










-
Myopia has been recognized as a global public health concern. Without effective intervention measures, it is estimated to affect half of the world's population by 2050[1]. As the prevalence of myopia increases, the visual impairment resulting from conditions associated with myopia will accumulate. Myopia, in particular high myopia, could lead to serious ocular conditions, including retinal detachment, posterior scleral staphyloma, choroidal neovascularization, and myopic maculopathy[2]. Pathologic myopia constitutes a substantial disease burden to the society. Thus, finding an effective and safe method to prevent the progression of myopia is crucial.
Several therapies demonstrate methods for clinically meaningful slowing of myopia progression, including multifocal soft contact lenses[3], low-concentration atropine[4], overnight orthokeratology[5], and repeated low-level red-light (RLRL) therapy[6]. The efficacy of atropine, a non-selective muscarinic antagonist primarily known to induce pupil dilation, has been confirmed by a clear concentration-dependent response observed in the Atropine for the Treatment of Myopia phase 2 (ATOM2) study and Low-Concentration Atropine for Myopia Progression phase 1 (LAMP1) study[7,8]. Currently, topical atropine is the only widely accessible ophthalmic formulation with an established efficacy profile[9]. A concentration of 0.01% atropine is considered optimal for balancing the efficacy, rebound effects, and side effects (pupil dilation, photophobia, and near blur), making it the most widely used pharmacological intervention. Prior studies have reported that 0.01% atropine reduces spherical equivalent refraction (SER) progression by 27−83% in children[10]. Because of its well-established efficacy and safety profile through multiple randomized controlled trials (RCTs), 0.01% atropine has become the clinical gold standard and the preferred control regimen in myopia intervention studies, recommended by both domestic and international guidelines. However, the inhibitory effect of 0.01% atropine on myopia progression remains controversial[4], and its side effects, though mild, still limit long-term adherence.
RLRL therapy, traditionally utilized for amblyopia treatment in children, has recently been repurposed for myopia control. It has shown significant efficacy in slowing myopic progression[11]. However, concerns regarding its potential for causing retinal structural damage have been raised in the literature. Foveal structural damage with reversible vision loss after five months of RLRL therapy has been reported in one study[12], and reduced paracentral foveal cone density following RLRL treatment has been reported by another study[13].
Against this background, we designed a multicenter, randomized, parallel-group, single-blind clinical trial to compare the efficacy of low-concentration atropine with that of RLRL therapy in myopia control. Additionally, we aim to evaluate the safety profiles of both interventions, with particular focus on the potential retinal damage risks associated with RLRL therapy.
-
We conducted a 12-month, multi-center, single-masked, parallel-group RCT in which 139 children were enrolled between November 2021 and July 2022 at Chongqing General Hospital and the First Affiliated Hospital of Chongqing Medical University, Chongqing, China. All examinations at baseline and follow-up visits were performed by the same examiners using the same protocol and equipment throughout. The investigators and key personnel at each site involved in the present study were trained and certified before study commencement. No changes in the protocol or methods were made after trial commencement.
This trial was registered in the Chinese Clinical Trial Registry (
www.chictr.org.cn ) with the registration number ChiCTR2100052653. Written informed consent was obtained from the parents or legal guardians. All procedures adhered to the tenets of the Declaration of Helsinki and were approved by the Ethics Committee of Chongqing General Hospital (Approval No. KYS2021-011-01, dated May 28, 2021) and the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (Approval No. 2021-426, dated September 15, 2021). The trial was planned to be terminated early if any of the following criteria were met: (1) occurrence of serious adverse events considered definitely or possibly related to the study intervention in more than 5% of participants in either group; (2) a confirmed case of irreversible visual loss or retinal structural damage attributed to the study intervention. No early termination occurred during the conduct of this trial.Inclusion and exclusion criteria
-
Children aged 6–12 years with cycloplegic SER between −6.00 and −1.00D, and a best-corrected visual acuity (BCVA) of 0.0 logMAR (equivalent to Snellen 1.0 or 20/20 vision) or better in both eyes were included. Age was calculated based on the actual age at enrollment. Exclusion criteria included astigmatism > 2.00D, anisometropia > 1.50D, abnormal intraocular pressure, serious ocular or systemic disease, and allergy to atropine or cyclopentanone. Those who had previously received myopia-controlling therapies such as atropine eye drops, RLRL, defocus-incorporated multiple-segment (DIMS) spectacle lenses, and orthokeratology contact lenses were also excluded.
Randomization and masking
-
Eligible subjects were randomly allocated to either the RLRL group (650 nm) or the low-concentration atropine group (0.01%) according to a randomization list pre-generated by a computer program. Because of the nature of the intervention, parents and children were made aware of the study allocation. Outcome assessors such as technicians, optometrists, and statisticians were masked to the treatment allocation (Fig. 1).
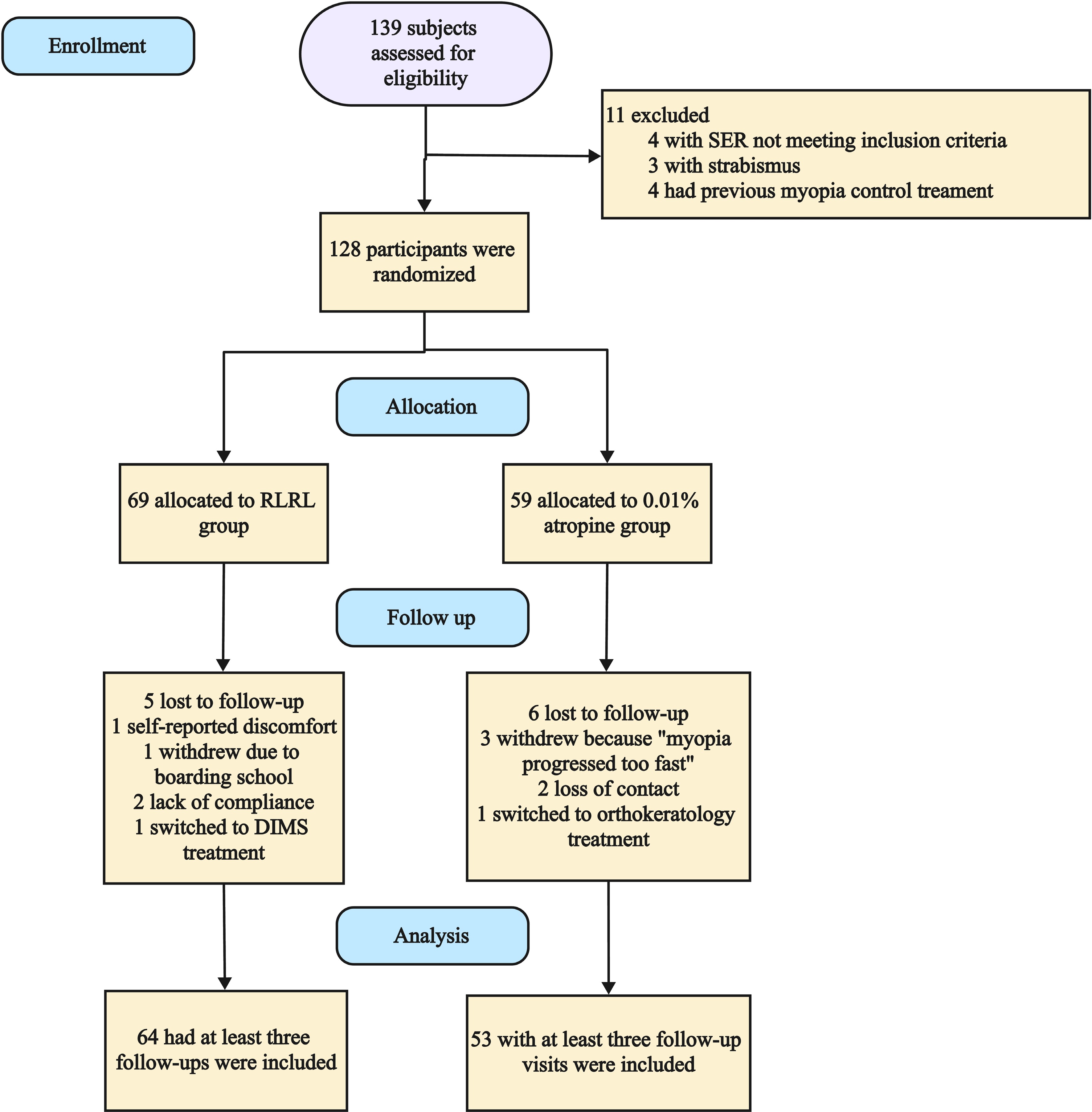
Figure 1.
