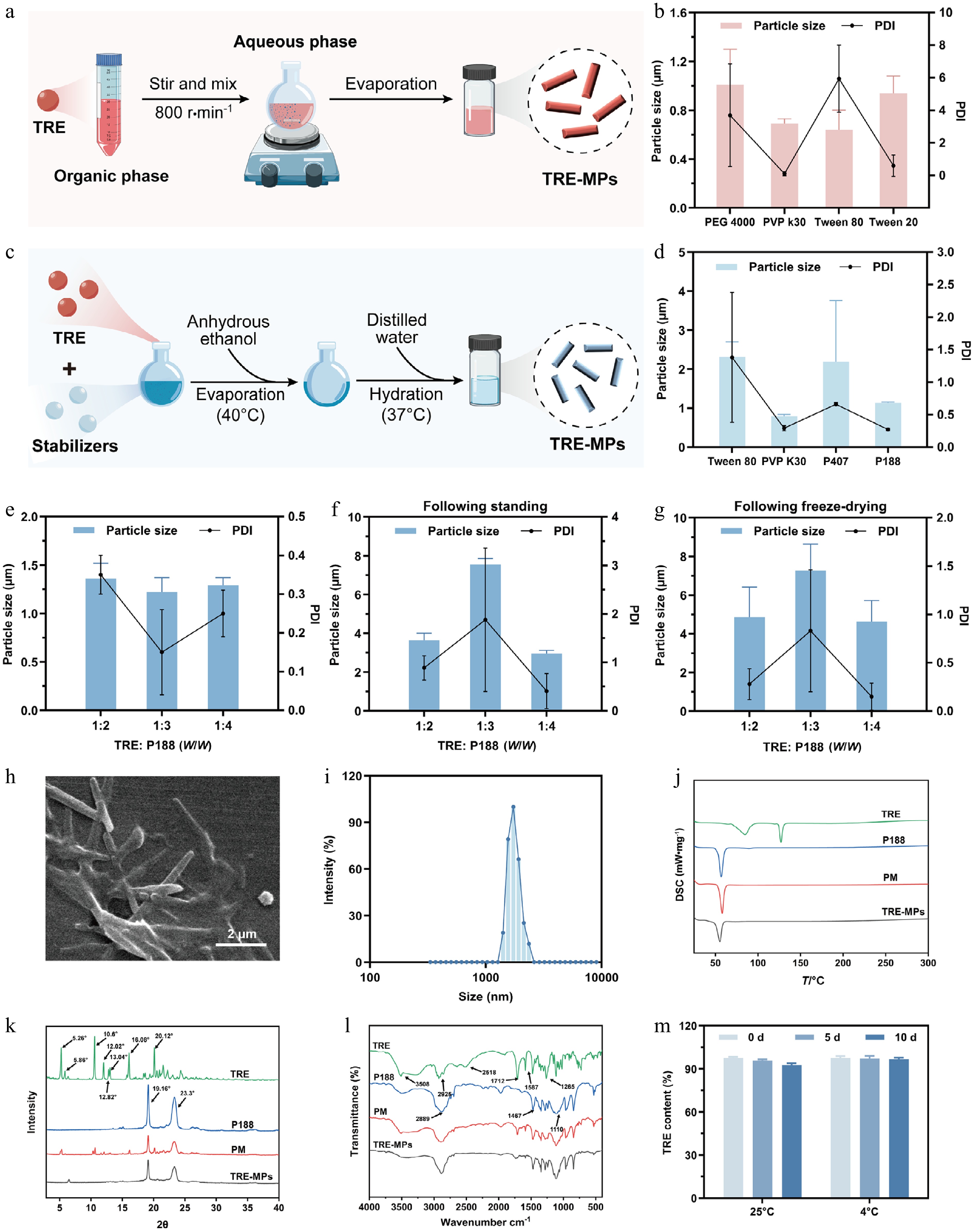
Figure 2.
Preparation and characterization of TRE-MPs. (a) TRE-MPs were prepared by the antisolvent precipitation–ultrasonication method. (b) Particle size and PDI of TRE-MPs prepared by the antisolvent precipitation–ultrasonication method. (c) TRE-MPs were prepared by the thin-film hydration method. (d) Particle size and PDI of TRE-MPs prepared by the thin-film hydration method. (e) Particle size and PDI of TRE-MPs with varying mass ratios of TRE and P188 (1 : 2, 1 : 3, and 1 : 4). (f, g) Particle size stability of TRE-MPs with different TRE: P188 ratios (f) stored at 4 °C and (g) following freeze-drying. (h) SEM image of TRE-MPs. Scale bar: 2 μm. (i) Particle size of TRE-MPs stored at 25 °C. (j) DSC thermograms. (k) PXRD patterns. (l) FTIR spectra of TRE, P188, their physical mixture, and TRE-MPs. (m) The stability of TRE-MPs under different storage conditions. Data are presented as mean ± SD, n = 3.
TRE-MPs displayed a uniform rod-like morphology with a uniform particle size distribution of approximately 1.76 ± 0.04 μm (Fig. 2h and i). Differential scanning calorimetry (DSC) revealed that TRE exhibited sharp endothermic peaks at 73.4 °C and 124.4 °C, and P188 did so at 53.1 °C, indicating the high crystallinity of both substances (Fig. 2j). Physical mixtures (PM) and TRE-MPs showed only the P188 peak (~53 °C), with no endothermic peak for TRE, suggesting that TRE may exist in an amorphous or partially amorphous form. Powder X-ray diffraction (PXRD) patterns confirmed that the TRE in TRE-MPs retained partial crystallinity but with significantly reduced diffraction intensities compared with the raw TRE (Fig. 2k). Collectively, these results indicated that TRE-MPs comprise TRE in a partially crystalline and partially amorphous state. Fourier transform infrared (FTIR) spectroscopy was used to identify the functional groups and intermolecular interactions[37], and showed the disappearance of characteristic TRE peaks at 3,508.45 and 2,518.98 cm–1 in TRE-MPs (Fig. 2l), likely attributable to the hydrogen bonding interactions between TRE and P188, consistent with their chemical structures. Storage stability tests at 4 and 25 °C and light exposure tests demonstrated little change in particle size in TRE-MPs after 10 d. In high-humidity tests, the particle size of TRE-MPs significantly increased with prolonged storage time (Supplementary Fig. S1). It is worth noting that particle size was not measured in the high-temperature and accelerated tests because of partial melting of the freeze-dried TRE-MP samples. This may be attributed to the fact that TRE-MPs exhibit an endothermic peak at 49.6 °C, indicating that their melting point is lower than or close to the test temperature (Fig. 2j). The TRE content remained unchanged during the storage stability tests and under high-humidity conditions, but significantly decreased under high temperature, light exposure, and accelerated degradation (Fig. 2m and Supplementary Fig. S2), emphasizing the sensitivity of TRE-MPs to heat and strong light. Therefore, freeze-dried TRE-MPs should be stored at room temperature or refrigerated (4 °C) to maintain stability.
