










-
Age-related macular degeneration affects roughly 200 million people worldwide, and neovascular age-related macualr degeneration (nAMD) is a leading cause of irreversible central vision loss in older adults[1,2]. Anti-vascular endothelial growth factor (anti-VEGF) therapy, beginning with ranibizumab and bevacizumab and later extended to aflibercept, transformed the natural history of nAMD and now allows most treated eyes to maintain or regain vision[3]. Newer agents have extended durability while preserving vision gains: Dual Ang-2/VEGF-A inhibition with faricimab delivered comparable 2-year outcomes on a treat-and-extend regimen[4], and high-dose aflibercept (8 mg) showed sustained efficacy with longer dosing intervals over 96 weeks[5]. Real-world outcomes are nonetheless uneven, and long-term treatment is accompanied by progressive macular atrophy in a substantial fraction of treated eyes, reshaping the ceiling on achievable visual function[6]. In clinical settings, we still judge treatment success mainly via best-corrected visual acuity (BCVA) and by anatomical endpoints revealed by optical coherence tomography (OCT), such as central retinal thickness and fluid status[7]. Whether these clinician-measured numbers reflect how patients actually see day to day is a separate question.
One problem with BCVA is that it measures letter recognition at a fixed distance under standardized high-contrast conditions. It does not capture real-world visual tasks such as reading, navigating unfamiliar environments, or driving. For this reason, regulators and guideline committees have pushed patient-reported outcome (PRO) measures as complementary endpoints. In retinal disease, the most widely used and validated instrument is the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25), which covers 12 domains of vision-related quality of life including near and distance activities, driving, mental health, and dependency[8]. The VFQ-25 was used to track changes in acuity in anti-VEGF trials[9]. Most age-related macular degeneration (AMD) studies using it have looked at its correlation with visual acuity; only a few studies have tested whether specific anatomical biomarkers are independently associated with what patients report.
Volumetric OCT can quantify individual components of the macular neovascular complex in three dimensions[10], and baseline compartment- and location-specific fluid volumes carry independent prognostic information for visual acuity outcomes[11]. Subretinal hyper-reflective material (SHRM) is one such component, and it is not a single entity. OCT angiography (OCTA) separates vascularized SHRM (vSHRM), which contains detectable flow and likely represents the neovascular membrane itself, from avascular SHRM (avSHRM), a fibrinous or proteinaceous exudate without flow[12]. The two behave differently: The volume of vSHRM reflects the active neovascular burden, whereas avSHRM has been linked to inflammatory exudation and to differences in the treatment response[13−15].
Our group has previously shown that these three-dimensional (3D) volumetric biomarkers carry prognostic information for clinician-measured endpoints in nAMD, including long-term injection burden and 2-year BCVA trajectories[16,17], and we have also characterized the behavior of avSHRM under anti-VEGF therapy[18] and linked the volume of avSHRM to photoreceptor integrity and functional outcomes[19]. Whether the same biomarkers are associated with patient-perceived visual function has not been tested.
When the fellow eye retains good acuity, VFQ-25 scores are driven mostly by the better-seeing eye[20,21], so any biomarker signal from the affected eye has to push through that ceiling. A finding in such a cohort would also be more clinically meaningful, because it would show that disease in one eye still measurably shapes quality of life. We therefore designed a prospective study to test whether baseline 3D OCT and OCTA lesion volumes are associated with 2-year NEI VFQ-25 outcomes in treatment-naïve nAMD eyes, beyond BCVA and clinical covariates.
-
This was a prospective cohort study conducted at two tertiary referral centers in Guangzhou, China. The study was registered with the Chinese Clinical Trial Registry (ChiCTR2200063428) and approved by the institutional ethics committees of Zhongshan Ophthalmic Center (approval 2022KYPJ117) and Guangdong Provincial People's Hospital (approval KY-H-2022-017-02). All procedures followed the Declaration of Helsinki. Written informed consent was obtained from every participant. Reporting followed the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines.
A total of 92 treatment-naïve patients with nAMD were enrolled, with one eye per patient. Macular neovascularization (MNV) was confirmed by fluorescein angiography, indocyanine green angiography, or OCTA. Eligible patients had to be willing to attend longitudinal follow-up and to have baseline spectral domain OCT imaging of adequate quality (signal strength index ≥ 6). Exclusion criteria were significant media opacity, active or prior uveitis, subfoveal fibrosis or atrophy, submacular hemorrhage obscuring the fovea, high myopia worse than −6.00 diopters, and any prior vitreoretinal surgery or photodynamic therapy. If both eyes were eligible, the eye with better image quality was chosen. MNV was confirmed by the presence of at least one of the following: (1) Leakage on fluorescein angiography, (2) hyperfluorescent plaque on indocyanine green angiography, or (3) a flow signal above the retinal pigment epithelium on OCTA. Diagnostic criteria followed the Consensus Nomenclature for Reporting Neovascular AMD Data[22].
All patients were treated with a standardized 3+ pro re nata (PRN) regimen using intravitreal ranibizumab, aflibercept, or conbercept, with monthly follow-up over 2 years. Three consecutive monthly injections were given as the loading treatment. During the PRN phase, retreatment was administered when follow-up OCT examinations showed the lesion's reactivation (new or persistent subretinal fluid, intraretinal fluid, or enlarged pigment epithelial detachment [PED]) or a decline in visual acuity of more than one Snellen line. The full treatment protocol and anatomical eligibility criteria, along with the imaging acquisition parameters and volumetric segmentation methodology, have been reported in our companion paper on structural outcomes from the same cohort[17].