Study design and flow diagram of the randomized, controlled clinical trial. SER = spherical equivalent refraction; RLRL = repeated low-level red-light; DIMS = defocus-incorporated multiple segments.
Study procedures
-
A repeated low-level red-light therapy device (Eyerising; Suzhou Xuanjia Optoelectronics Technology, Suzhou, China) was used in this study. It consists of semiconductor laser diodes, which deliver low-level red light with a wavelength of 650 ± 10 nm at an illuminance level of approximately 1,600 lx through the pupil to the fundus. Subjects in the RLRL group took the device home, where they were instructed to complete the treatment twice daily with an interval of at least 4 h, with each treatment lasting 3 min, for 7 days per week. Subjects were asked to adjust the best position and wear refractive correction spectacles before use to ensure the light entered the eyes properly. To ensure accurate monitoring of treatment compliance, the device was set to automatically record the date and time of each treatment session and to transmit this data to a central server via the Internet. If a participant failed to log into the system for two consecutive days, an automated reminder message was sent to both the participant and their supervisor to enhance adherence. Treatment compliance was calculated as the percentage of completed sessions relative to the total number of prescribed sessions (two sessions per day, seven days per week) over the entire treatment period, based on data from the device's automated diary function. Additionally, the server continuously monitored the device's power output. In the event of unexpected fluctuations, the device was remotely deactivated to ensure safety.
Low-concentration atropine (0.01%) was prepared by the pharmacy department in Chongqing General Hospital. In the hospital preparation center, within the purification workshop, a trace amount of ethyl paraben was added to sterile physiological saline to prepare a 0.02% ethyl paraben solution. Atropine sulfate injection was diluted into the eye drop solvent to achieve a final concentration of 0.01% atropine solution. Sampling was conducted in accordance with the requirements of the Chinese Pharmacopoeia (2020 edition) for content determination. After passing the content test, the solution underwent sterilization. The prepared atropine eye drops were then recrimped and subjected to moist heat sterilization at 121 °C for 15 min, followed by natural cooling. In the Class 100 clean area of the preparation center's purification workshop, a sterile high-precision disposable infusion set was inserted into the butyl rubber stopper of a large infusion bottle under a laminar flow hood, allowing the solution to drip naturally into low-density polyethylene eye drop bottles sterilized with ethylene oxide. Once the filling volume reached the 8 mL mark, the bottles were stoppered, capped, and screw-locked. The entire process strictly adhered to aseptic techniques. After labeling, the bottles were packaged into sealed bags using a film-wrapping machine, completing the preparation.
The comparison group received 0.01% atropine eye drops in both eyes at bedtime every day. Participants were instructed to wear single-vision spectacles throughout the study. During the treatment period, if a participant's myopia progressed by > 0.5D, new spectacles based on appropriate prescription were provided.
Measurements
-
All measurements were obtained from both eyes at the initial visit, and at 1, 3, 6, and 12 months. All evaluations were performed from 9 to 11 am to avoid diurnal variation. Cycloplegia was conducted with 1 drop of 0.5% Alcaine (Alcon) followed by 1% cyclopentolate (Alcon, Geneva, Switzerland) 5 min apart, three times. Pupil light reflex and pupil diameter were checked to confirm full cycloplegia after an additional 30 min. Dilation and light reflex status were recorded, and full cycloplegia was justified if the pupil dilated to 6 mm or more and the light reflex was absent. Cycloplegic autorefraction was performed using the autorefractor (Nidek ARK-510A; Nidek, Gamagori, Japan). At least three readings, less than 0.25D apart in spherical or cylindrical power, were recorded. The average of these three readings was used in the analysis. SER was calculated as spherical power plus half of the cylinder power. Ocular biometric parameters, such as axial length (AL) and corneal curvature (CC), were measured using the Zeiss IOL-Master 500 (Carl Zeiss Meditec, Inc., Dublin, CA) before cycloplegia, for the flattest and steepest CCs. The average ALs of at least five measurements with ≤ 0.05 mm difference were recorded. Average CC was recorded as the mean of the flattest and steepest CCs. Corneal astigmatism was defined as the absolute difference between the K1 and K2 values.
Swept-source optical coherence tomography (SS-OCT) (DRI-OCT Triton, Topcon) was used for choroidal imaging. The SS-OCT machine used in the present study was equipped with a light source of 1,050 µm wavelength and a scanning speed of 100,000 A-scans per second, with which a depth resolution of 8 µm and a lateral resolution of 10 µm of ocular tissue were reached. Before recording the image by SS-OCT scanning, the spherical power diopter, cylindrical power diopter, and AL, using which the SS-OCT machine calculated the scan circle size, were input to minimize the error caused by the magnification factors associated with AL. The device operator adjusted the focus settings to the specific eye model of each participant before scanning. The scan protocol used the 12-line radial scan pattern with a resolution of 1,024 × 12 centered on the fovea. All measurements in the optical coherence tomography (OCT) images were acquired by a single experienced technician at each center. Images with a signal strength index of ≤ 60 were excluded. The borderlines of layers were identified using the built-in software, which segmented each layer automatically. Manual adjustments were performed whenever inaccurate auto-segmentation of each layer led to measurement artifacts. The subfoveal choroidal thickness (SFChT) was determined as the distance from the outer border of the retinal pigment epithelium (RPE) to the inner border of the chorioscleral interface in the subfoveal region, and was measured manually by two OCT technicians independently using the software provided by the OCT system. The mean of the two values taken by the OCT technicians was recorded as the final value and used for statistical analyses. To ensure the reproducibility of the SFChT measurements by the two observers, both technicians read randomly selected images from 20 eyes in advance. The interobserver correlation of average measures for SFChT was 0.98. Bland–Altman analysis (Supplementary Fig. S1) was used to calculate the interobserver agreement. The mean difference of SFChT measurements in 117 right eyes between the 2 observers was −0.87 µm, and the 95% limits of agreement were −22.75 to 21.01 µm. The interobserver correlation was 98.3% (p < 0.001).
BCVA values were assessed using using a logarithmic visual acuity (VA) chart at a distance of 5 m. The examination protocol was the same as the one used in the Refractive Error Study in Children. Accommodation amplitude (AA), uncorrected visual acuity (UCVA), near VA, height, and weight were optional secondary outcomes assessed at the study centers. Participants (n = 53; RLRL group, n = 30; 0.01% atropine group, n = 23) enrolled at Chongqing General Hospital underwent these evaluations. The near point of accommodation was measured using a near-point rule while participants wore their best-corrected distance spectacle correction in a phoropter. Participants were instructed to move the target inward until the 20/25 print became persistently blurred, and accommodation amplitude was calculated as the reciprocal of the near-point of accommodation (in meters). UCVA was assessed using the same protocol as BCVA. Height and weight were measured with participants wearing light clothing and no shoes.