Preparation and characterization of TRE-MPs-Gel
-
TRE-MPs-Gel was prepared using a simple physical mixing method with MC as the thermosensitive gel matrix (Fig. 3a). Initially, the effects of different additives (NaCl, PVP K30, HA, and PEG 4000) and their concentrations on the gelation temperature of MC were evaluated (Fig. 3b–e). The MC concentration was inversely proportional to gelation temperature because of the increased methoxy content, and viscosity increased with concentration. To ensure injectability, we chose a 1% MC solution for further optimization. Then four hydrophilic additives were tested, with the additive concentration inversely proportional to the gelation temperature. The addition of NaCl reduced the gelation temperature to 38.3, 36.2, and 34.3 °C at 5%, 6%, and 7% concentrations, respectively. To account for injection site safety, we selected a 6% NaCl formulation in 1% MC for subsequent studies.
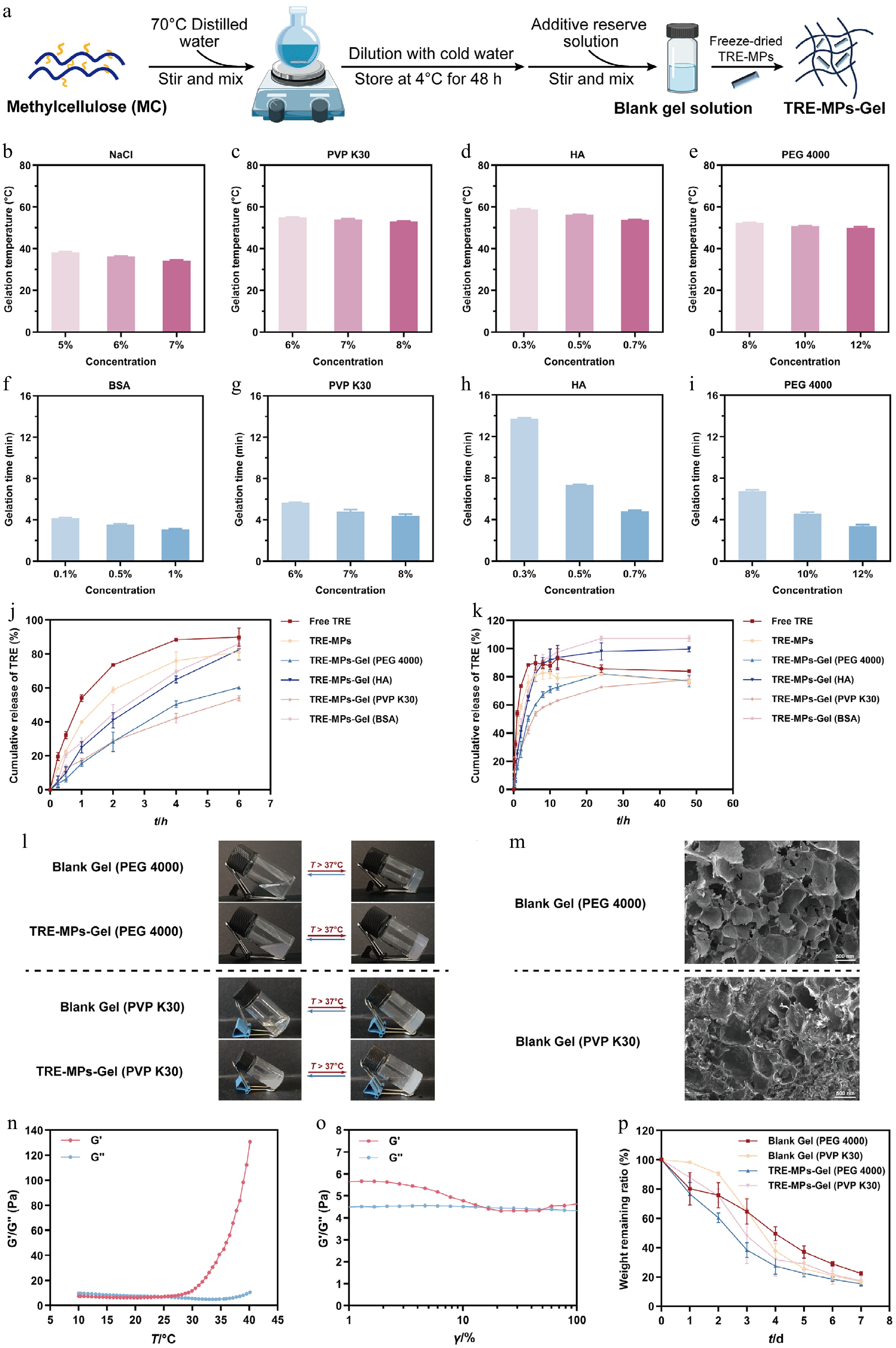
Figure 3.
Optimizing the formulation and characterization of TRE-MPs-Gel. (a) The flowchart for the preparation of TRE-MPs-Gel. (b–e) Gelation temperature of MC hydrogels with varying additive concentrations of (b) NaCl, (c) PVP K30, (d) HA, and (e) PEG 4000. (f–i) Gelation time of MC hydrogels with varying additive concentration of (f) BSA, (g) PVP K30, (h) HA, and (i) PEG 4000. (j, k) In vitro release profiles of free TRE, TRE-MPs, TRE-MPs-Gel (PEG 4000), TRE-MPs-Gel (HA), TRE-MPs-Gel (PVP K30), and TRE-MPs-Gel (BSA) within the (j) first 7 h and (k) 60 h. (l) Sol–gel transition behavior of blank gel and TRE-MPs-Gel. (m) SEM images of blank gel (PEG 4000) and blank gel (PVP K30). Scale bar: 500 μm. (n) Linear viscoelastic region and (o) gelation temperature of blank gel (PEG 4000). (p) In vitro degradation profiles of blank gel and TRE-MPs-Gel. Data are given as the mean ± SD, n = 3.
The impact of the additives and their concentrations on the gelation time was then investigated (Fig. 3f–i). The results showed that higher additive concentrations significantly shortened the gelation time. To minimize drug diffusion through rapid gelation, the following concentrations were selected for further evaluation: 1% BSA, 8% PVP K30, 0.7% HA and 12% PEG 4000. Subsequently, their in vitro release behavior was assessed using dynamic membrane dialysis (Fig. 3j and k). TRE-MPs were released rapidly and equilibrated at 24 h, whereas TRE-MPs-Gel significantly prolonged the release. TRE-MPs-Gel (PEG 4000) and TRE-MPs-Gel (BSA) equilibrated at 24 h with cumulative release rates of 82.0% and 107.2%, whereas TRE-MPs-Gel (HA) and TRE-MPs-Gel (PVP K30) equilibrated at 48 h with 99.5% and 77.9%, respectively. Compared with TRE-MPs, the cumulative release at 0.5 h was reduced by 3.66-, 2.32-, and 1.77-fold for TRE-MPs-Gel (PEG 4000), TRE-MPs-Gel (HA), and TRE-MPs-Gel (PVP K30), respectively, thereby reducing the initial burst release. However, TRE-MPs-Gel (HA) exhibited higher late-stage release, limiting its sustained release potential. Therefore, TRE-MPs-Gel (PEG 4000) and TRE-MPs-Gel (PVP K30) were selected for subsequent studies.