Baseline imaging and 3D volumetric quantification
-
Baseline imaging used spectral domain OCT (SD-OCT; Spectralis, Heidelberg Engineering, Heidelberg, Germany) and OCTA (RTVue-XR Avanti, Optovue, Fremont, CA). OCT volumes covered a macular area of 8 mm × 6 mm with 61 horizontal B-scans at 100-μm spacing. OCTA provided co-registered 6-mm × 6-mm high-density macular scans. The OCTA data allowed us to separate vSHRM from avSHRM, which cannot be done via structural OCT alone.
Lesion segmentation was performed in 3D Slicer (version 5.4.0) with the SlicerMorph extension, following the protocol in our companion report[17]. Before measurement, the voxel dimensions were calibrated for each case. Using the Segment Editor tool, the lesion regions were manually annotated slice by slice across all 61 B-scans, and co-registered 6-mm × 6-mm OCTA B-scans were used to distinguish vascular from avascular components within SHRM and PED lesions. Within each baseline scan set, six lesion components were delineated: Subretinal fluid (SRF), intraretinal fluid (IRF), vSHRM, avSHRM, fibrovascular PED (fvPED), and serous PED (sPED); vSHRM and fvPED were defined by the corresponding OCTA flow signals, whereas avSHRM and sPED lacked detectable flow. The current analysis used five of these (avSHRM, IRF, vSHRM, SRF, and sPED) and total lesion volume, defined as the sum of all components. Fibrovascular PED was dropped because it was too infrequent in this cohort to yield stable regression estimates. Representative baseline OCT/OCTA images and the corresponding 3D volumetric reconstructions for three illustrative nAMD cases are shown in Fig. 1. Two investigators (J.P. and X.Z.) segmented each scan independently, masked to the clinical and functional data. Inter-rater reliability was good for all components (intraclass correlation coefficients of 0.88–0.92). We used the mean of the two measurements for analysis. Acquisition parameters, segmentation boundaries, and reproducibility testing are described in full elsewhere[17,18].
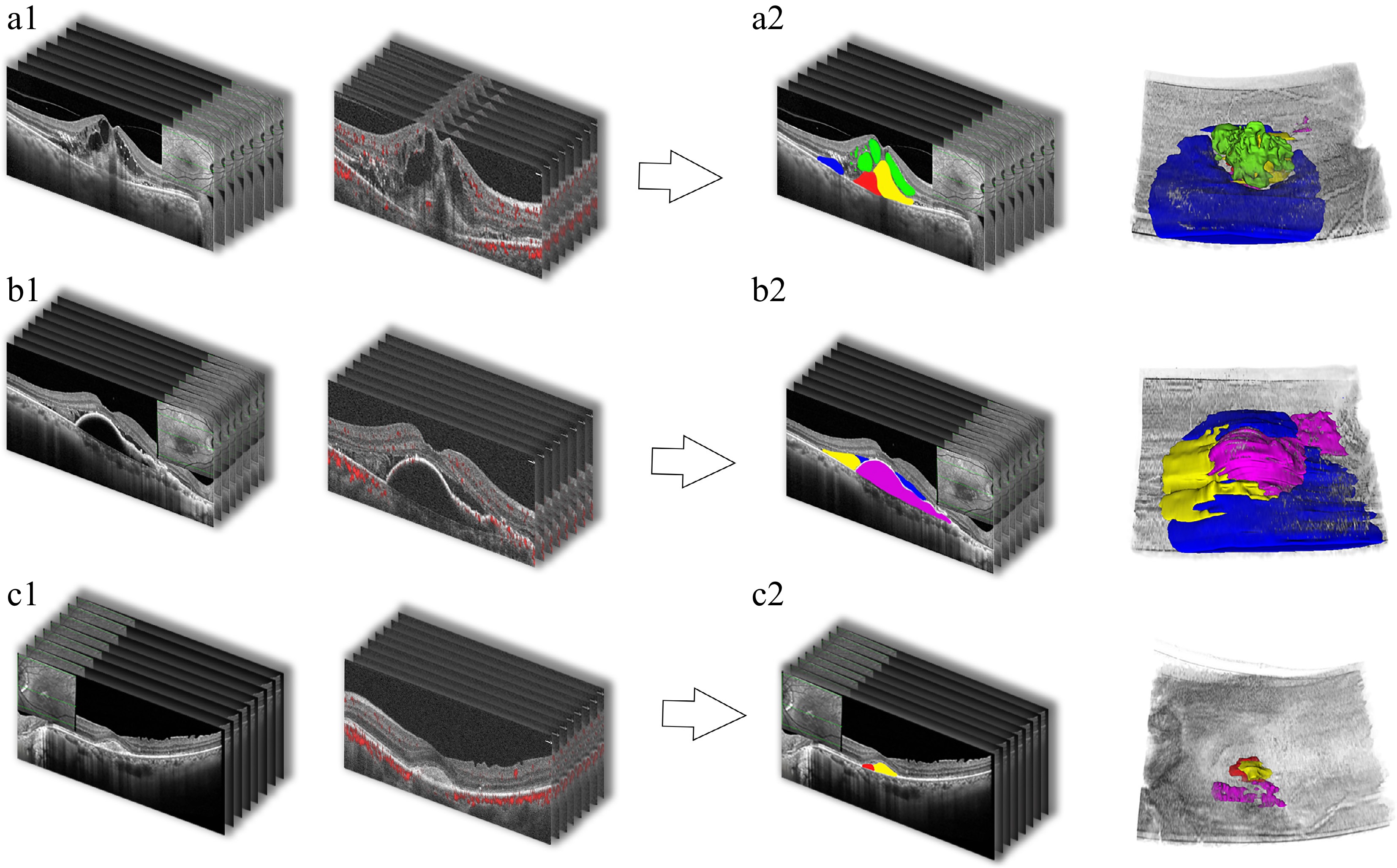
Figure 1.