Sample size
-
Based on previously published data, the mean annual AL progression in children 4 to 12 years old who received the treatment of 0.01% atropine was 0.36 mm (standard deviation, 0.29 mm)[8]. We estimated the RLRL group to have a 50% treatment effect (reducing the axial elongation by 0.18 mm). With an α level of 0.05 and 90% power, the sample size required was 56 subjects per group or 112 participants in total. Adjusting for a 10% loss to follow-up yielded a total sample size of 128 participants.
Statistical analysis
-
Longitudinal mixed models were used to demonstrate the treatment efficacy in terms of the primary outcome (changes in AL) and secondary outcomes (changes in SER and SFChT) on multiple follow-up visit time points. Treatment efficacy was calculated by dividing the between-arm difference in values by the control-arm value. An unstructured covariance matrix was used along with a restricted maximum likelihood method, in which the group, visit, and group-by-visit interaction were added as fixed effects together with baseline age, sex, and baseline AL as covariates. The participants were included as a random factor. Right eyes were used as the outcome data representing the participant. Missing data at the specific follow-up visits were not imputed because linear mixed-effect models still provide valid results when data are missing at random. All of the analyses were conducted using Stata 16 (Stata Corp, College Station, TX), and two-sided p < 0.05 was considered statistically significant. Only the SER data with full cycloplegia were used for the analysis to ensure accuracy on refraction measurement. To measure the associations between treatment efficacy and treatment compliance in the intervention group, we used a further longitudinal mixed model in which treatment compliance in the intervention group was estimated as a percentage of the total number of assigned treatment sessions.
Changes in UCVA (an ordinal variable) were categorized into 3 groups: worsening of 2 lines or more, no change (within 1 line), and improvement of 2 lines or more. All adverse events were reported individually in detail. Two ophthalmologists (Y.TS. and Z.N.) independently reviewed all OCT scans to identify possible structural damages.
-
Between November 2021 and July 2022, children with myopia (n = 139) were recruited and assessed for eligibility at 2 study sites. A total of 128 children were included in the study, with 69 children with myopia randomly assigned to the RLRL group and 59 children randomly assigned to the 0.01% atropine group by simple random sampling. Enrollment was ceased when the predefined sample size was achieved. Some participants did not complete all follow-up visits because of the coronavirus disease 2019 pandemic. Of 128 included children, 109 (85.2%) completed the 12-month study. A total of 117 participants who completed at least three follow-up visits were included in the analysis, consisting of 64 children in the RLRL group and 53 children in the 0.01% atropine group.
The baseline demographic and ocular characteristics of participants by treatment group are provided in Table 1. Overall, mean age and gender, baseline SER, AL, IOP, UCVA, AA, and body mass index (BMI) were similar in the RLRL and 0.01% atropine groups.
Table 1. Demographics and baseline ocular characteristics between the RLRL group (650 nm) and the low-concentration atropine group (0.01%).
Characteristics RLRL group (650 nm) (n = 64) Low-concentration atropine group (0.01%) (n = 53) p-Value Age (y), median (IQR) 9.00 (8.00, 10.00) 9.00 (8.00, 10.00) 0.98 Female, no (%) 32 (50.0) 26 (49.1) 0.99 SER (D), median (IQR) −2.25 (−3.03, −1.38) −2.00 (−2.75, −1.50) 0.81 AL (mm), median (IQR) 24.56 (23.78, 24.97) 24.15 (23.72, 24.66) 0.18 IOP (mmHg), mean ± SD 16.93 ± 2.65 17.21 ± 2.97 0.59 SFChT (μm), mean ± SD 244.84 ± 54.04 253.96 ± 52.98 0.36 UCVA (logMAR), median (IQR) 0.25 (0.15, 0.40) 0.25 (0.15, 0.30) 0.79 AA(D), mean ± SD 15.23 ± 3.76 15.92 ± 3.25 0.49 BMI (kg/m2), mean ± SD 18.15 ± 2.33 17.36 ± 2.47 0.24 Categorical variables are described by the number of subjects (percentage). Continuous variables with a normal distribution are described by mean ± SD. Continuous variables without a normal distribution are described by median (IQR). p-Values were calculated on the basis of unpaired t-tests for continuous data and chi-square tests for categorical data. AL = axial length; D = diopter; IOP = intraocular pressure; logMAR = logarithm of the minimum angle of resolution; SER = spherical equivalent refraction; UCVA = uncorrected visual acuity; AA = accommodation amplitude; BMI = body mass index; SFChT = subfoveal choroidal thickness. Primary outcome: axial elongation control
-
After adjusting for age, sex, baseline AL, treatment group, visit, and group-by-visit interactions, the 12-month mean axial elongation was −0.05 mm (95% confidence interval [CI], −0.09 to −0.01 mm) in the RLRL group, compared with 0.37 mm (95% CI, 0.33 to 0.41 mm) in the 0.01% atropine group. The mean difference in axial elongation between the RLRL and 0.01% atropine groups was 0.42 mm (95% CI, 0.36 to 0.47 mm; p < 0.01), reflecting a 113.5% reduction in myopia progression in the RLRL group relative to the atropine group. Adjusted axial elongation values at 1, 3, and 6 months for each group, along with mean differences between groups, are presented in Fig. 2 and Table 2. The longitudinal mixed-effects model revealed that baseline age, visit, and group-by-visit interactions were significantly associated with changes in AL, whereas treatment group, sex, and baseline AL were not significant predictors of AL progression (Table 3). Subgroup analysis based on baseline AL revealed a threshold-dependent predictive pattern (Supplementary Table S1). In children with baseline AL ≤ 24 mm, the adjusted mean AL change was 0.07 mm (95% CI: 0.00 to 0.13) in the RLRL group vs. 0.42 mm (0.36 to 0.49) in the atropine group (mean difference −0.36 mm, p < 0.001). For children with baseline AL between 24 and 25 mm, the RLRL group showed a mean AL shortening of −0.11 mm (−0.17 to −0.05) compared to a 0.34 mm (0.27 to 0.41) elongation in the atropine group (mean difference −0.45 mm, p < 0.001). In children with baseline AL > 25 mm, RLRL therapy also induced AL shortening (−0.14 mm, 95% CI: −0.21 to −0.06), while the atropine group showed 0.26 mm (0.17 to 0.35) elongation (mean difference −0.40 mm, p < 0.001). These findings indicate that a longer baseline AL (>24 mm) is associated with actual AL shortening under RLRL therapy, whereas the overall linear regression (Table 3) did not detect a significant association due to the relatively narrow distribution of baseline AL in the study population.
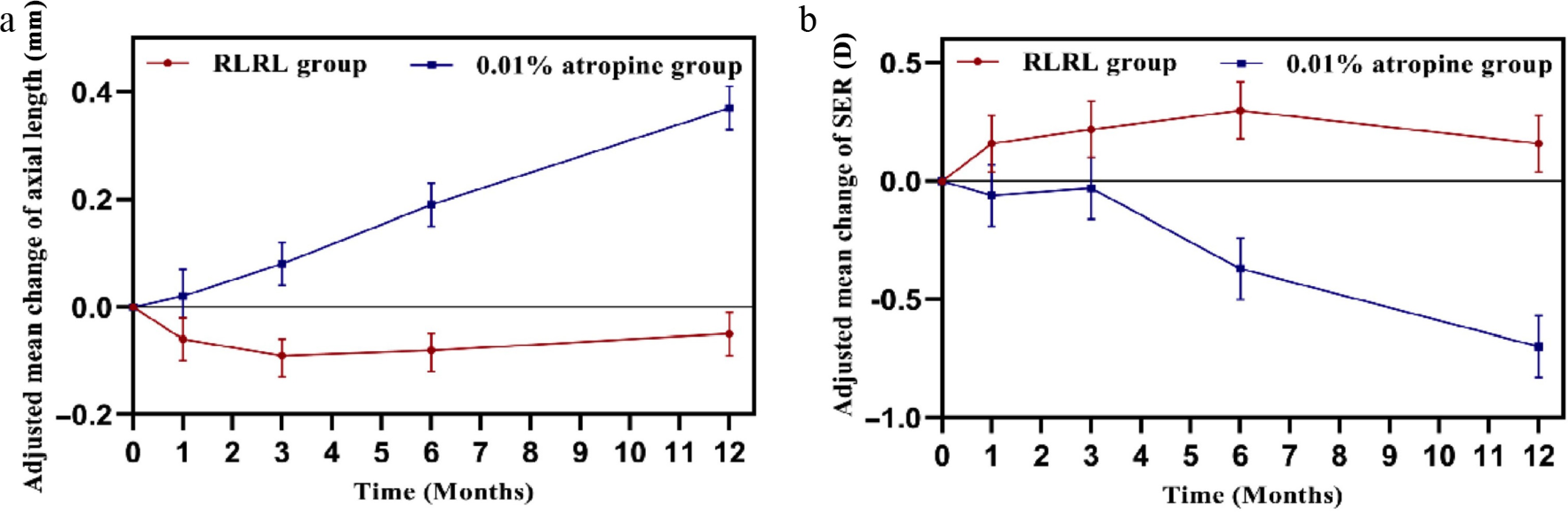
Figure 2.