The sol–gel transition behavior was assessed, with both blank gel solutions and TRE-MPs-Gel solutions transforming into an opaque, semisolid state upon heating (Fig. 3l). SEM revealed a three-dimensional porous network in blank gels containing PEG 4000 or PVP K30, with notable structural differences. PEG 4000-based gels had larger, irregular pores and a looser network, whereas PVP K30-based gels featured smaller, uniform pores and a denser structure (Fig. 3m). This network provided a structural foundation for drug storage. Rheological analysis of the blank gel (PEG 4000) determined a linear viscoelastic region (LVR) limit of 3.54% (Fig. 3n), indicating good structural stability under stress[38]. Within the LVR, gelation temperature testing showed that the loss of blank gel (PEG 4000) was investigated at stress levels below 25 °C (Fig. 3o). When the environmental temperature was lower than 25 °C, G'' was higher than G', and the hydrogel behaved as a viscous liquid. With the reverse, gel formation occurred. These findings confirmed that the blank hydrogel can gelate at body temperature, supporting its suitability for in vivo applications.
The in vitro degradation of hydrogels is a critical factor influencing drug release[39,40]. As shown in Fig. 3p, after 7 d, the remaining weights of the PEG 4000 blank gel, the PVP K30 blank gel, TRE-MPs-Gel (PEG 4000), and TRE-MPs-Gel (PVP K30) were 22.43%, 16.77%, 15.30%, and 17.35%, respectively, corresponding to degradation rates of approximately 77.57%, 83.23%, 84.7%, and 82.65%. These variations stemmed from the differential effects of the additives on the in vitro degradation of MC-based thermosensitive hydrogels. Notably, TRE-MPs-Gels degraded faster than the blank gels at all time points, likely through the dissolution of TRE in PBS, which promotes MC's dissociation and accelerates hydrogel erosion.
In vivo fate at the injection site and pharmacokinetic study
-
We evaluated the in vivo residence of TRE-MPs-Gel using fluorescence imaging in healthy rats after IM injection of a preparation containing TRE labeled with the near-infrared fluorescent dye Cy5.5-COOH (Fig. 4a), as previously reported[41−44]. Fluorescence persisted until Days 8, 10, 12, and 15 for free TRE, TRE-MPs, TRE-MPs-Gel (PVP K30), and TRE-MPs-Gel (PEG 4000), respectively (Fig. 4b). Quantitative analysis of fluorescence intensity in the muscle region revealed a rapid decline for free TRE and TRE-MPs, with significant reductions by Day 4 (P < 0.05) and Days 8–10 (P < 0.05), respectively, and complete signal loss by Day 12. In contrast, TRE-MPs-Gel maintained signals until they disappeared on Day 15 (Fig. 4c–j). These results demonstrated that TRE-MPs provide sustained release compared with free TRE, and the gel further extended residence, with TRE-MPs-Gel (PEG 4000) showing the longest in vivo persistence.
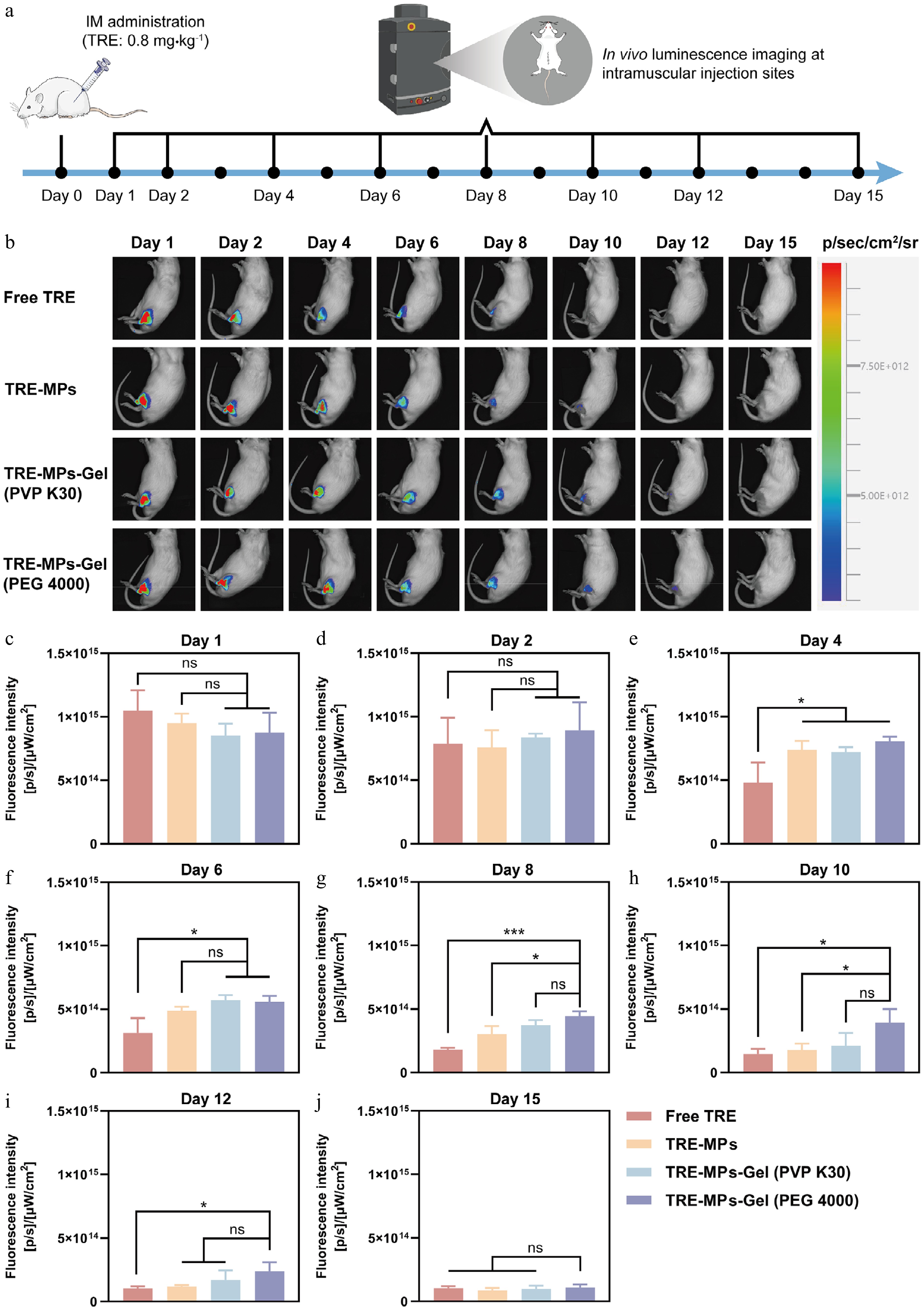
Figure 4.
In vivo residence time study of TRE-MPs-Gel. (a) In vivo residence time study design. The administration site was photographed at predetermined time points after a single dose. (b) Fluorescence intensity at the administration site of TRE-MPs-Gel was measured in the same rat tracked longitudinally at predetermined time points. (c–j) Quantitative fluorescence data at the administration site of TRE-MPs-Gel measured at (c) 1, (d) 2, (e) 4, (f) 6, (g) 8, (h) 10, (i) 12, and (j) 15 d. Data are shown as the mean ± SD, n = 3; * P < 0.05, *** P < 0.001, ns, not significant.