The 3D baseline OCT/OCTA volumetric reconstruction workflow in three representative nAMD cases (Cases A, B, and C). For each case, subpanels labeled 1 show the raw baseline spectral-domain OCT B-scan stack (left) and the corresponding OCTA B-scan stack with flow signals (right). Subpanels labeled 2 show the color-coded segmentation of lesion components on OCT B-scans (left) and the resulting 3D volumetric reconstruction (right). Color coding: subretinal fluid (SRF, dark blue), intraretinal fluid (IRF, green), vascular subretinal hyperreflective material (vSHRM, red), avascular SHRM (avSHRM, yellow), fibrovascular pigment epithelial detachment (fvPED, brown), and serous PED (sPED, pink).
Patient-reported outcome assessment
-
Vision-related quality of life was measured with the NEI VFQ-25 plus the 13-item supplement, yielding 38 items in total[8]. We used the validated Chinese-language version and administered it at the 2-year visit. Many of our patients were elderly with limited literacy, so a trained researcher (J.P.) delivered every questionnaire as a face-to-face interview. The questionnaire yields 12 subscales: General health, general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, color vision, peripheral vision, and driving. Scoring followed the standard RAND Corporation/National Eye Institute (RAND/NEI) algorithm: Items were rescaled to 0–100, and each subscale was the mean of its items, with higher scores indicating better visual function. The driving subscale was dropped because more than 75% of the participants did not drive. A composite score was computed as the unweighted mean of the 10 vision-targeted subscales (with general health and driving excluded).
Visual acuity grouping
-
Patients were stratified by the studied eye's BCVA at the 2-year visit (logMAR) into three groups: Good (≤ 0.30, Snellen ~20/40 or better), moderate (> 0.30 to ≤ 1.00, ~20/50 to 20/200), and poor (> 1.00, worse than 20/200). These strata were used to describe VFQ-25 subscale distributions across levels of visual outcome.
Statistical analysis
-
Normally distributed continuous variables are reported as the mean ± standard deviation (SD). Categorical variables are shown as frequencies and percentages. VFQ-25 subscale scores were compared across the three BCVA groups with the Kruskal–Wallis test. Subscales with a mean score ≥ 80 were considered to show a ceiling effect and were not used as regression outcomes, since the narrow variance limits statistical power. Five subscales met this criterion: Ocular pain, social functioning, dependency, color vision, and peripheral vision. Together with general health (nonvision) and driving (> 75% missing), this left six outcomes for regression: The composite score, near activities, distance activities, general vision, mental health, and role difficulties.
Univariate associations between the six baseline biomarker volumes and the six outcomes were estimated with standardized linear regression (both the predictor and outcome were z-scored). The resulting 36 tests were corrected for multiple testing using the Benjamini–Hochberg false discovery rate (FDR) procedure at q < 0.05. Associations that survived FDR correction were then carried forward into the multivariable models. The adjustment set included baseline study-eye BCVA, baseline fellow-eye BCVA, age, sex, MNV type, and anti-VEGF agent. Two-year BCVA was not included as a covariate because it lies on the causal pathway from the baseline morphology to patient-reported outcomes; adjusting for it would bias the estimate of interest. For each biomarker, we computed ΔR2, namely the difference in R2 between the full model and the covariates-only model, to quantify its independent contribution. The 95% confidence intervals are reported for the primary regression coefficients. Residual normality was checked with the Shapiro–Wilk test. We ran two sensitivity analyses: One additionally adjusting for the cumulative number of anti-VEGF injections over 2 years, and one repeating all models using natural log-transformed biomarker volumes [ln(volume + 1)] to limit the influence of extreme values. Analyses were performed in R (version 4.3.x). A two-sided p < 0.05 was considered to be statistically significant.
-
Ninety-two eyes of 92 patients were studied (Table 1). The mean age was 65.8 ± 7.3 years. Seventy patients (76.1%) were male. The MNV subtypes were Type 1 PCV in 46 eyes (50.0%), Type 1 non-PCV in 10 (10.9%), and Type 2 in 36 (39.1%). Patients received ranibizumab (n = 36, 39.1%), aflibercept (n = 20, 21.7%), or conbercept (n = 36, 39.1%). Patients received 5.9 ± 3.2 injections (range: 3–13) over 2 years. BCVA improved from 0.6 ± 0.4 to 0.5 ± 0.4 logarithm of the minimum angle of resolution (logMAR) (p < 0.001, paired t-test); fellow-eye BCVA at 2 years was 0.2 ± 0.1 logMAR. By 2-year BCVA, 38 eyes (41.3%) were good, 44 (47.8%) were moderate, and 10 (10.9%) were poor. Mean baseline lesion volumes were as follows: avSHRM, 0.85 ± 1.86 mm3; vSHRM, 0.10 ± 0.27 mm3; subretinal fluid, 0.38 ± 0.60 mm3; intraretinal fluid, 0.06 ± 0.16 mm3; sPED, 0.34 ± 1.14 mm3; total lesion volume, 2.55 ± 3.34 mm3.
Table 1. Demographic and clinical characteristics of the study cohort.
