









-
The cornea represents the most densely innervated tissue in the human body. Corneal nerves play roles far beyond critical sensation. They regulate corneal epithelial homeostasis by releasing neurotrophic factors. Additionally, they activate brainstem circuits to mediate reflex tearing and blinking, and participate in preserving the overall ocular surface integrity. This intricate neural network serves as a critical mediator, facilitating bidirectional signaling between the corneal epithelium and stroma. This signaling is achieved primarily through the modulation of key neurotrophic factors. These factors, which include nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and neurotrophins 3 and 4 (NT-3, NT-4), are essential for promoting tissue repair and regeneration. Neurological dysfunction characterizes neurotrophic keratitis (NK). Upon epithelial injury, neighboring cells migrate to the lesion site to initiate re-epithelialization, thereby restoring the epithelial barrier. This repair process is mediated by epithelial–neuronal interactions, which orchestrate the resynthesis of damaged extracellular matrix, cell migration, and structural restoration. Compromised healing exposes the stroma to enzymatic degradation, potentially leading to melting and perforation[1].
Conventional treatments for Stage 2 NK include sodium hyaluronate eye drops, autologous serum, therapeutic contact lenses, etc. For severe cases, surgical interventions such as tarsorrhaphy, amniotic membrane transplantation, or botulinum toxin injection may be considered. However, these treatment modalities are associated with some risk of a recurrence of epithelial defects and inadequate regeneration of the corneal nerves[2]. Corneal neurotization is a treatment to promote nerve recovery, but it involves a large surgical wound. Consequently, pharmacological treatments that simultaneously promote corneal epithelial healing and nerve regeneration have emerged as a preferable therapeutic strategy. Recombinant human nerve growth factor (rh-NGF) has shown clinical efficacy and impact on corneal morphology and function, and is currently a significant focus of research. Studies report its efficacy in healing persistent epithelial defects (PEDs) and ulcers of diverse etiologies[3−6]. However, although the efficacy and safety of rh-NGF have been demonstrated in previous studies[7,8], data regarding its effects on corneal nerve regeneration and sensory recovery remain limited. This retrospective study therefore aimed to evaluate the long-term outcomes of rh-NGF therapy on corneal nerve structure and sensation in patients with NK.
-
This retrospective study was conducted at the Beijing Tongren Eye Center, Beijing Tongren Hospital, Capital Medical University. The retrospective study analyzed clinical data from 21 patients with Stage 2 NK according to the Mackie classification[9]. These patients received rh-NGF (Cenegermin, Dompé farmaceutici S.p.A., Milan, Italy) treatment between January 2021 and September 2022. This study complies with the Declaration of Helsinki. Ethical approval was granted by the Beijing Tongren Hospital Ethics Committee (Approval No. TREC2026-KY115), with written informed consent from all participants.
The inclusion criteria were aged > 18 years; with a clinical diagnosis of Grade 2 NK with impaired corneal sensitivity within the lesion area and in at least one corneal quadrant beyond the lesion margins, and baseline best corrected visual acuity (BCVA) in the affected eye of ≥ 0.2 LogMAR, demonstrated persistence of the PED without objective clinical improvement after at least 2 weeks of conventional therapy prior to initiating rh-NGF treatment; and their complete medical records and follow-up data were available at all the specified time points (baseline, Week 4, Week 8, and Week 56). The exclusion criteria were bilateral Grade 2 or 3 NK, active ocular infection or inflammation unrelated to NK at the time of treatment initiation, concurrent ocular infection (e.g., endophthalmitis), and concomitant ocular diseases in the affected eye, including but not limited to corneal ulcer perforation, glaucoma, uveitis, or autoimmune-associated peripheral keratitis.