Line graphs showing the adjusted mean changes in (a) axial length (after adjusting for age, sex, time, treatment group, visit*group, and baseline AL) and (b) cycloplegic spherical equivalent refractions (SERs) (after adjusting for age, sex, time, treatment group, visit*group, and baseline SER) from baseline to 12 months at each time point between the RLRL group and the 0.01% atropine group. D = diopter.
Table 2. Cumulative adjusted mean changes in axial length and cycloplegic spherical equivalent refraction from baseline to 12 months at each timepoint between RLRL group and 0.01% atropine group.
Time/visit Cumulative adjusted mean (95% CI) Mean difference (95% CI) p-Value RLRL group 0.01% atropine group Number of subjects 64 53 Change of AL (mm) 1 month −0.06 (−0.10 to −0.02) 0.02 (−0.02 to 0.07) −0.09 (−0.14 to −0.03) < 0.01 3 months −0.09 (−0.13 to −0.06) 0.08 (0.04 to 0.12) −0.18 (−0.23 to −0.12) < 0.01 6 months −0.08 (−0.12 to −0.05) 0.19 (0.15 to 0.23) −0.27 (−0.33 to −0.22) < 0.01 12 months −0.05 (−0.09 to −0.01) 0.37 (0.33 to 0.41) −0.42 (−0.47 to −0.36) <0.01 Change in SER (D) 1 month 0.16 (0.04 to 0.28) −0.06 (−0.19 to 0.07) 0.22 (0.04 to 0.40) 0.02 3 months 0.22 (0.10 to 0.34) −0.03 (−0.16 to 0.10) 0.24 (0.06 to 0.42) 0.01 6 months 0.30 (0.18 to 0.42) −0.37 (−0.50 to −0.24) 0.67 (0.49 to 0.85) < 0.01 12 months 0.16 (0.04 to 0.28) −0.70 (−0.83 to −0.57) 0.86 (0.68 to 1.04) < 0.01 Mean difference = change of variable in the 0.01% atropine group − change of variable in the RLRL group; AL = axial length; D = diopter; SER = spherical equivalent refraction; CI = confidence interval. Two-tailed t-tests were applied to the estimated mean differences at each time point, with degrees of freedom estimated by the Kenward–Roger method and two-tailed p-values computed from the t-distribution. Table 3. Mixed-model analysis of factors and effects on changes of axial length and cycloplegic spherical equivalent refraction.
Factors Coefficient (95% CI) p-Value Primary outcome Change in AL, mm Age, year −0.024 (−0.038 to −0.010) 0.002 Gender(M/F) 0.013 (−0.030 to 0.056) 0.566 Baseline AL, mm −0.024 (−0.050 to 0.002) 0.776 Group (RLRL/0.01% atropine) −0.034 (−0.096 to 0.027) 0.274 Time (visits) −0.105 (−0.132 to −0.077) <0.001 Interaction of group and time 0.109 (0.091 to 0.127) <0.001 Secondary outcome Change in SER, D Age, year 0.049 (0.008 to 0.901) 0.023 Gender (M/F) −0.039 (−0.163 to 0.085) 0.546 Baseline SER, D −0.072 (−0.127 to −0.018) 0.012 Group (RLRL/0.01%atropine) 0.092 (−0.115 to 0.299) 0.389 Time (visits) 0.245 (0.143 to 0.348) <0.001 Interaction of group and time −0.236 (−0.303 to −0.169) <0.001 CI = confidence interval, AL = axial length; D = diopter; SER = spherical equivalent refraction. Adjusted estimates at each time point were calculated on the basis of longitudinal mixed models, adjusted for baseline age, gender, group, group × visit, and the corresponding baseline parameter as fixed factors, and subjects as the random factor. Multiple comparisons with sequential Bonferroni adjustment were performed. Secondary outcomes
-
After adjusting for age, sex, baseline SER, treatment group, visit, and group-by-visit interactions, the 12-month mean SER progression was 0.16D (95% CI, 0.04 to 0.28D) in the RLRL group, compared with −0.70D (95% CI, −0.83 to −0.57D) in the 0.01% atropine group. The mean difference in SER progression between the RLRL and 0.01% atropine groups was 0.86D (95% CI, 0.68 to 1.04D; p < 0.01), representing a 122.9% reduction in myopia progression in the RLRL group relative to the atropine group. Adjusted SER progression values at 1, 3, and 6 months for each group, along with mean differences between groups, are presented in Fig. 2 and Table 2. The longitudinal mixed-effects model revealed that baseline age, baseline SER, visit, and group-by-visit interactions were significantly associated with changes in SER, whereas sex and treatment group were not significant predictors of SER progression (Table 3).
Adjusted 12-month changes in SFChT showed significant intergroup differences: +21.09 µm (95% CI, 12.82 to 29.36) in the RLRL group vs. −15.60 µm (95% CI, −24.69 to −6.51) in the atropine group. The intergroup difference in SFChT change was 36.70 µm (95% CI, 24.39 to 49.00; p < 0.001). Temporal profiles of adjusted SFChT measurements at 1, 3, and 6 months for both cohorts, with corresponding between-group differences, are shown in Fig. 3 and Table 4. Notably, CC showed no significant longitudinal changes at 12 months (Table 4).