To precisely assess residence and pharmacokinetics, we measured the blood drug concentration of TRE via LC-MS/MS after a single IM injection and constructed a drug concentration–time curve (Fig. 5a). Pharmacokinetic parameters were fitted using PKSolver software[45], as demonstrated in Fig. 5d–j and summarized in Table 1. TRE-MPs-Gel exhibited a flatter curve with a smoother decline in plasma concentration, sustaining levels for 3 d, compared with rapid drops in free TRE and TRE-MPs (Fig. 5b and c). Additionally, TRE-MPs-Gel had a significantly increased half-life (t1/2), area under the curve (AUC), and mean residence time (MRT) while reducing the maximum plasma concentration (Cmax) and the clearance rate (CL), indicating suppression of their burst release and prolonged drug exposure. Specifically, TRE-MPs-Gel (PEG 4000) achieved a t1/2 of 17.96 ± 5.38 h (Fig. 5d), the lowest Cmax (554.68 ± 117.83 ng·mL–1; Fig. 5f), and the highest AUC (1,472.62 ± 152.08 ng·h·mL–1; Fig. 5g) and MRT (23.16 ± 2.64 h, Fig. 5i). As a result, TRE-MPs-Gel (PEG 4000) was selected for subsequent in vivo pharmacodynamic studies.
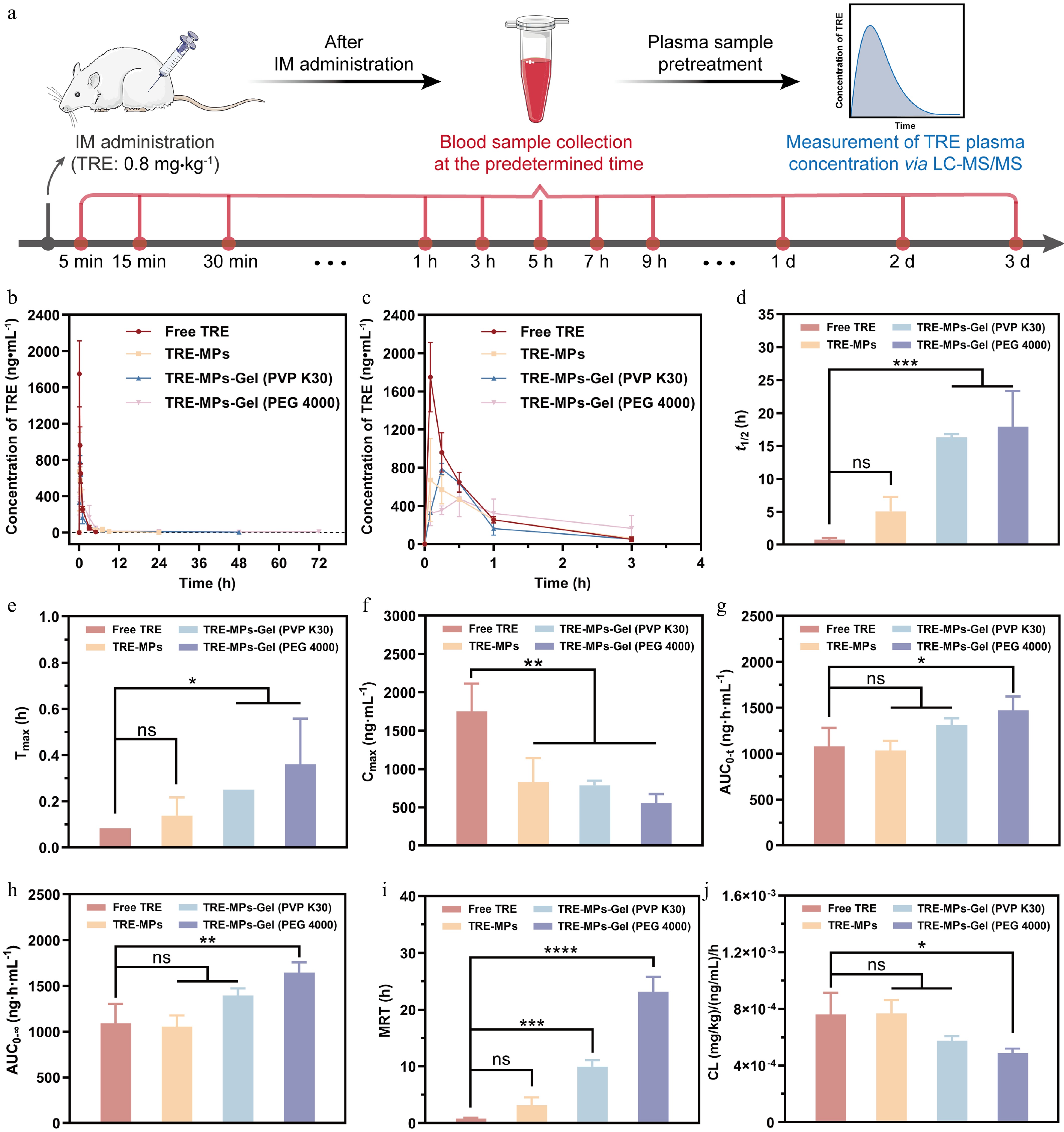
Figure 5.
Pharmacokinetic study. (a) The pharmacokinetic study's design. Blood samples were collected at the predetermined time after a single IM administration, and TRE plasma concentrations were measured by LC-MS/MS. (b, c) Drug concentration–time curve at (b) 72 h and (c) 4 h of TRE-MPs-Gel after a single IM administration at a dose of 0.8 mg·kg–1. (d–j) Main pharmacokinetic parameters of TRE-MPs-Gel including (d) t1/2, (e) time to reach maximum plasma concentration (Tmax), (f) Cmax, (g) AUC0-t, (h), AUC0-∞, (i) MRT, and (j) CL. Data are given as the mean ± SD, n = 3. * P < 0.05, ** P < 0.01, *** P < 0.001, **** P < 0.0001, ns, not significant.
Table 1. Pharmacokinetic parameters of TRE-MPs-Gel after a single IM injection in rats at a TRE dose of 0.8 mg·kg–1.
Formulations t1/2a (h) Tmaxb (h) Cmaxc (ng·mL–1) AUC0-td (ng·h·mL–1) AUC0-∞e (ng·h·mL–1) MRTf (h) CLg (mg·kg–1)·(ng·mL–1)–1·h–1 Free TRE 0.75 ± 0.24 0.083 1,749.57 ± 364.52 1,079.85 ± 200.68 1,092.67 ± 213.17 0.81 ± 0.12 0.0008 ± 0.0002 TRE-MPs 5.04 ± 2.20ns 0.14 ± 0.08ns 825.67 ± 317.14** 1,033.93 ± 105.57ns 1,058.06 ± 120.73ns 3.18 ± 1.33ns 0.0008 ± 0.0001ns TRE-MPs-Gel (PVP K30) 16.29 ± 0.48** 0.25ns 787.19 ± 59.97** 1,313.92 ± 71.23ns 1,393.70 ± 79.55ns 9.97 ± 1.13*** 0.0006 ± 0.00003ns TRE-MPs-Gel (PEG 4000) 17.96 ± 5.38*** 0.36 ± 0.20* 554.68 ± 117.83** 1,472.62 ± 152.08* 1,646.94 ± 110.08* 23.16 ± 2.64**** 0.0005 ± 0.00003* Data are given as the mean ± SD, n = 3. * P < 0.05, ** P < 0.01, *** P < 0.001, compared with the free TRE. ns, not significant. a Elimination half-life of the drug. b Time to reach the maximum plasma concentration. c Maximum plasma concentration. d Area under the concentration–time curve from 0 to t h. e Area under the concentration–time curve from 0 to ∞ h f Mean residence time. g Clearance rate. Therapeutic efficacy
In vivo long-acting inhibition of PASMCs' proliferation -
First, we assessed the cytotoxicity of TRE on N-PASMCs and PAH-PASMCs using the MTT assay. The results showed a concentration-dependent increase in cytotoxicity for both cell types (Supplementary Fig. S3), with PAH-PASMCs exhibiting higher survival rates than N-PASMCs at equivalent TRE concentrations. This was primarily driven by the enhanced proliferative activity of pathological PAH-PASMCs[46]. Their excessive proliferative mainly arose from phenotypic transition and the massive release of inflammatory factors in the pathological microenvironment, ultimately reducing cellular sensitivity to TRE[47,48].