Characteristic Value Age, years 65.8 ± 7.3 Male sex, n (%) 70 (76.1%) MNV type, n (%) Type 1 (PCV) 46 (50.0%) Type 1 (non-PCV) 10 (10.9%) Type 2 36 (39.1%) Symptom duration, months 10.3 ± 15.7 2-year injection count 5.9 ± 3.2 Anti-VEGF agent, n (%) Ranibizumab 36 (39.1%) Aflibercept 20 (21.7%) Conbercept 36 (39.1%) Systemic conditions, n (%) Hypertension 36 (39.1%) Diabetes mellitus 8 (8.7%) Visual acuity, logMAR Baseline BCVA, study eye 0.6 ± 0.4 2-year BCVA, study eye 0.5 ± 0.4 2-year BCVA, fellow eye 0.2 ± 0.1 2-year BCVA group, n (%) Good (≤ 0.30) 38 (41.3%) Moderate (0.30–1.00) 44 (47.8%) Poor (> 1.00) 10 (10.9%) Baseline lesion volumes, mm³ IRF 0.06 ± 0.16 SRF 0.38 ± 0.60 vSHRM 0.10 ± 0.27 avSHRM 0.85 ± 1.86 sPED 0.34 ± 1.14 Total lesion volume 2.55 ± 3.34 Values reported as the mean ± SD. BCVA, best-corrected visual acuity; IQR, interquartile range; MNV, macular neovascularization; PCV, polypoidal choroidal vasculopathy; SHRM, subretinal hyperreflective material (av, avascular; v, vascular); SRF, subretinal fluid; IRF, intraretinal fluid; sPED, serous pigment epithelial detachment. The VFQ-25 composite score averaged 78.8 ± 3.4 at 2 years (Table 2, Fig. 2a). The highest subscales were peripheral vision (90.8 ± 8.9), dependency (88.4 ± 6.5), and social functioning (87.1 ± 8.0); color vision (84.6) and ocular pain (83.6) also exceeded 80. Lower scores were seen for near activities (70.5 ± 10.4), general vision (68.4 ± 10.6), and mental health (65.2 ± 7.7). General health scored 38.2 ± 14.0. Driving was excluded because more than 75% of participants were nondrivers.
Table 2. The NEI VFQ-25 subscale scores for the full cohort and stratified by 2-year BCVA outcome group.
Subscale All (n = 92) Good (n = 38) Moderate (n = 44) Poor (n = 10) p-value Distance activities 78.2 ± 7.7 82.1 ± 6.7 76.2 ± 7.1 72.1 ± 6.5 < 0.001 Near activities 70.5 ± 10.4 73.8 ± 9.3 70.6 ± 9.9 57.5 ± 6.2 < 0.001 Composite 78.8 ± 3.4 80.1 ± 2.8 78.3 ± 3.5 75.8 ± 2.3 < 0.001 General vision 68.4 ± 10.6 71.7 ± 8.2 66.2 ± 12.5 65.5 ± 5.5 0.021 Mental health 65.2 ± 7.7 66.8 ± 9.0 64.1 ± 6.5 63.5 ± 6.7 0.176 Ocular pain 83.6 ± 10.8 82.6 ± 8.0 84.7 ± 11.4 82.5 ± 16.9 0.444 Role difficulties 71.1 ± 9.3 71.2 ± 6.7 71.6 ± 11.1 68.7 ± 9.3 0.446 Peripheral vision 90.8 ± 8.9 91.8 ± 6.7 89.8 ± 9.4 91.2 ± 13.2 0.563 General health 38.2 ± 14.0 40.2 ± 13.9 36.9 ± 13.6 36.5 ± 16.8 0.614 Social functioning 87.1 ± 8.0 87.7 ± 7.2 87.2 ± 7.7 84.2 ± 12.1 0.859 Dependency 88.4 ± 6.5 88.5 ± 7.2 88.4 ± 6.0 88.1 ± 6.9 0.912 Color vision 84.6 ± 14.8 84.7 ± 15.0 84.3 ± 15.5 85.0 ± 12.9 0.996 Values are the mean ± SD. The p-values are from the Kruskal–Wallis test comparing the three BCVA groups. Bold p-values indicate p < 0.05. Subscales are ordered by p-value (most significant first). Composite = unweighted mean of 10 vision-targeted subscales (excluding general health and driving). Good: ≤ 0.30 logMAR; moderate: 0.30–1.00; poor: > 1.00. 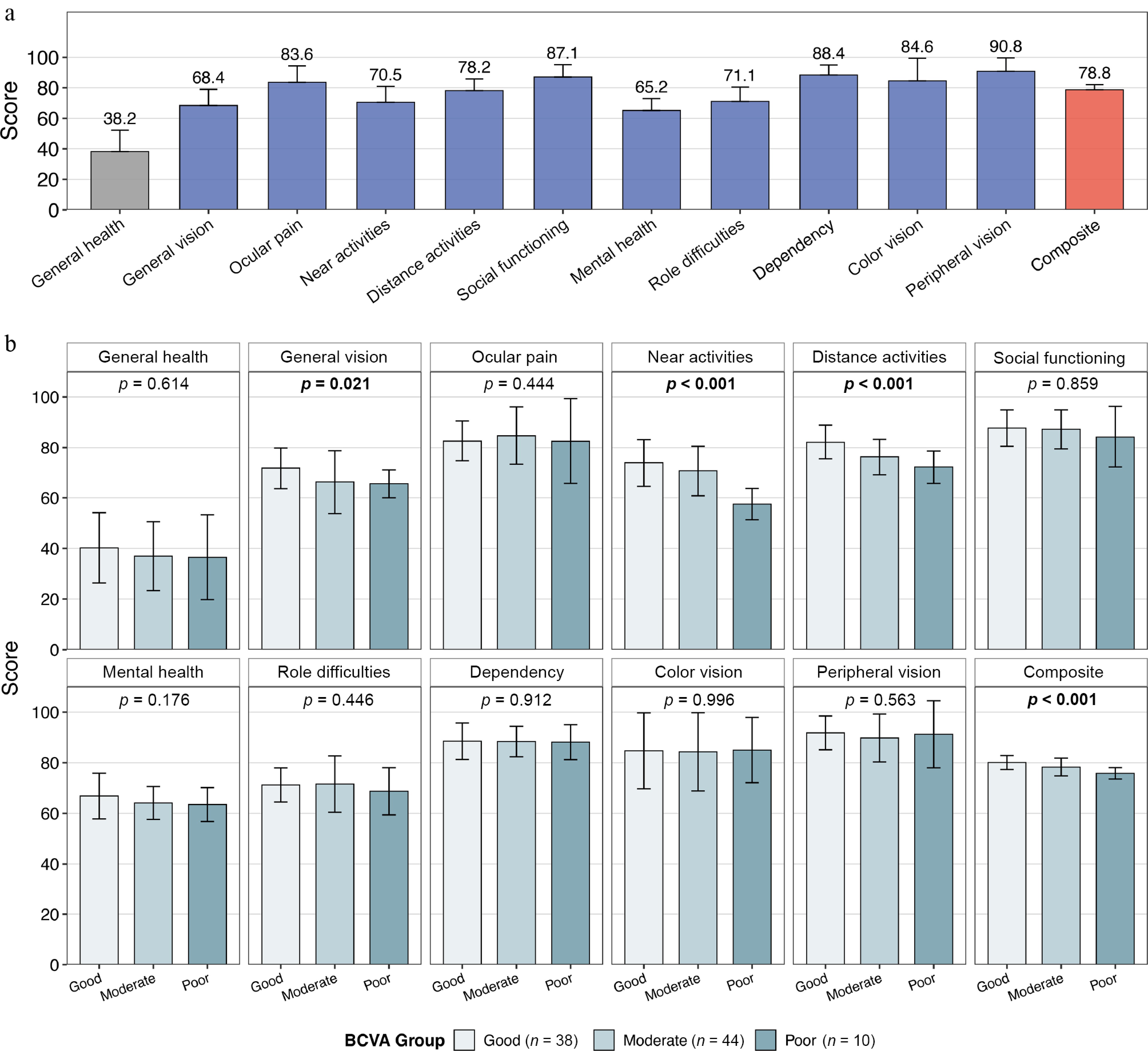
Figure 2.
The NEI VFQ-25 scores in the study cohort. (a) Mean subscale scores for the full cohort (n = 92), ordered by the questionnaire sequence. The composite score is shown on the right. (b) Subscale score distributions across the three 2-year BCVA outcome groups (good, ≤ 0.30 logMAR; moderate, > 0.30 to ≤ 1.00; poor, > 1.00). Bars represent the mean ± SD. The p-values are from Kruskal–Wallis tests; bold indicates p < 0.05.
Four subscales differed across the good, moderate, and poor BCVA groups (Table 2, Fig. 2b): Distance activities (p < 0.001), near activities (p < 0.001), composite (p < 0.001), and general vision (p = 0.021). The mean near activities scores were 73.8 ± 9.3, 70.6 ± 9.9, and 57.5 ± 6.2 in the good, moderate, and poor groups, respectively. The remaining subscales did not differ: Mental health (p = 0.176), ocular pain (p = 0.444), role difficulties (p = 0.446), peripheral vision (p = 0.563), social functioning (p = 0.859), dependency (p = 0.912), color vision (p = 0.996), and general health (p = 0.614).
In total, 3 of 36 univariate associations survived FDR correction at q < 0.05 (Table 3). Vascular SHRM was inversely associated with the composite score (standardized β = −0.507, p < 0.001, q < 0.001) and with near activities (standardized β = −0.351, p < 0.001, q = 0.011). Avascular SHRM was inversely associated with near activities (standardized β = −0.329, p = 0.001, q = 0.016). Additional nominal associations (p < 0.05) for SRF, avSHRM, vSHRM, and total lesion volume with several subscales did not survive FDR correction.
Table 3. Univariate and multivariate standardized regression of the baseline lesion volumes on NEI VFQ-25 subscale scores.