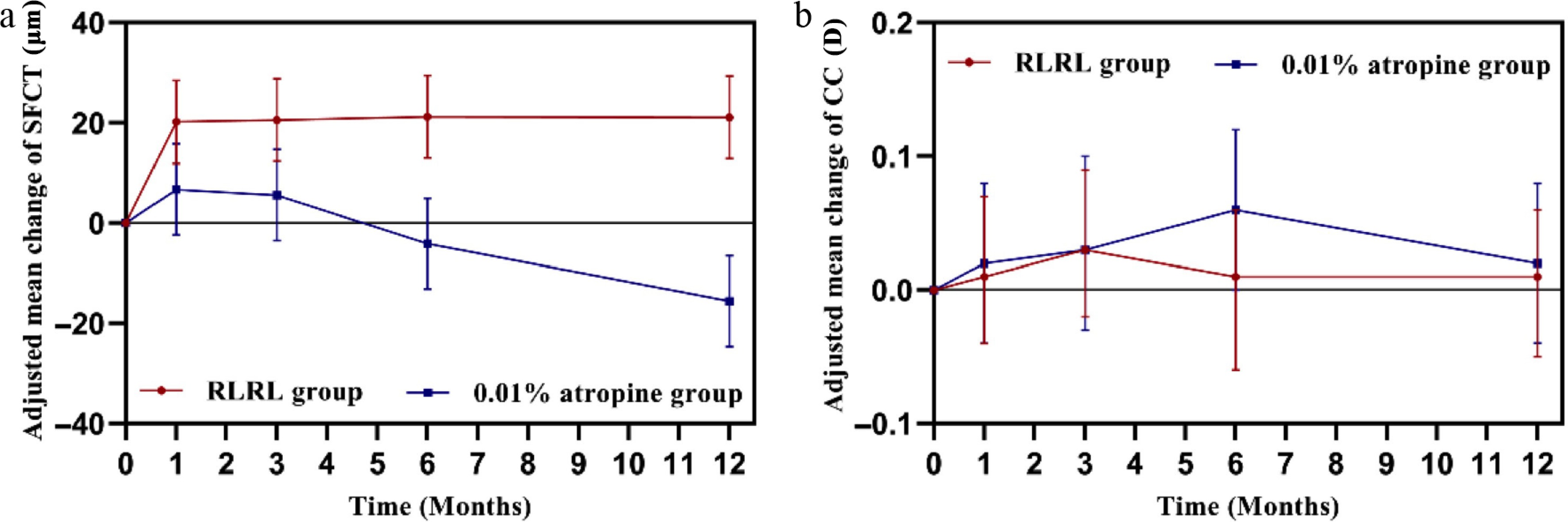
Figure 3.
Line graphs showing the adjusted mean changes in (a) subfoveal choroidal thickness (SFChT) (after adjusting for age, sex, time, treatment group, visit*group, and baseline SFChT). (b) Corneal curvature (CC) (after adjusting for age, sex, time, treatment group, visit*group, and baseline CC) from baseline to 12 months at each time point between the RLRL group and the 0.01% atropine group.
Table 4. Cumulative adjusted mean changes in subfoveal choroidal thickness and cycloplegic spherical equivalent refraction from baseline to 12 months at each timepoint between the RLRL group and the 0.01% atropine group.
Time/visit Cumulative adjusted mean (95% CI) Mean difference (95% CI) p-Value RLRL group 0.01% atropine group Number of patients analyzed 64 53 Change in subfoveal choroidal thickness (μm) 1 month 20.20 (11.93 to 28.47) 6.73 (−2.36 to 15.82) 13.50 (1.17 to 25.8) 0.032 3 months 20.54 (12.27 to 28.81) 5.59 (−3.50 to 14.68) 14.94 (1.17 to 25.8) 0.018 6 months 21.26 (12.99 to 29.53) −4.11 (−13.20 to 4.98) 25.4 (13.06 to 37.7) < 0.001 12 months 21.09 (12.82 to 29.36) −15.60 (−24.69 to −6.51) 36.7 (24.39 to 49.0) < 0.001 Change in CC (D) 1 month 0.01 (−0.04 to 0.07) 0.02 (−0.04 to 0.08) −0.01 (−0.09 to 0.07) 0.832 3 months 0.03 (−0.02 to 0.09) 0.03 (−0.03 to 0.10) −0.003 (−0.086 to 0.080) 0.944 6 months 0.01 (−0.06 to 0.06) 0.06 (−0.00 to 0.12) −0.054 (−0.137 to 0.029) 0.198 12 months 0.01 (−0.05 to 0.06) 0.02 (−0.04 to 0.08) −0.012 (−0.096 to 0.070) 0.759 CI = confidence interval, D = diopter; CC = corneal curvature. Two-tailed t-tests were applied to estimate the mean differences at each time point, with degrees of freedom estimated by the Kenward–Roger method and two-tailed p-values computed from the t-distribution. At 12 months, significantly more RLRL-treated myopic children demonstrated ≥ 2 lines of UCVA improvement compared to the 0.01% atropine group (33.33% vs. 8.69%; p = 0.003, Supplementary Table 2). Both cohorts achieved comparable best-corrected visual outcomes, with 100% of children in each group attaining BCVA ≤ 0.0 logMAR (p > 0.05). No ocular hypertension occurred during follow-up, and clinically significant IOP fluctuations (≥ 5 mmHg from baseline) occurred at similar rates between groups (21.87% vs. 20.8%; p > 0.05, Supplementary Table S2).
Near visual function showed no significant intergroup differences over the 12-month period (Table 5). Accommodation amplitude diverged significantly between groups only at the 1-month assessment (RLRL vs. 0.01% atropine; p < 0.05), with no subsequent timepoints showing statistically significant differences (Table 5).
Table 5. Cumulative adjusted mean changes in near VA (logMAR) and accommodation amplitude from baseline to 12 months at each timepoint in the RLRL group and the 0.01% atropine group.
RLRL group (n = 30) 0.01% atropine group (n = 23) Mean difference (95% CI) p-Value Near VA Change at 1 month −0.016 (−0.038 to −0.005) 0.004 (−0.021 to 0.029) −0.020 (−0.054 to 0.013) 0.236 Change at 3 months −0.023 (−0.045 to −0.001) −0.022 (−0.047 to −0.003) −0.001 (−0.034 to 0.033) 0.968 Change at 6 months −0.030 (−0.051 to −0.008) −0.035 (−0.060 to −0.010) 0.006 (−0.028 to 0.039) 0.736 Change at 12 months −0.026 (−0.048 to −0.005) −0.009 (−0.034 to 0.016) −0.017 (−0.050 to 0.016) 0.314 Accommodation amplitude, D Change at 1 month 1.185 (0.037 to 2.334) −1.321 (−2.634 to −0.008) 2.506 (0.751 to 4.260) 0.005 Change at 3 months −0.266 (−1.413 to 0.882) −0.888 (−2.201 to 0.425) 0.622 (−1.133 to 2.380) 0.483 Change at 6 months −0.646 (−1.794 to 0.502) −0.854 (−2.167 to 0.459) 0.208 (−1.547 to 1.960) 0.814 Change at 12 months −1.868 (−3.017 to −0.720) −1.621 (−2.934 to −0.308) −0.247 (−2.002 to 1.510) 0.781 VA = visual acuity; RLRL = repeated low-level red-light; CI = confidence interval. Two-tailed t-tests were applied to estimate the mean differences at each time point, with degrees of freedom estimated by the Kenward–Roger method and two-tailed p-values computed from the t-distribution. Degree of axial elongation and myopia progression
-
Over the 12-month period, a significantly greater proportion of participants in the RLRL group exhibited minimal AL progression (≤ 0.1 mm) compared to the 0.01% atropine group (79.7% vs. 9.4%; p < 0.001; Supplementary Fig. S2). Conversely, rapid AL progression (≥ 0.36 mm) was markedly lower in the RLRL group (6.3% vs. 43.4%; p < 0.001; Supplementary Fig. S2). Similarly, a higher percentage of RLRL participants showed limited SER progression (≤0.5D) compared to the atropine group (93.8% vs. 47.2%; p = 0.001; Supplementary Fig. S2), with no RLRL participants exhibiting significant SER progression (> 1.0D) compared to 17.0% in the atropine group (p = 0.001; Supplementary Fig. S2). Notably, 48.4% (31/64) of the myopic children in the RLRL group achieved AL shortening (> 0.05 mm) at the 1-month follow-up, exceeding the threshold for measurement error using the IOL-Master 500. The corresponding proportions of clinically significant AL shortening at 3, 6, and 12 months were 59.4%, 64.1%, and 50.0%, respectively.
Treatment compliance and treatment efficacy
-
The median treatment compliance in the RLRL group was 79.88% (68.21% and 85.14%, respectively, in each center). Participants with a treatment compliance rate of 100% carried out the treatment 7 days per week. The median adherence rate of 79.88% was defined as the clinical efficacy threshold based on the observed dose–response relationship. The 0.01% atropine group was used as the reference because it represents standard clinical practice for myopia control, providing a well-established benchmark for comparing the efficacy of RLRL therapy. The dose–response relationship between treatment compliance with RLRL and efficacy in controlling myopia progression and AL reduction is shown in Supplementary Table S3 and Supplementary Fig. S3.