A brief summary of the baseline demographic characteristics and etiology is as follows. In total, 21 patients were included, aged 22 to 85 years (mean: 56.00 ± 14.04 years). There were 11 female patients (52.4%) and 10 male patients (47.6%). All patients were of Chinese ethnicity. Regarding etiology, 13 patients (61.9%) had a history of herpes simplex or herpes zoster virus infection, two patients (9.5%) had diabetes mellitus, two patients (9.5%) had a history of trigeminal nerve surgery, three patients (14.3%) had undergone penetrating keratoplasty, and one patient (4.8%) had a history of laser-assisted in situ keratomileusis (LASIK) refractive surgery.
Methods
-
Comprehensive ocular examinations were performed at baseline and follow-up visits as part of routine clinical practice. The treatment consisted of cenegermin (20 μg/mL) administered six times daily for 8 weeks. Thereafter, patients with an Oxford score > 0 continued to receive preservative-free sodium hyaluronate eye drops. Assessments were conducted at baseline, Week 4, Week 8, and Week 56, and data were collected on PED healing (Oxford scale, with clinical healing defined as a maximum diameter ≤ 0.5 mm and a score of 0 indicating complete healing), epithelial defect recurrence, corneal sensitivity (Cochet–Bonnet), BCVA (logarithm of the minimum angle of resolution [LogMAR]), ocular pain (visual analog scale [VAS]), conjunctival hyperemia (Efron scale), and corneal neovascularization. The methods used for these examinations are described below.
Corneal epithelial status was evaluated using corneal fluorescein sodium staining test paper. Corneal epithelial healing was assessed under cobalt blue light with a slit lamp. According to the Oxford ocular surface staining score, the cornea was divided into five quadrants and graded as 0 (≤ 1 spot), 1 (2–10 spots), 2 (> 10 spots without obvious fusion), or 3 (diffuse staining with significant fusion)[10]. The diameter of the corneal epithelial defect was measured from external digital photographs of the eye using ImageJ, with a maximum diameter ≤ 0.5 mm defined as clinical healing and a score of 0 indicating complete healing.
Corneal nerve architecture was assessed using in vivo confocal microscopy (IVCM) with the Heidelberg Retina Tomograph II and Rostock Cornea Module (HRT II RCM; Heidelberg Engineering, Heidelberg, Germany). The system scanned the central, superior, inferior, nasal, and temporal corneal quadrants to evaluate the density and morphology of the subepithelial nerve plexus and intraepithelial nerve endings, as well as their spatial variations from the peripheral to central cornea. Stromal nerve regeneration was assessed by systematically scanning multiple locations within each quadrant across different depth layers. IVCM images were retrieved at baseline, 8 weeks, and 56 weeks, with five images obtained at the level of the epithelium and basal lamina at each time point. Only well-focused frames with good contrast and containing the entire image within a single layer were included; oblique sections were excluded. All images were anonymized before analysis. Subbasal corneal nerve fibers were traced and quantified using ImageJ software. Nerve density was expressed in millimeters per square millimeter (mm/mm2), and the number of nerve branches was manually counted per image. For each patient at each time point, nerve density and branch number are reported as the median and interquartile range (IQR). The nerve regeneration rate (NRR) was calculated as (follow-up nerve density – baseline nerve density) / follow-up months.
Corneal sensitivity was measured with a Cochet–Bonnet esthesiometer (Luneau Ophthalmologie, Chartres, France). Measurements were taken at the central cornea (within an area 4.0 mm in diameter over the pupil) and at four peripheral points (superior, inferior, nasal, and temporal), each located 1–2 mm inside the corneal limbus[11]. The filament was applied vertically to the cornea, starting at a length of 60 mm and reducing in 5-mm decrements until the patient perceived contact. Each length was tested three times, and a positive response was recorded if detected in at least two trials. The final threshold length was recorded in millimeters.
BCVA measurements recorded before and after treatment were collected from medical records and converted to LogMAR visual acuity for statistical analysis. At each follow-up visit, patients were asked whether they had eye pain; if present, pain was assessed using the VAS, and the scores were recorded. The Efron ocular hyperemia grading scale was applied to external eye photographs captured at each visit. Conjunctival areas in four locations (superior, nasal, inferior, and temporal) were graded from 0 to 4, and the average of the four scores was used as the patient's Efron grading score for that visit.