We then assessed the antiproliferative effects of TRE-MPs-Gel on PAH-PASMCs. The cytotoxicity of TRE-MPs, TRE-MPs-Gel (PEG 4000), and TRE-MPs-Gel (PVP K30) was lower than that of free TRE at the same concentration (Supplementary Fig. S4), attributable to the controlled drug release that minimized initial burst effects, as evidenced by the lower short-term (6 h) release in Fig. 3j. These results indicated that TRE-MPs-Gel achieves long-acting inhibition of PAH-PASMCs' proliferation while reducing acute toxicity by delaying drug release, providing an optimized strategy for targeted PAH therapy.
Improved hemodynamics and antipulmonary vascular remodeling
-
In vivo therapeutic efficacy of TRE-MPs-Gel was evaluated in an MCT-induced rat PAH model (Fig. 6a). First, we assessed its therapeutic efficacy by measuring mPAP. Elevated mPAP (> 33 mm Hg, P < 0.0001) is a hallmark of PAH[49]. All formulation groups effectively reduced mPAP to below 25 mm Hg after 14 d of treatment, primarily because of the potent vasodilatory effects of TRE. At the same dosage, TRE-MPs-Gel exhibited more sustained vasodilatory effects and the most significant mPAP-lowering effects (P < 0.0001) (Fig. 6c). Furthermore, we investigated the long-acting antihypertensive effects of low-dose TRE-MPs-Gel (at a TRE dose of 0.8 mg·kg–1) in the MCT-induced rat PAH model (Fig. 6b). The results demonstrated that mPAP decreased from 33 to 21 mm Hg within 1 h of treatment, with a rapid reduction in pulmonary vascular resistance. The antihypertensive effect persisted for 3–4 d, indicating its long-acting efficacy (Fig. 6d).
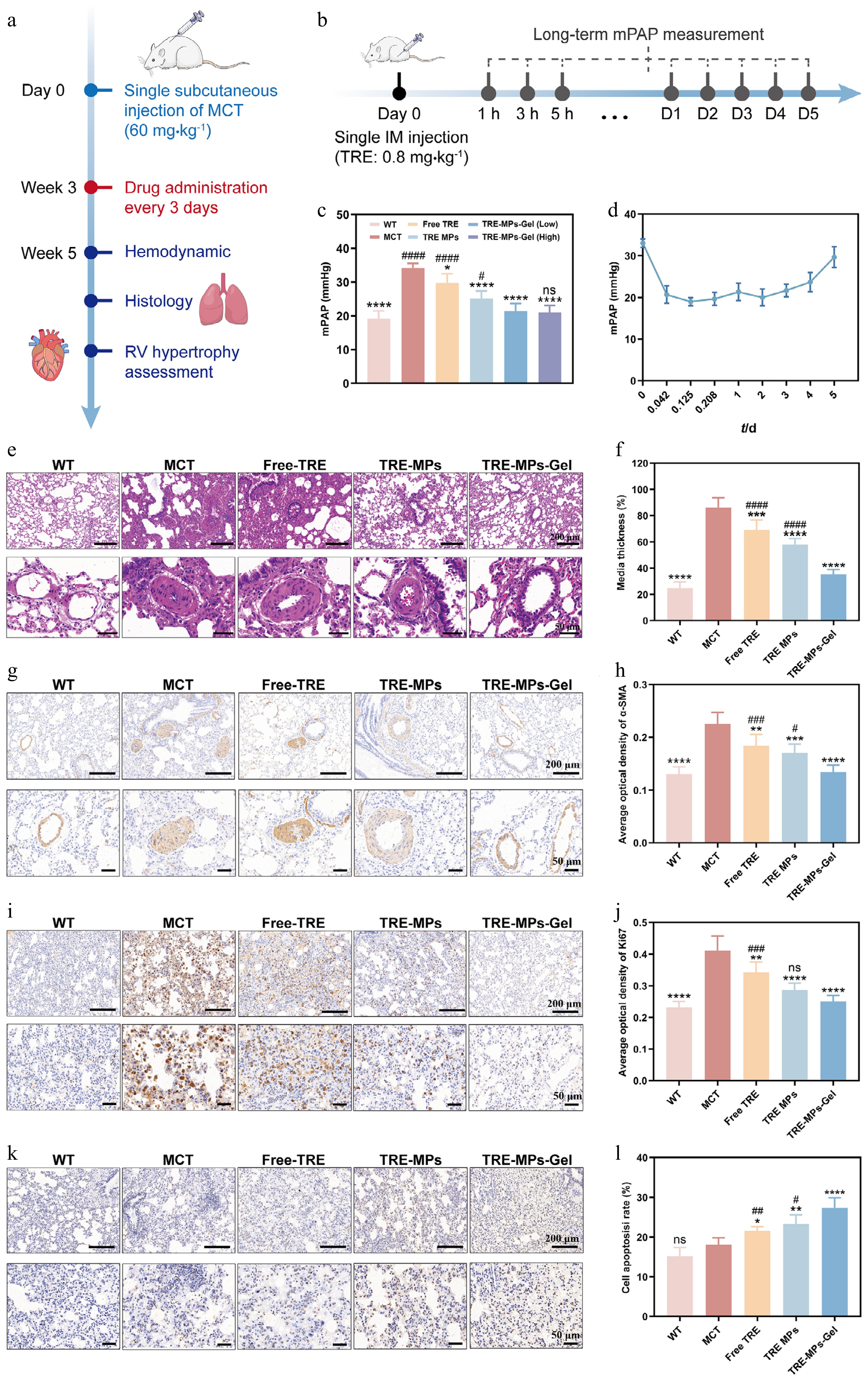
Figure 6.
Therapeutic efficacy in the MCT rat model. TRE-MPs-Gel (PEG 4000) was selected for in vivo pharmacodynamic evaluation. (a) Establishment of the PAH rat model and PAH treatment administration schedule. (b) Long-term mPAP measurement schedule. (c) mPAP in rats after treatment (n = 5). (d) mPAP in rats after a single administration of TRE-MPs-Gel (PEG 4000) at 1, 3, and 5 h and 1, 2, 3, 4, and 5 d (n = 3). (e) H&E staining of lung sections, showing nuclei in blue and cytoplasm/extracellular matrix in red. (f) Semiquantitative analysis of pulmonary medial thickness (n = 5). (g) Representative α-SMA immunohistochemistry (IHC) images and (h) semiquantitative analysis of α-SMA expression in pulmonary vessels (n = 5). (i) Representative Ki67 IHC images and (j) semiquantitative analysis of Ki67's expression in pulmonary vessels (n = 5). (k) TUNEL staining images and (l) semiquantitative analysis of TUNEL-positive cells (n = 5). Brown staining indicates positive areas. Scale bars: 200 and 50 μm. Rats received IM injections of free TRE (0.286 mg·kg–1 once daily), TRE-MPs (0.8 mg·kg–1 once every 3 d), and TRE-MPs-Gel (normal: 0.8 mg·kg–1; high: 1.2 mg·kg–1, once every 3 d) for 2 weeks. Data are presented as the means ± SD. * P < 0.05, ** P < 0.01, *** P < 0.001, **** P < 0.0001 vs. MCT group; # P < 0.05, ## P < 0.01, ### P < 0.001, #### P < 0.0001 vs. TRE-MP-Gel group; ns, not significant.