Treatment compliance was derived from automated device logs, calculated as the percentage of completed sessions relative to prescribed sessions (twice daily, seven days weekly). For AL outcomes, the 0.01% atropine cohort (n = 53; mean change 0.369 ± 0.228 mm) served as the efficacy benchmark. Similarly, for SER comparisons we used the atropine group data (n = 53; mean progression −0.705 ± 0.481D) as reference. Treatment efficacy was quantified using the formula
$ \mathrm{Treatment\; efficacy=\dfrac{Value_{RLRL}-Value_{0.01\text{%}Atropine}}{Value_{0.01\text{%}Atropine}}}. $ Adverse events
-
No serious adverse events occurred during the 12-month follow-up period. Five RLRL participants withdrew from treatment owing to the following reasons: ocular discomfort (n = 1), boarding school restrictions preventing treatment access (n = 1), non-compliance with treatment protocol (n = 2), and decision to switch to DIMS spectacles (n = 1). Six atropine group participants discontinued treatment for the following reasons: rapid myopia progression (n = 3), loss to follow-up (n = 2), and transition to orthokeratology (n = 1). SS-OCT revealed no pathological macular alterations in any study participant.
Sensitivity and subgroup analyses
-
Per-protocol sensitivity analyses confirmed the robustness of primary outcomes, yielding consistent results. Subgroup analyses were performed to evaluate the myopia control efficacy (axial elongation and SER progression) stratified by baseline refractive status and age. Children with lower baseline myopia (SER −1.00 to −2.99D) or younger age (6−10 years) exhibited accelerated progression in the 0.01% atropine group. In contrast, RLRL therapy effectively controlled myopia progression in these subgroups. Although greater efficacy was observed in children with higher baseline myopia (≤ −3.00D) and older age (11−12 years) receiving RLRL, both subgroups demonstrated clinically significant treatment responses (Supplementary Table S4).
-
This multicenter RCT compared RLRL therapy with 0.01% atropine for myopia control and found that RLRL significantly slowed AL elongation and SER progression over 1, 3, 6, and 12 months compared with 0.01% atropine. Compared with 0.01% atropine, RLRL treatment slowed AL elongation by 0.42 mm and progression of myopic SER by 0.86D. Our results suggest that RLRL might have better efficacy for myopia control than 0.01% atropine.
The efficacy of RLRL has been reported in previous studies. The 2022 multicenter RCT conducted by Jiang et al.[14] reported adjusted axial elongation in the RLRL group at 1, 3, and 6 months as −0.04, −0.01, and 0.13 mm, respectively. Our study observed corresponding values of −0.06, −0.09, and −0.05 mm. Although axial control efficacy was comparable during the first three months, our RLRL group demonstrated significantly enhanced suppression of axial elongation beyond this period. Despite the RLRL devices having identical parameters (650 nm, ~1,600 lx), the treatment frequency differed (7 days/week in our study vs. 5 days/week in the study by Jiang et al.[14]). Moreover, the age range of our cohort (6–12 years) was not identical to that of Jiang et al.[14] (8–13 years). Thus, the observed differences may be attributable to age-related variations in myopia progression or adherence, rather than frequency alone. Further studies directly comparing different frequencies within the same age group and device settings are needed to isolate the effect of treatment frequency.
Refractive outcomes showed similar trends. Jiang et al. documented adjusted SER progression values of 0.08, 0.07, and −0.20D at the same intervals, whereas our cohort exhibited 0.16, 0.22, and 0.16D. These findings suggest that daily RLRL administration may provide more sustainable control of both axial elongation and refractive progression.
In the overall cohort, baseline AL was not significantly associated with AL progression (Table 3), whereas baseline SER showed a significant association with SER progression. This discrepancy can be explained by the distribution characteristics of the two parameters. Baseline AL values were concentrated within a relatively narrow range (approximately 23–26 mm), which limits the statistical power to detect a linear relationship. In contrast, baseline SER exhibited a much wider spread (from −6D to 0), making it more sensitive to linear associations. However, when we stratified the baseline AL into clinically meaningful subgroups (≤ 24, 24–25, and >25 mm), a clear threshold-dependent predictive pattern emerged: children with baseline AL > 24 mm consistently showed AL shortening under RLRL therapy, whereas those with AL ≤ 24 mm did not. This suggests that baseline AL is a valuable predictor of RLRL efficacy, but the relationship is categorical rather than strictly linear. Therefore, clinicians may use a baseline AL cutoff of 24 mm to identify children who are more likely to achieve axial shortening with RLRL therapy.
This study directly compared RLRL with low-dose atropine, providing evidence that corroborates the findings from previous single-center studies[15,16]. Our results demonstrate a superior effect of RLRL in slowing axial elongation over one year compared to 0.01% atropine, with a between-group difference of 0.11 mm (–0.09 vs. +0.02 mm). This finding aligns with the 0.10 mm difference reported in the single-center RCT by Chen et al.[16] and the 0.17 mm cumulative difference over two years in the retrospective study by Zhang et al.[17]. The consistency of this treatment effect across multiple clinical sites in our study enhances the generalizability of the conclusion. Given the well-established concentration-dependent response of atropine, we compared the efficacy of 0.05% atropine with RLRL therapy. In the LAMP study, 0.05% atropine resulted in a mean annual SER progression of −0.27 ± 0.61D and AL elongation of 0.20 ± 0.25 mm in myopic children over 1 year[8]. Indirect comparisons with studies on higher atropine concentrations (e.g., 0.05% atropine in the LAMP study) are not conclusive but suggest that RLRL may have comparable efficacy. Further head-to-head trials are needed to directly compare RLRL with 0.05% atropine. Furthermore, our data on the significantly greater increase in SFChT in the RLRL group (+15.2 vs. +5.8 µm) are in agreement with the work of Peng et al.[18] and Shang et al.[19], who reported similar improvements in choroidal and retinal vascular parameters. This suggests a distinct mechanistic pathway for RLRL, potentially involving enhanced choroidal blood flow, which is not a primary mechanism of action for atropine. The crossover trial by Pang et al.[15], which found a 40% improvement in AL control after switching from atropine to RLRL, provides a rationale for future investigations into sequential or combination therapy.
In the overall cohort, baseline AL was not significantly associated with AL progression (Table 3), whereas baseline SER showed a significant association with SER progression. This discrepancy can be explained by the distribution characteristics of the two parameters. Baseline AL values were concentrated within a relatively narrow range (approximately 23.0–26.0 mm), which limits the statistical power to detect a linear relationship. In contrast, baseline SER exhibited a much wider spread (from −6.0 to −1.0D), making it more sensitive to linear associations. However, when we stratified baseline AL into clinically meaningful subgroups (≤ 24, 24–25, and > 25 mm), a clear threshold-dependent predictive pattern emerged: children with baseline AL > 24 mm consistently showed AL shortening under RLRL therapy, whereas those with AL ≤ 24 mm did not. This suggests that baseline AL is a valuable predictor of RLRL efficacy, but the relationship is categorical rather than strictly linear. Therefore, clinicians may use a baseline AL cutoff of 24 mm to identify children who are more likely to achieve axial shortening with RLRL therapy.
Myopia has traditionally been considered a progressive and irreversible ocular condition. AL shortening remains rarely observed following conventional myopia control interventions. Short-term AL reduction has been documented with orthokeratology, while previous studies (e.g., ATOM study) reported temporary AL shortening of −0.14 ± 0.28 mm after 1 year and −0.02 ± 0.35 mm after 2 years in subjects using 1% atropine[20].