Composite Near activities Distance activities General vision Mental health Role difficulties Std β p Std β p Std β p Std β p Std β p Std β p Univariate IRF −0.148 0.158 −0.062 0.558 −0.031 0.770 −0.083 0.434 0.055 0.604 0.192 0.067 SRF −0.242 0.020 −0.063 0.548 −0.074 0.483 −0.036 0.733 −0.145 0.168 −0.031 0.766 vSHRM −0.507 < 0.001 −0.351 < 0.001 −0.220 0.035 −0.189 0.071 −0.103 0.330 −0.124 0.237 avSHRM −0.098 0.352 −0.329 0.001 −0.251 0.016 −0.013 0.904 0.017 0.874 0.048 0.651 sPED 0.088 0.405 0.192 0.066 0.107 0.310 0.052 0.620 −0.083 0.434 0.034 0.746 Total volume −0.208 0.047 −0.253 0.015 −0.235 0.024 −0.072 0.498 −0.057 0.587 −0.006 0.952 Multivariate vSHRM −0.366 0.001 −0.129 0.286 − − − − − − − − avSHRM − − −0.370 < 0.001 − − − − − − − − Model R2 0.373 0.387 − − − − ΔR2 0.080 0.119 − − − − Univariate and multivariate standardized regression of baseline 3D lesion volumes on NEI VFQ-25 subscale scores. The univariate rows report standard β and p-values for all 36 pairs of baseline biomarker volume measures (avSHRM, IRF, vSHRM, SRF, sPED, total lesion volume) × VFQ-25 subscales (composite, near activities, distance activities, general vision, mental health, role difficulties). p-values shown in bold indicate pairs that survived Benjamini–Hochberg FDR correction at q < 0.05 across the 36 univariate tests. FDR-surviving pairs were then entered into multivariate models adjusting for baseline study-eye BCVA, fellow-eye BCVA, age, sex, MNV type, and anti-VEGF agent; multivariate p-values shown in bold also denote pairs surviving a second round of Benjamini–Hochberg correction applied across the multivariate tests. Model R2 refers to the full multivariate model (biomarker plus all covariates), and ΔR2 is the incremental variance explained by the biomarker term beyond the covariates-only model. BCVA, best-corrected visual acuity; FDR, false discovery rate; MNV, macular neovascularization; SHRM, subretinal hyperreflective material (a, avascular; v, vascular); SRF, subretinal fluid; IRF, intraretinal fluid; sPED, serous pigment epithelial detachment; Std β: standardized beta. Two associations held in multivariate models adjusting for age, sex, MNV subtype, anti-VEGF agent, baseline BCVA, and fellow-eye BCVA (Table 3, Fig. 3). Vascular SHRM remained inversely associated with the composite score (standardized β = −0.366, p = 0.001, q = 0.002). Avascular SHRM remained inversely associated with near activities (standardized β = −0.370, p < 0.001, q < 0.001). The vSHRM–near activities association was attenuated (standardized β = −0.129, p = 0.286, q = 0.286). The full models explained 37.3% of the variance in the composite score and 38.7% in the near activities subscale. The biomarker term contributed ΔR2 of 8.0% and 11.9%, respectively.
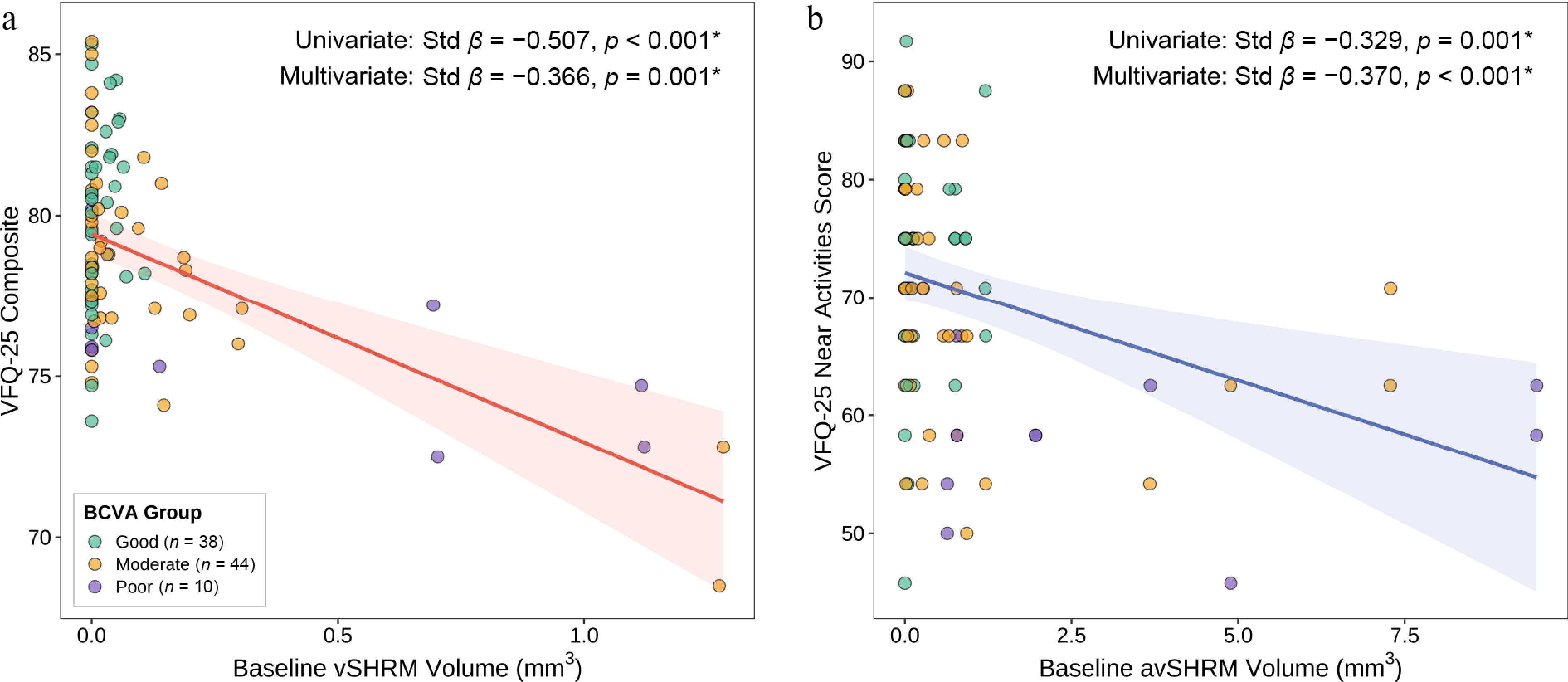
Figure 3.