Next, we evaluated pulmonary vascular remodeling after 14 d of treatment in the MCT-induced rat PAH model. PA wall thickening, a key driver of increased vascular resistance and PAH's progression[50], was evident in the MCT group compared with the untreated controls. The treatment using drug-containing formulation significantly reduced wall thickness (P < 0.001) (Fig. 6e and f). TRE-MPs-Gel treatment enabled the vascular walls to be closest to normal (~35 μm), resulting in 1.96- and 1.65-fold reductions compared with free TRE and TRE-MPs, respectively, indicating its superior therapeutic performance. Moreover, we identified the α-SMA marker to assess PA muscularization. All treatment groups showed a reduction in this marker, especially with TRE-MPs-Gel, emphasizing the ability of the formulations to mitigate vascular remodeling (Fig. 6g and h).
Antiproliferation and proapoptotic effects
-
Excessive proliferation of PASMCs is a key contributor to pulmonary vascular remodeling. Therefore, Ki67 immunohistochemistry was performed to assess PASMCs' proliferation in the lung tissue of rats after treatment (Fig. 6i). Quantitative analysis of the average optical density (AOD) demonstrated that all treatments significantly inhibited PASMCs' proliferation (Fig. 6j, P < 0.01). Notably, the TRE-MPs-Gel group exhibited the most potent antiproliferative effect, restoring proliferation levels to near-normal levels.
Concurrently, apoptosis was evaluated in rat lung tissue after treatment using TUNEL immunohistochemical staining[51]. The apoptotic rate was quantified using ImageJ, with the results shown in Fig. 6k and l. The quantitative findings aligned with the staining observations: Free TRE, TRE-MPs, and TRE-MPs-Gel all significantly promoted apoptosis (P < 0.05), increasing apoptotic rates by 1.20-, 1.29-, and 1.51-fold, respectively, compared with the MCT group. Among these, TRE-MPs-Gel induced the highest level of apoptosis, demonstrating the strongest proapoptotic activity.
Overall, TRE-MPs-Gel significantly downregulated α-SMA's expression, inhibited PASMCs' proliferation, and enhanced apoptosis, thereby significantly inhibiting pulmonary vascular remodeling and alleviating PA occlusion.
Anti-right ventricular remodeling
-
Compared with the untreated group, RVHI was significantly elevated in the MCT group, whereas it was reduced in all the treatment groups (Supplementary Fig. S5). Notably, the TRE-MPs-Gel (high) group displayed the lowest RVHI value (P < 0.01), approaching that of normal rats (~0.23), indicating effectiveness against right ventricular hypertrophy. H&E staining also indicated that TRE-MPs-Gel treatment effectively ameliorated hypertrophy (Supplementary Fig. S6), with a cardiomyocyte morphology most closely resembling that of the untreated group. Quantitative analysis revealed that the CSA was significantly larger in the MCT group than in the untreated group, and was reduced in all treatment groups compared with the MCT group (P < 0.01). Further comparison revealed that the CSA in the TRE-MPs-Gel group was the lowest among all the treatment groups, being 1.89-fold and 1.60-fold lower than in the free TRE and TRE-MPs groups, respectively. This highlighted the enhanced efficacy of TRE-MPs-Gel in inhibiting right ventricular myocardial hypertrophy. Collectively, these data suggested that TRE can attenuate and reverse the pathological process of right ventricular remodeling by inhibiting right ventricular myocardial cell hypertrophy, with the TRE-MPs-Gel showing the most prominent effect.
Safety evaluation
-
The MTT assay was used to evaluate the biocompatibility of blank gel extracts at different extraction times. With complete medium as the control, cell survival decreased with increasing incubation time, suggesting a gradual increase in the extracts' cytotoxicity. Further analysis revealed that the survival rate of cells exposed to blank hydrogel extracts declined slightly with prolonged extraction time. Notably, the PEG 4000 blank gel group exhibited higher survival rates than the PVP K30 blank gel group. Importantly, the cell survival rate in the PEG 4000 blank gel was higher than that in the PVP K30 blank gel, indicating better cellular compatibility (Fig. 7a and b).
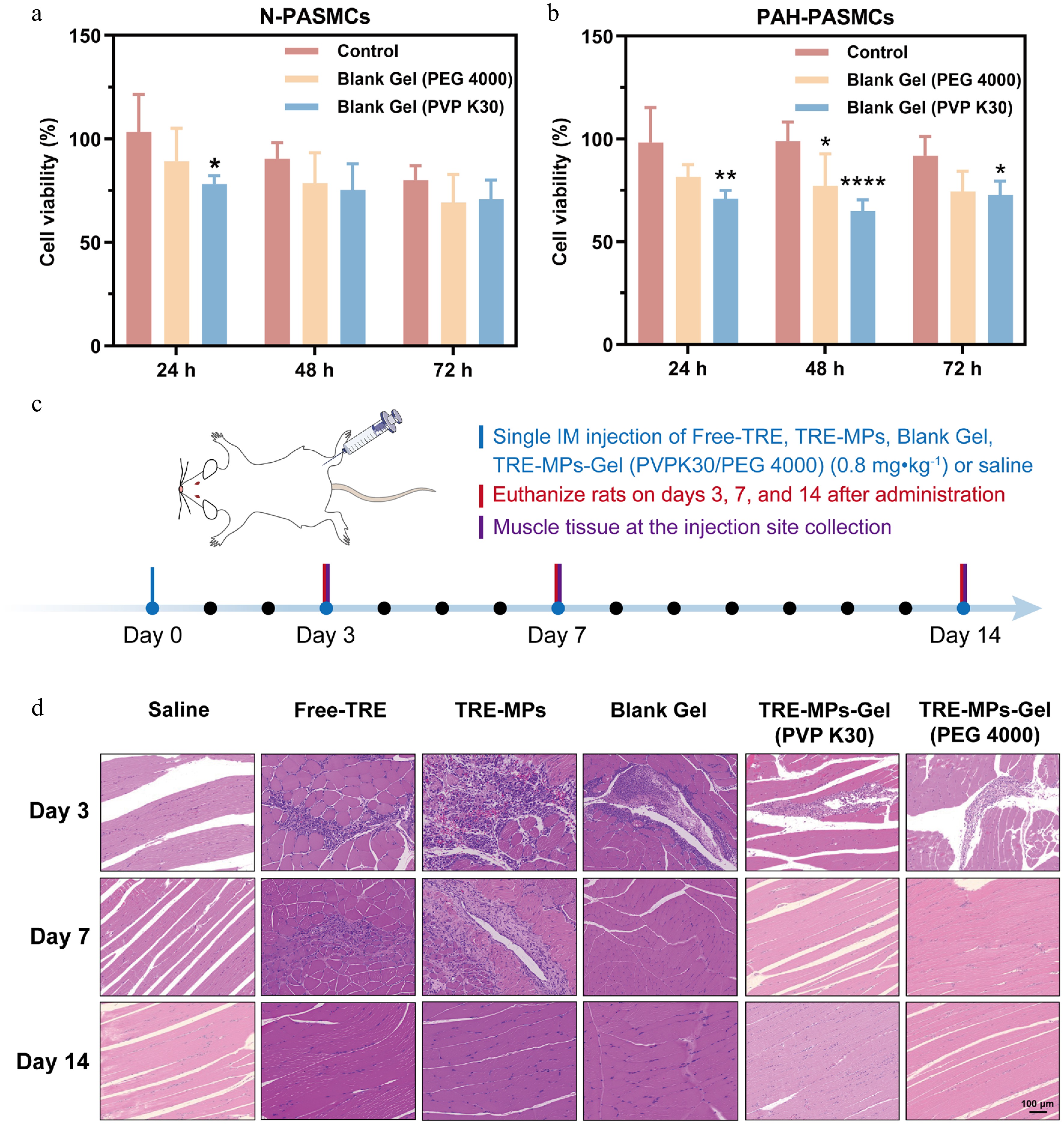
Figure 7.