By contrast, AL shortening represents a notable phenomenon following RLRL therapy. Both Jiang et al. and Wang et al. have documented axial shortening in myopic children receiving RLRL treatment[14,21]. Among subjects with −1.0 to −5.0D myopia, we observed negative adjusted mean AL changes at both 1- and 3-month intervals. Notably, 21.6% of the RLRL-treated subjects exhibited an AL shortening of > 0.05 mm at 12 months despite an overall positive mean AL change.
Consistent with these findings, our RLRL cohort demonstrated sustained negative adjusted mean AL changes throughout follow-up, with 50% achieving >0.05 mm AL reduction at 12 months. Xu et al.[22] similarly reported persistent AL shortening (−0.06 mm at 1 month maintained through 12 months) in high myopes, with 53.3% exhibiting this effect.
We further measured SFChT changes. At 1 month, choroidal thickening averaged +20.20 μm (95% CI: 11.93 to 28.47 μm) alongside AL shortening of −0.06 mm (95% CI: −0.10 to −0.02 mm). This magnitude of AL reduction cannot be fully attributed to choroidal thickening, corroborating Xiong's finding of +15.97 μm (95% CI: 5.42 to 26.31 μm) macular choroidal thickness changes[23].
A time-point-specific summary of major RLRL studies is presented in Supplementary Table S5. Across studies, RLRL consistently induced early choroidal thickening accompanied by suppression of axial elongation and attenuation of myopic progression. In our study, subfoveal choroidal thickness increased by 20.20 μm at 1 month, 20.54 μm at 3 months, 21.26 μm at 6 months, and 21.09 μm at 12 months, while AL change remained negative throughout follow-up (−0.06, −0.09, −0.08, and −0.05 mm at 1, 3, 6, and 12 months, respectively). Similar temporal patterns were observed in the studies of Jiang et al.[14] and Xiong et al.[23], in which early choroidal thickening and axial shortening were followed by sustained, although less pronounced, control over time.
Although atropine has also been reported to increase choroidal thickness, our results suggest that this effect may be time-dependent and not sustained. In the present study, the 0.01% atropine group showed choroidal thickening at 1 and 3 months, followed by thinning at 6 and 12 months. This temporal pattern is broadly consistent with recent evidence indicating that atropine induces significant choroidal thickening early in treatment, whereas the long-term differences in choroidal thickness compared with controls may no longer remain statistically significant[24]. By contrast, the inhibitory effect of atropine on axial elongation appears to be more consistent over time. These findings suggest that choroidal change may be an early biomarker or partial mediator of atropine treatment, but not its sole or sustained mechanism of myopia control.
Animal studies suggest that RLRL may increase choroidal blood flow[25]. Given the recent evidence implicating scleral hypoxia in scleral remodeling and myopia progression[26,27], we hypothesize that RLRL ameliorates scleral hypoxia and restores collagen synthesis through enhanced fundal perfusion and metabolic activity. Further mechanistic studies are warranted to validate this pathway.
The mechanisms by which RLRL therapy may suppress myopia progression are likely multifactorial and can be discussed, at least in part, through the framework of photobiomodulation (PBM). At the cellular level, PBM has been associated with mitochondrial activation, enhanced antioxidative capacity, and modulation of inflammatory signaling. By acting on mitochondrial cytochrome c oxidase, red-light absorption is proposed to initiate downstream signaling involving nitric oxide (NO), adenosine triphosphate (ATP), calcium ions, and reactive oxygen species (ROS)[28]. These molecular shifts are reported to inhibit hypoxia-inducible factor 1α (HIF-1α) expression and promote scleral collagen synthesis, thereby reinforcing the structural integrity of the posterior pole[29].
From a visual neuroscience perspective, multiple animal models support the anti-myopic potential of red light, although species differences and light parameters matter. In the mudpuppy retina, sufficiently bright red light (620 nm) triggers the uncoupling of horizontal cells via dopamine release, a classic neuromodulatory mechanism that signals light adaptation and reduces retinal gain[30]. Dopamine is a key stop signal for axial elongation, linking ambient light conditions to eye growth. In mammals such as tree shrews and rhesus monkeys, pure narrow band and filtered red light consistently induces hyperopic shifts, shortens the vitreous chamber, and thickens the choroid[31,32]. This effect may arise from red light creating a chronic "myopic defocus" signal through longitudinal chromatic aberration, biasing emmetropization toward hyperopia. However, the hyperopic effect is easily diluted by white light contamination, requires a minimum intensity (≥ 50 to 100 lx)[31], and may have species variability. Despite these caveats, convergent evidence from multiple models supports that red light, when delivered with adequate purity, intensity, and intermittent patterning, engages retinal dopaminergic pathways and chromatic cues to suppress axial elongation, providing a mechanistic foundation for clinical RLRL therapy.
Beyond these biochemical pathways, RLRL could plausibly confer neuroprotective benefits to the optic nerve, although this remains to be directly verified in future studies. In our study, RLRL was associated with increased choroidal thickness and improved perfusion-related parameters; experimental work in guinea pigs further supports that RLRL can influence choroidal thickness and blood flow responses[33]. Given the close vascular and metabolic coupling between the posterior pole and the optic nerve head (ONH), such hemodynamic changes may extend to the ONH and thereby support oxygen and nutrient delivery to retinal ganglion cell (RGC) axons, which have high metabolic demands[34]. This hypothesis is consistent with the concept that scleral hypoxia is involved in myopia-related remodeling and with evidence that reduced choroidal blood perfusion can induce myopia in animal models, together suggesting that improved oxygenation/perfusion might mitigate hypoxia-driven processes and potentially reduce secondary optic nerve vulnerability during myopic expansion[26,35].
The biomechanical implications of RLRL should also be considered. We observed marked suppression of axial elongation, including a small mean axial shortening (−0.05 mm). From a biomechanical perspective, limiting globe expansion may reduce the tensile load on the ONH and peripapillary lamina cribrosa, thereby potentially lowering the risk of traction-related stress on optic nerve fibers[36]. Taken together, these cellular, hemodynamic, and biomechanical pathways may act in concert, offering a broader therapeutic rationale for RLRL beyond refractive outcomes alone.
The efficacy of RLRL therapy in myopia control is strongly correlated with treatment compliance. Evidence indicates that increasing the compliance from 50% to ≥ 75% significantly enhances the control of AL and SER progression, with AL suppression improving from 44.6% to 76.8% and SER progression control rising from 41.7% to 87.7%. Lower compliance[14] is associated with reduced therapeutic outcomes.
In our study, participants with ≥80% compliance achieved a 121.68% greater AL suppression efficacy compared to 0.01% atropine, whereas those with <80% compliance showed a 106.22% improvement. This dose–response relationship shows RLRL's efficacy in myopia control and addresses the need for high adherence. Strategies to improve compliance, such as Internet-connected device monitoring, automated reminders, and parental supervision, hold promise but require further validation through controlled clinical trials.
Table 5 demonstrates a decline in accommodation amplitude (AA) in both treatment groups over the study period, a finding classically associated with the muscarinic antagonism of low-dose atropine. Interestingly, a similar although milder decline was also observed in the RLRL group, with the intergroup difference reaching statistical significance only at the 1-month follow-up and converging thereafter.
In our study, the AA measurement was performed using the conventional push-up method, in which participants moved a 20/25-equivalent target inward until persistent blur was reported, with amplitude calculated as the reciprocal of the near-point distance in meters. This subjective approach is prone to early measurement bias due to adaptation or mild discomfort[37].
Moreover, the indirect effects of RLRL on the ciliary muscle should also be considered. As discussed in Section 4.4, RLRL may engage retinal dopaminergic pathways, which are also known to regulate ciliary muscle tone[38]. This indirect neuromodulation could transiently reduce AA early in treatment, but the effect is expected to diminish over time as the eye adapts to the therapy. Importantly, the AA decline in the RLRL group remained clinically mild and did not result in reported visual symptoms or treatment discontinuations, supporting the overall favorable safety profile of this non-pharmacological intervention. These interpretations provide a balanced, mechanism-informed explanation for the observed pattern without altering the primary efficacy conclusions.