Image analysis and blinding procedure
-
A masked method was used for data assessment to minimize observer bias during image analysis. All images were anonymized and recoded by an independent researcher who was not involved in clinical care. The code key was sealed until all measurements were completed. The evaluator responsible for quantitative analysis remained blinded to the patients' identity and the time point of image acquisition.
Statistical methods
-
All statistical analyses were performed using IBM SPSS Statistics (Version 27). The normality of continuous variables was assessed using the Shapiro–Wilk test. Data found to be normally distributed (corneal sensitivity, Efron hyperemia grading) were analyzed using repeated-measures analysis of variance (ANOVA) with Bonferroni's post hoc correction for multiple comparisons, with the adjusted significance level set at α = 0.05/4 = 0.0125 for corneal sensitivity (pairwise comparisons among four time points) and α = 0.05/3 = 0.017 for Efron hyperemia grading (pairwise comparisons among three time points). Data not conforming to a normal distribution (relative area of corneal epithelial defects, corneal epithelium healing time, BCVA-LogMAR, relative area of corneal neovascularization, corneal subbasal nerve density and branches) were analyzed using the Friedman test. Within-group pairwise comparisons were then performed using the Wilcoxon signed-rank test, with multiplicity adjustment via Bonferroni's method (adjusted α = 0.05/3 = 0.017). In all reports, 'p' denotes the adjusted p-value after Bonferroni correction.
The sample size was based on the 8-week clinical healing rate of corneal epithelial defects, using the formula for a single proportion (normal approximation) with a two-sided α of 0.05 and a power of 0.80.
-
Twenty-one patients (21 eyes) were included in the final analysis. At baseline, the median for the relative area of the corneal epithelial defect was 6.90% (IQR: 19.75%). At Week 4, the relative area decreased to 2.60% (5.50%), which was significantly lower than at baseline (Z = –4.016, p < 0.001, r = 0.88). At this time point, eight patients (38.1%) achieved clinical healing, defined as a maximum defect diameter ≤ 0.5 mm. By Week 8, the relative area further decreased to 0.00% (0.65%), remaining significantly lower than at baseline (Z = –4.015, p < 0.001, r = 0.88); all patients showed a reduction in defect area compared with the baseline, and 16 patients (76.2%) met the criteria for clinical healing. By Week 56, the relative area decreased to 0.00% (0.00%), remaining significantly lower than at baseline (Z = −4.015, p < 0.001, r = 0.88) (Fig. 1a), and 20 patients (95.2%) had an Oxford score of 0, indicating no epithelial defect. To further quantify the healing process, we analyzed the time required for patients to achieve clinical healing and Oxford score = 0. Consistent with the progressive reduction in the area of corneal epithelial defects observed at each follow-up time point, the median time to clinical healing of the corneal epithelial defect was 6.00 (IQR: 4.50) weeks, whereas the median time to achieve an Oxford score of 0 was 12.00 (IQR: 13.00) weeks. The time to Oxford score normalization was significantly longer than the time to epithelial defect closure (Z = –3.923, p < 0.001, r = 0.86) (Fig. 1b). However, one patient experienced recurrence of the epithelial defect. The patient’s epithelial defect initially healed at Week 21, although corneal sodium fluorescein staining revealed minimal punctate staining at that time. Recurrence occurred at Week 39, resulting in a new epithelial defect. A representative image of corneal epithelial defect recovery is shown in Fig. 2a.