Scatter plots of the two FDR-surviving baseline biomarker–NEI VFQ-25 associations. (a) Baseline vSHRM volume versus the NEI VFQ-25 composite score. (B) Baseline avSHRM volume versus the NEI VFQ-25 near activities score. Each point represents one eye, color-coded by 2-year BCVA outcome group. Solid lines and shaded bands show the fit of ordinary least squares regression and the 95% confidence intervals. Univariate and multivariate standardized β and p-values are annotated in each panel.
Both primary associations were stable across sensitivity analyses (Supplementary Table S1). With injection count added as a covariate, avSHRM was associated with near activities (standardized β = −0.372, p < 0.001), and vSHRM was associated with the composite score (standardized β = −0.344, p = 0.003). Using log-transformed volumes, the corresponding estimates were standardized β = −0.435 (p < 0.001) and standardized β = −0.385 (p = 0.001).
-
In this cohort, two baseline volumetric biomarkers were associated with patient-reported visual function 2 years later. Of 36 univariate biomarker–subscale pairs, 3 survived FDR correction. After adjustment for BCVA, age, sex, MNV type, and anti-VEGF agent, vSHRM was still associated with the VFQ-25 composite score (standardized β = −0.366), and avSHRM was associated with the near activities subscale (standardized β = −0.370). The biomarker terms added 8.0% and 11.9% of the increase in variance beyond the clinical covariates, and both held up under the injection count and log-transformed sensitivity checks. Volumetric imaging at diagnosis seems to carry prognostic information about how patients will later rate their own vision.
Vascularized SHRM, defined by OCTA flow within the subretinal compartment, is active neovascular tissue[12,15]. A larger volume at baseline means more active tissue, and the recurrent exudation this drives is a plausible route to ellipsoid zone disruption and photoreceptor damage[23]. Why this should show up in the composite score rather than in a specific subscale is less obvious to us. One possibility, though we lack direct evidence, is that diffuse fluctuating exudation degrades many small aspects of daily vision rather than any single domain, and the composite score simply sums those small deficits. The direction of the finding is consistent with CATT, where SHRM's presence predicted worse acuity[14] and where SHRM and persistent fluid were spatially co-located with subsequent areas of macular atrophy and fibrotic scar at 2 years[24]; with the HAWK/HARRIER post hoc data on treatment response[25]; and with the cross-sectional correlation reported by Kumar et al.[26]. In a companion paper from our group, eyes whose vSHRM resolved during loading went on to need fewer subsequent injections[17]. Kawashima et al. had earlier shown that vSHRM often persists after three aflibercept injections and is associated with failure to achieve a dry macula, whereas avSHRM tends to resolve more readily[15], so a large baseline vSHRM burden may mark eyes that are hardest to dry out.
Avascular SHRM is fibrinous exudate, cellular debris, and early fibrotic material sitting between photoreceptors and the retinal pigment epithelium (RPE)[13]. Sitting where it does, it plausibly disrupts the close metabolic coupling the outer retina depends on from the RPE[27], and whatever damage it leaves behind is concentrated where cone density is highest, at the fovea[28]. Near tasks such as reading small print or finding objects on a cluttered shelf demand high-acuity foveal function in a way that distance tasks do not[29]. If avSHRM preferentially scars the fovea, near vision is where the loss will be felt first. In a companion analysis from our group, avSHRM showed variable absorption under anti-VEGF therapy[18], and Roberts et al. described the gradual shift of vascular lesion components toward fibrosis over time[30]. The compartmental distribution of residual fluid itself shapes the downstream atrophy and fibrosis risk during long-term treatment[31]. Persistent avSHRM leaves a structural residue, and that residue sits exactly where the near activities items are scored. Orr et al. validated the NEI VFQ-25 in an nAMD cohort and found that near activity scores correlated with reading performance,[29] and the VFQ-25 has been shown to retain reliability and construct validity in geographic atrophy populations[32].
The specificity of our findings that significant associations for the composite score and near nctivities subscale but not for other subscales reflects both biological and psychometric factors. Near activity items (reading small print, seeing well up close) are fovea-dependent tasks requiring high spatial resolution, making them sensitive to structural macular damage. In contrast, subscales like color vision, peripheral vision, and ocular pain showed ceiling effects and minimal variance, limiting thee statistical power to detect associations. Moreover, the NEI VFQ-25 assesses binocular function; in our cohort with unilateral nAMD and healthy fellow eyes, tasks easily compensated by the better-seeing eye (e.g., social functioning, dependency) showed no biomarker associations. The composite score, as an aggregate measure, captures the cumulative functional impact across multiple domains, explaining its sensitivity to the vSHRM burden.
Five subscales exhibited ceiling effects (ocular pain, social functioning, dependency, color vision, and peripheral vision all had means above 80), a known limitation of the NEI VFQ-25 in populations with preserved peripheral and color vision. This instrument-related constraint is well-documented in AMD populations and reflects the binocular nature of the questionnaire, where tasks are easily compensated by a healthy fellow eye (e.g., color vision, peripheral vision, ocular pain) show minimal variance. The fellow eyes in this cohort had a mean BCVA near 0.2 logMAR (20/32), which is more than enough for most of what those subscales measure, and the better-seeing eye is known to dominate NEI VFQ-25 scores[20,21]. The consequence is that for ceiling-compressed instruments of this kind, reported effect sizes likely underestimate the true monocular impact. Only the high-acuity subscales (near and distance activities) and the composite score retained enough spread for a biomarker signal to emerge. Future nAMD studies may benefit from incorporating monocular patient-reported outcome measures and newer instruments, such as the macular treatment satisfaction questionnaire (MacTSQ), to better assess eye-specific functional burden that may be underestimated by the NEI VFQ-25.