Safety evaluation of TRE-MPs-Gel (a, b) Cytotoxicity evaluation of blank gel (PEG 4000) and blank gel (PVP K30) on (a) N-PASMCs and (b) PAH-PASMCs (n = 6). (c) Safety evaluation at the injection sites. Muscle tissue was collected on Days 3, 7, and 14 after a single IM administration of free TRE, TRE-MPs, blank gel, TRE-MPs-Gel (PEG 4000), TRE-MPs-Gel (PVP K30) or saline. (d) H&E staining of paraffin-embedded rat muscle sections. Scale bars: 200 μm. Data are given as the mean ± SD. * P < 0.05, ** P < 0.01, **** P < 0.0001 vs. control group.
We then we evaluated the injection site safety of TRE-MPs-Gel (Fig. 7c). At 3 d post-treatment, local inflammatory cell infiltration was observed in all formulation-treated groups, with the most severe neutrophil and inflammatory cell infiltration in TRE-MP group. On Day 7, inflammation persisted in the free TRE and TRE-MP group, whereas it had completely disappeared in the blank gel, TRE-MPs-Gel (PVP K30), and TRE-MPs-Gel (PEG 4000) groups. By Day 14, little difference was observed between the formulation-treated and saline-treated muscle sections, indicating that this local inflammatory response was transient and reversible (Fig. 7d).
Overall, these results indicated that the acute inflammatory response induced by TRE-MPs-Gel at the injection site was transient and reversible, confirming that TRE-MPs-Gel meets the local safety standards for long-acting injectables, providing a strong foundation for further preclinical development.
-
PAH, as a progressive and fatal vascular disease, faces significant challenges in its long-term management. Although TRE is a first-line drug for treating PAH, its clinical application remains limited by pain at the SC injection site and catheter-associated IV infection associated with SC/IV administration via external/implantable pump delivery systems. These associated risks and complications ultimately become key barriers to patients' medication adherence. Hydrogel-encapsulated drug microparticles form a stable drug depot after injection, effectively inhibiting the burst release and prolonging drug delivery[24]. Inspired by this, this study developed a novel in situ-forming drug depot (TRE-MPs-Gel) based on drug microparticles and thermosensitive hydrogel technology. By preparing morphologically stable rod-shaped TRE-MPs stabilized with P188 via thin-film hydration and then combined with an optimized MC/PEG 4000 thermosensitive hydrogel to form TRE-MPs-Gel, the optimal formulation rapidly transformed into a gel at body temperature, forming a TRE depot. Through a synergistic sustained release mechanism, TRE-MPs-Gel extended the TRE dosing interval from 24 h to 3 d while addressing critical shortcomings of traditional formulations, such as low drug loading capacity and an uncontrolled initial burst release, offering a highly efficient, safe, and convenient therapeutic solution for PAH treatment.
The sustained release effect of TRE-MPs-Gel was primarily attributed to the dual-release mechanism of the microsized drug particles and thermosensitive hydrogels. First, the sustained release of drug particles was primarily driven by particle size. With a larger particle size and a smaller specific surface area, particles exhibited relatively low dissolution rates[52,53]. Preparing TRE as microsized hydrophobic particles enabled high drug loading efficiency (~97%), and the slow dissolution of microparticles provided primary regulation for the sustained delivery of TRE. Second, encapsulating TRE-MPs within a thermosensitive hydrogel created a secondary barrier. In our study, MC was selected as the thermosensitive gel matrix because of its widespread use as an in situ gelling polymer, offering biocompatibility, low cost, and injectability even at low temperatures. Importantly, the gelation behavior of MC can be easily modulated by adding additives such as salts, sugars, or polymers[54]. Although other polymers (such as hyaluronic acid and poloxamer) can also form hydrogels, they often suffer from drawbacks, including nonbiodegradability, rapid dissolution, and low mechanical strength[55]. To overcome these limitations, hydrogel materials typically require modification by physical cross-linking or chemical modification, thereby restricting their clinical applications[56]. Gel formation correlated with exposed hydrophobic methoxy groups and enhanced hydrophobic interactions[57]. The hydrogel rapidly responded to body temperature after IM injection, and the hydrogen bonds between MC and water molecules broke, exposing methoxy groups that progressively increased hydrophobic interactions, forming a three-dimensional hydrogel network that restricted drug diffusion at the injection site and minimized burst release[23, 54]. In vitro release data further confirmed this synergistic effect: A comparative analysis demonstrated that the microparticles–thermosensitive gel composite system reduced burst release by 3.66-fold compared with TRE-MPs alone, thereby achieving secondary regulation for sustained delivery of TRE.
Compared with previously reported sustained release formulations such as prodrugs, implants and microspheres, which suffered from complex preparation processes, surgical intervention requirements, and low drug loading[24, 58−60], the TRE-MPs-Gel developed in this study encapsulated TRE-MPs by simply adding a blank gel solution to freeze-dried microparticle samples and stirring until the microparticles were uniformly dispersed. For instance, CAM2043 is reported to be a long-acting TRE SC injection formulation in development, based on Camurus' FluidCrystal® sustained-release injection technology[61]. Comparative analysis suggested that those TRE-MPs consisted solely of the drug and stabilizer (P188) at an optimal mass ratio (1 : 4), containing no organic solvents. The simplified, safe preparation process, high drug-loading capacity, minimally invasive administration, low cost, and ease of industrial-scale production enabled the formulation to effectively address the delivery challenges of hydrophobic drugs like TRE for chronic disease treatment, demonstrating significant potential for clinical translation. The optimal physicochemical properties translated to enhanced in vivo performance. The optimal formulation formed an in situ drug depot after IM injection that significantly prolonged the drug's residence time (15 d), far exceeding the 8-d and 10-d residence times of TRE and TRE-MPs, respectively. TRE-MPs exhibited sustained release effects, whereas the gel further extended the duration of release time of the microparticles. Additionally, the optimal formulation demonstrated excellent pharmacokinetic properties, such as a plasma half-life of 18 h, whereas TRE and TRE-MPs maintained their efficacy for only 3 and 24 h, respectively. The stable plasma concentration curve of TRE-MPs-Gel supported a 3-d dosing regimen while reducing the systemic side effects caused by concentration fluctuations, thereby enhancing safety.