Given the concerns regarding potential retinal structural damage associated with RLRL therapy, it is essential to report the safety outcomes of our study. During the 12-month follow-up period, no serious adverse events occurred in any participant. The primary reasons for discontinuing RLRL in this study were related to operational burden and environmental constraints rather than treatment efficacy or safety concerns, whereas the main reasons for discontinuing atropine were insufficient efficacy (rapid progression) and follow-up burden (loss to follow-up) rather than direct side effects. Importantly, swept-source OCT revealed no pathological macular alterations in any study participant. In our recently published adaptive optics scanning laser ophthalmoscopy (AO-SLO) study in children after RLRL therapy, no significant decrease in cone photoreceptor density was found compared with untreated myopic controls[39]. These structural findings, together with the absence of severe clinical adverse events, provide supportive but preliminary evidence regarding the retinal safety of RLRL therapy under the treatment regimen used in our study. Nevertheless, longer-term follow-up, larger sample sizes, and multidimensional safety assessments—such as microperimetry and electroretinography—are warranted to further evaluate the safety profile of RLRL therapy in future studies.
This study has several limitations. (1) This was a single-blind study in which parents and children were aware of group assignments. Although outcome assessors were masked, the lack of participant masking may have introduced performance bias (e.g., differential adherence or expectation effects). (2) Compliance with atropine treatment was not quantitatively assessed. While some studies measure compliance by counting empty bottles, our center lacked access to single-dose atropine formulations, potentially reducing the reliability of our results. (3) All participants were recruited from a single center in Chongqing, China, which limits the generalizability of our findings to other geographic regions or ethnic populations. (4) The study compared RLRL therapy solely with 0.01% atropine. Given the well-established concentration-dependent efficacy of atropine in myopia control, future research should explore comparisons with higher concentrations, such as 0.05%. (5) The COVID-19 pandemic prolonged patient recruitment and led to increased loss to follow-up, particularly at 6 months. (6) The observed efficacy in controlling myopic progression is specific to the RLRL device used in this study. The effectiveness of alternative wavelengths, power intensities, exposure durations, or treatment frequencies remains unverified. (7) The 12-month follow-up duration limits insights into the long-term cumulative benefits of RLRL therapy, necessitating extended studies to confirm sustained efficacy.
-
This multicenter RCT demonstrates that RLRL therapy outperforms 0.01% atropine in controlling myopia progression, with 50% of RLRL-treated children showing > 0.05 mm AL shortening at 12 months. A key finding is that adherence plays a critical role: high compliance (≥ 80%) enhanced AL control by 121.68% compared to atropine, vs. 106.22% at < 80% compliance. Secondary findings include RLRL achieving better suppression of spherical equivalent refraction progression and fewer side effects than atropine. Clinically, strategies such as device connectivity and parental supervision may improve compliance, though these require validation. Limitations include unquantified atropine adherence, single-device use, and a 12-month follow-up. Longer studies with varied devices and higher atropine concentrations (e.g., 0.05%) are needed to confirm RLRL's long-term efficacy. RLRL proves to be an effective, well-tolerated myopia control option, supporting optimized clinical protocols.
-
All procedures adhered to the principles of the Declaration of Helsinki and were approved by the Ethics Committee of Chongqing General Hospital (KYS2021-011-01, May 28, 2021) and the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (2021-426, September 15, 2021). Written informed consent was obtained from the parents or legal guardians of all participants.
-
The authors confirm their contributions to the paper as follows: study conception and design: Yi H, Yi S, Zhang N; data collection: Yue Y, Xing L, Shui L; analysis and interpretation of results: Yue Y, Yi S, Yi T; draft manuscript preparation: Yue Y, Zhang N. All authors reviewed the results and approved the final version of the manuscript.
-
The datasets generated during and analyzed during the current study are available from the corresponding authors on reasonable request.
-
This study was funded by the National Natural Science Foundation of China (No. 82571201 and No. 81900845). We would like to thank the optometrists in the Ophthalmology Department for their assistance in collecting the basic ocular data of the participants at Chongqing General Hospital and the First Affiliated Hospital of Chongqing Medical University.
-
The authors declare that they have no conflict of interest.
-
accompanies this paper online at: https://doi.org/10.48130/vns-0026-0030.
-
Authors contributed equally: Yu Yue, Ni Zhang
- Supplementary Table S1 Subgroup analysis by baseline axial length (AL).
- Supplementary Table S2 One-year changes in UCVA, BCVA, and Fluctuation in IOP in the RLRL and 0.01% atropine groups.
- Supplementary Table S3 The efficacy of repeated low-level red-light therapy in controlling axial length and cycloplegic spherical equivalent refraction in different treatment compliance groups.
- Supplementary Table S4 Sensitivity analysis of adjusted mean changes in axial length and spherical equivalent refraction from baseline to 12 months between RLRL and 0.01% atropine groups, stratified by myopia severity (A) and age group (B).
- Supplementary Table S5 Time-point-specific summary of major RLRL studies reporting axial length and spherical equivalent refraction (A), and choroidal thickness outcomes (B).
- Supplementary Fig. S3
- Supplementary Fig. S1 The Bland-Altman plot represents the agreement between the choroid thickness measurements obtained by the two observers.
- Supplementary Fig. S2 Distribution of changes in AL(A) and SER(B) at 1 year for the RLRL and 0.01% atropine groups.
- Supplementary Fig. S3 The dose-response relationship between treatment compliance for repeated low-level red-light and change in axial length and SER.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Yue Y, Zhang N, Xing L, Shui L, Yi H, et al. 2026. Repeated low-level red light vs. 0.01% atropine for myopia control in children: a multicenter randomized controlled trial. Visual Neuroscience 43: e029 doi: 10.48130/vns-0026-0030 

Repeated low-level red light vs. 0.01% atropine for myopia control in children: a multicenter randomized controlled trial
- Received: 26 February 2026
- Revised: 25 May 2026
- Accepted: 26 May 2026
- Published online: 30 June 2026
Abstract: To compare the efficacy and safety of repeated low-level red-light (RLRL) therapy with that of low-concentration atropine (0.01%) for myopia control in children, a single-masked, two-center (Chongqing General Hospital and the First Affiliated Hospital of Chongqing Medical University), randomized controlled trial was conducted. Of the 128 enrolled children, 69 were assigned to the RLRL group (32 from Chongqing General Hospital and 37 from the First Affiliated Hospital of Chongqing Medical University) and 59 to the atropine group (24 and 35, respectively). After adjusting for age, sex, baseline axial length (AL), treatment group, visit, and group-by-visit interactions, the mean difference in axial elongation between the RLRL and 0.01% atropine groups among 117 participants was 0.42 mm (95% confidence interval [CI], 0.36 to 0.47 mm; p < 0.01). The mean difference in spherical equivalent refraction (SER) progression between the RLRL and 0.01% atropine groups was 0.86D (95% CI, 0.68 to 1.04D; p < 0.01). An increase in subfoveal choroidal thickness was observed with RLRL (+21.09 μm), while a a decrease was observed with atropine (–15.60 μm, p < 0.001). No functional visual loss or structural damage was observed in both groups. RLRL demonstrates superior efficacy for myopia control compared to 0.01% atropine, accompanied by a choroidal response and favorable safety profile. This study was registered in the Chinese Clinical Trial Registry (www.chictr.org.cn/showprojEN.html?proj=136525; ID: ChiCTR2100052653; Date of Registration: November 03, 2021).
-
Key words:
- Myopia /
- Red light therapy /
- Atropine