The incremental variance explained by baseline biomarkers is modest but clinically meaningful in the context of prognostic counseling. At the time of diagnosis, patients with large baseline vSHRM or avSHRM volumes can be informed that their patient-reported visual function outcomes at 2 years may be more limited, even if their BCVA improves. This information helps set realistic expectations and may guide shared decision-making regarding treatment commitment and follow-up adherence. However, these findings are not yet sufficient for treatment modification. The effect sizes are insufficient to justify altering monitoring intervals or switching agents depending solely on the baseline biomarker volumes. Rather, these biomarkers should be viewed as prognostic stratification tools that complement BCVA in comprehensive outcome assessments. Future research integrating baseline biomarkers with early treatment response dynamics may yield actionable decision rules, but such models require prospective validation before their clinical implementation.
These findings should also be interpreted in the context of the sample size. However, the multivariable models were deliberately restricted to the small number of associations surviving FDR correction, and the two primary associations remained materially consistent in sensitivity analyses with additional adjustment for injection number and with log-transformed biomarker volumes. Taken together, this pattern supports the stability of the main findings, although confirmation in larger independent cohorts remains warranted.
The most important limitation is that we only measured NEI VFQ-25 at Year 2, so we cannot assess the change in patient-reported visual function from the baseline. Second, the cohort is also modest: 92 patients from two centers on a pro re nata regimen. Third, the NEI VFQ-25 assesses binocular visual function, and subtle fellow-eye disease may influence patient-reported outcomes beyond what BCVA alone captures. This unquantified fellow-eye burden may have attenuated the observed associations between study-eye biomarkers and NEI VFQ-25 scores. Moreover, although the anti-VEGF agent was included as a covariate in the adjusted models, the cohort size did not permit a well-powered formal assessment of biomarker × agent interaction; therefore, treatment heterogeneity remains an important issue for future studies.
-
Baseline vSHRM and avSHRM volumes were independently associated with how patients rated their own vision 2 years after a diagnosis of nAMD. For now, these two volumetric measurements at the time of diagnosis are the clearest imaging handles we have on how a patient will later experience their own vision.
-
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Zhongshan Ophthalmic Center (approval 2022KYPJ117, dated 2022-06-21) and Guangdong Provincial People's Hospital (approval KY-H-2022-017-02, dated 2022-05-05). Written informed consent was obtained from all participants.
-
The authors confirm their contributions to the paper as follows: study concept and design, acquisition, analysis, and interpretation of data: Pu J, Zhuang X, Wen F; drafting of the manuscript, statistical analysis: Pu J, Zhuang X; revision of the manuscript: Wen F, Li M, Borrelli E, Marolo P, Cao D, Zhang L, Cheng Z, Cui Y; administrative, technical, or material support: Wen F, Li M, Mi L, Ji Y, He G, Hao X, Su Y, Chen X; study supervision: Zhang L, Wen F, Cheng Z. All authors reviewed the results and approved the final version of the manuscript.
-
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
-
This work was supported by the China Postdoctoral Science Foundation (2025M772435), the National Natural Science Foundation of China (General Program, Grant No. 82371063), the GDPH Supporting Fund (8257040141; 8250040357), and the GDPH Postdoctoral Program (BY012024027).
-
The authors declare that they have no conflict of interest.
-
accompanies this paper online at: https://doi.org/10.48130/vns-0026-0023.
-
# Authors contributed equally: Xuenan Zhuang, Jiaxin Pu, Dan Cao
- Supplementary Table S1 Sensitivity analyses for the two primary FDR-surviving associations.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Zhuang X, Pu J, Cao D, Borrelli E, Marolo P, et al. 2026. Association of baseline three-dimensional lesion volumes with two-year patient-reported visual function after anti-vascular endothelial growth factor therapy in neovascular age-related macular degeneration. Visual Neuroscience 43: e030 doi: 10.48130/vns-0026-0023 

Association of baseline three-dimensional lesion volumes with two-year patient-reported visual function after anti-vascular endothelial growth factor therapy in neovascular age-related macular degeneration
- Received: 08 April 2026
- Revised: 24 April 2026
- Accepted: 13 May 2026
- Published online: 30 June 2026
Abstract: This prospective cohort study tested whether baseline three-dimensional optical coherence tomography (OCT) and OCT angiography (OCTA) lesion volumes are associated with patient-reported visual function after anti-vascular endothelial growth factor (anti-VEGF) therapy in neovascular age-related macular degeneration (nAMD). Ninety-two treatment-naïve nAMD eyes underwent volumetric segmentation of their baseline lesion components, including vascular subretinal hyper-reflective material (vSHRM), avascular subretinal hyper-reflective material (avSHRM), subretinal fluid, intraretinal fluid, and serous pigment epithelial detachment. The National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) was administered at the 2-year visit. Univariate standardized regressions across 36 biomarker–subscale pairs were corrected for multiple testing with the Benjamini–Hochberg false discovery rate (FDR). Three univariate associations survived FDR correction (q < 0.05). In multivariate analysis, baseline vSHRM volume was independently associated with a worse VFQ-25 composite score (standardized β = −0.366, p = 0.001), and baseline avSHRM volume was independently associated with a worse near activities score (standardized β = −0.370, p < 0.001), adding 8.0% and 11.9% incremental variance beyond clinical covariates. Baseline vSHRM and avSHRM volumes thus add prognostic information about patient-reported visual function beyond best-corrected visual acuity and clinical covariates. This study was registered in Chinese Clinical Trial Registry (www.chictr.org.cn/showproj.html?proj=173189; ID: ChiCTR2200063428; date of registration: 2022-09-06).