Notably, the in vitro depot release time was shorter than the in vivo residence time at the injection site. This discrepancy may be attributed to the controlled conditions of in vitro release studies, which cannot fully replicate the complexity of the in vivo environment[62]. For instance, Yanev et al. developed a thermosensitive hydrogel based on thiolated hyaluronic acid, releasing 64% of the payload over 6 d in vitro, whereas 83% was released over the same period in vivo[63]. This discrepancy can be attributed to the inability of in vitro conditions to effectively replicate the complex factors present in the in vivo environment, including the mechanical constraints imposed by the surrounding tissues (where tissue pressure affects the gel's morphology and porosity), inflammatory responses, foreign body reactions, and the absence of enzymatic degradation in PBS-based in vitro systems. For instance, Ding et al. reported that in vivo inflammation and osmotic pressure can induce the hydrogel's dehydration, reducing porosity and further slowing degradation[64]. Furthermore, the polymer micelle network of hydrogels exhibits higher density and mechanical strength at high concentrations within the local injection site, thereby further hindering drug diffusion[65]. In our study, Cy5.5-TRE synthesized via covalent conjugation of the fluorescent dye Cy5.5-COOH to TRE via an esterification reaction, exhibited a higher molecular weight and greater hydrophobicity than free TRE, potentially prolonging its residence time at the injection site.
Pharmacologically, sustained drug exposure effectively reduced mPAP, inhibited vascular remodeling and alleviated right ventricular hypertrophy. Importantly, unlike free TRE, which exhibited extremely low therapeutic blood concentrations with clinical IV or SC infusion doses ranging from 1.25 to 40 ng·kg–1·min–1[66,67], the exceptional inhibitory effect of TRE-MPs-Gel on pulmonary vascular remodeling may stem from the ability of long-acting formulations to maintain steady drug concentrations within the therapeutic window over an extended period beyond its prolonged antihypertensive effect. Notably, although the peak cumulative release of TRE in vitro occurred within 50 h and the drug release rate slowed thereafter, the depot continued to provide effective plasma concentrations of TRE over the following days, which may be attributed to the dual sustained release mechanism of the microparticles and the hydrogel, as well as the relatively slow degradation of the gel matrix.
The MCT model has been widely validated as a suitable platform for evaluating anti-PAH drugs, as it reproduces the key pathological features of PAH, including pulmonary vascular remodeling, inflammatory cell infiltration, and right ventricular hypertrophy[68−70]. In this study, the efficacy of TRE-MPs-Gel in the MCT model has been fully demonstrated. In contrast, the hypoxia/Sugen model induces endothelial cell apoptosis and excessive proliferation, leading to pulmonary endothelial hyperplasia and vascular remodeling similar to that observed in severe human PAH[68, 71,72]. Our previous study demonstrated that 3 weeks of bosentan treatment simultaneously ameliorated PAH in both MCT and hypoxia/Sugen rats, indicating that vasodilators are effective across different models[49]. Both bosentan and TRE are vasodilators, but with different mechanisms of action. Bosentan inhibits ET-1-mediated vasoconstriction and cell proliferation, whereas TRE acts on the IP receptor; both exert their effects via vasodilation and reduced vascular resistance[73,74]. Therefore, it is expected that TRE-MPs-Gel may also significantly ameliorate PAH in hypoxic/Sugen models.
-
In conclusion, this study developed a TRE depot that enables sustained drug release at the injection site for up to 3 d. This prolonged release system significantly reduces mPAP and effectively inhibits pulmonary vascular and right ventricular remodeling in MCT-induced rat PAH models. Compared with traditional IV or SC administration, this minimally invasive approach reduces the treatment burden associated with pumps and demonstrates favorable local tolerability. This system is promising for facilitating reproducibility and providing a robust foundation for clinical translation.
This study was supported by the National Natural Science Foundation of China (Nos. 82073782 and 82241002).
-
The animals used in all experiments followed the Regulations on the Management of Laboratory Animals and the Jiangsu Province Measures for the Management of Laboratory Animals, as well as the China Pharmaceutical University Institutional Animal Care and Use Committee (No. 202407033).
-
The authors confirm contribution to the work as follows: study conception and design: Yang P, He W; data collection: Li Z, Xie B; analysis and interpretation of results: Li Z, Xie B, Zou J, He X; draft manuscript preparation: Li Z, Xie B; manuscript revision and editing: Yang P, He W. All authors reviewed the results and approved the final version of the manuscript.
-
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
-
The authors have no conflicts of interest to declare.
-
accompanies this paper online at: https://doi.org/10.48130/targetome-0026-0029.
-
#Authors contributed equally: Zimin Li, Bing Xie
- Supplementary Fig. S1 Particle size (μm) of TRE-MPs in stability tests. Data are given as mean ± SD, n = 3.
- Supplementary Fig. S2 TRE content (%) of TRE-MPs in stability tests. Data are given as mean ± SD, n = 3.
- Supplementary Fig. S3 Cytotoxicity of TRE on N-PASMCs and PAH-PASMCs. Data are presented as mean ± SD, n = 6.
- Supplementary Fig. S4 Cytotoxicity of varying concentrations of TRE-MPs-Gel on PAH-PASMCs.
- Supplementary Fig. S5 Assessment of right ventricular hypertrophy in the MCT-induced rat model.
- Supplementary Fig. S6 Assessment of right ventricular cardiomyocyte hypertrophy in the MCT-induced rat model.
- Supplementary Text 1 Supplementary information for long-acting injectable in situ treprostinil depot for pulmonary hypertension.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press on behalf of China Pharmaceutical University. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Li Z, Xie B, Zou J, He X, He W, et al. 2026. A long-acting injectable in situ treprostinil depot for the targeted treatment of pulmonary hypertension. Targetome 2(3): e030 doi: 10.48130/targetome-0026-0029 

A long-acting injectable in situ treprostinil depot for the targeted treatment of pulmonary hypertension
- Received: 28 February 2026
- Revised: 20 April 2026
- Accepted: 06 May 2026
- Published online: 30 June 2026
Abstract: Pulmonary arterial hypertension (PAH) is a fatal, progressive cardiovascular disease. Treprostinil (TRE) is a first-line drug for PAH treatment. However, the use of TRE for severe PAH is often limited by the risks and complexities of pain at the subcutaneous (SC) infusion site or fatal catheter-associated intravenous (IV) infections with external or implanted pump systems. We engineered an injectable in situ-forming TRE depot at physiological temperature to prolong vasodilation by loading drug microparticles into a methylcellulose-based gel. A single intramuscular (IM) injection significantly prolonged the drug's residence at the injection site, increased the half-life of elimination, and lowered the maximal plasma concentration. One injection induced pulmonary vasodilation lasting 3–4 d, improved hemodynamics, and reduced pulmonary vascular remodeling. A safety evaluation showed favorable biocompatibility and local tolerability, with a mild local inflammatory response resolving within 1 week. In conclusion, the injectable TRE depot is a promising alternative to pump delivery, reducing the administration burden and improving compliance and quality of life.
-
Key words:
- Pulmonary arterial hypertension /
- Treprostinil /
- Microparticles /
- Hydrogel /
- Prolonged release /
- Long-acting