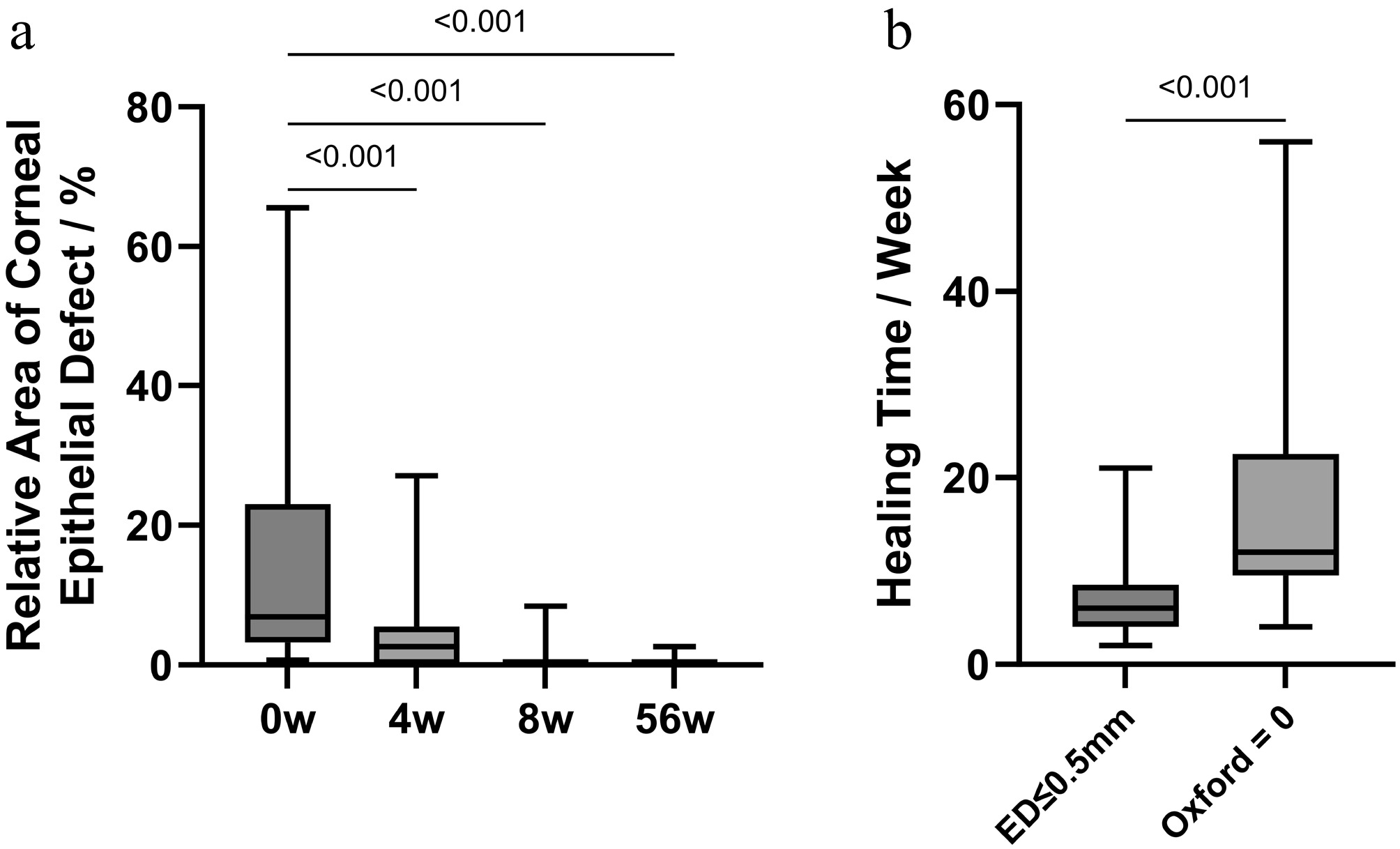
Figure 1.
(a) Changes in the relative area of corneal epithelial defects (epithelial defect area/corneal area) at different follow-up time points. (b) Time to achieve clinical healing (epithelial defect diameter ≤ 0.5 mm) and Oxford score = 0 (complete healing). Data are presented as the median and IQR. Statistical analysis was performed using the Wilcoxon signed-rank test; n = 21.
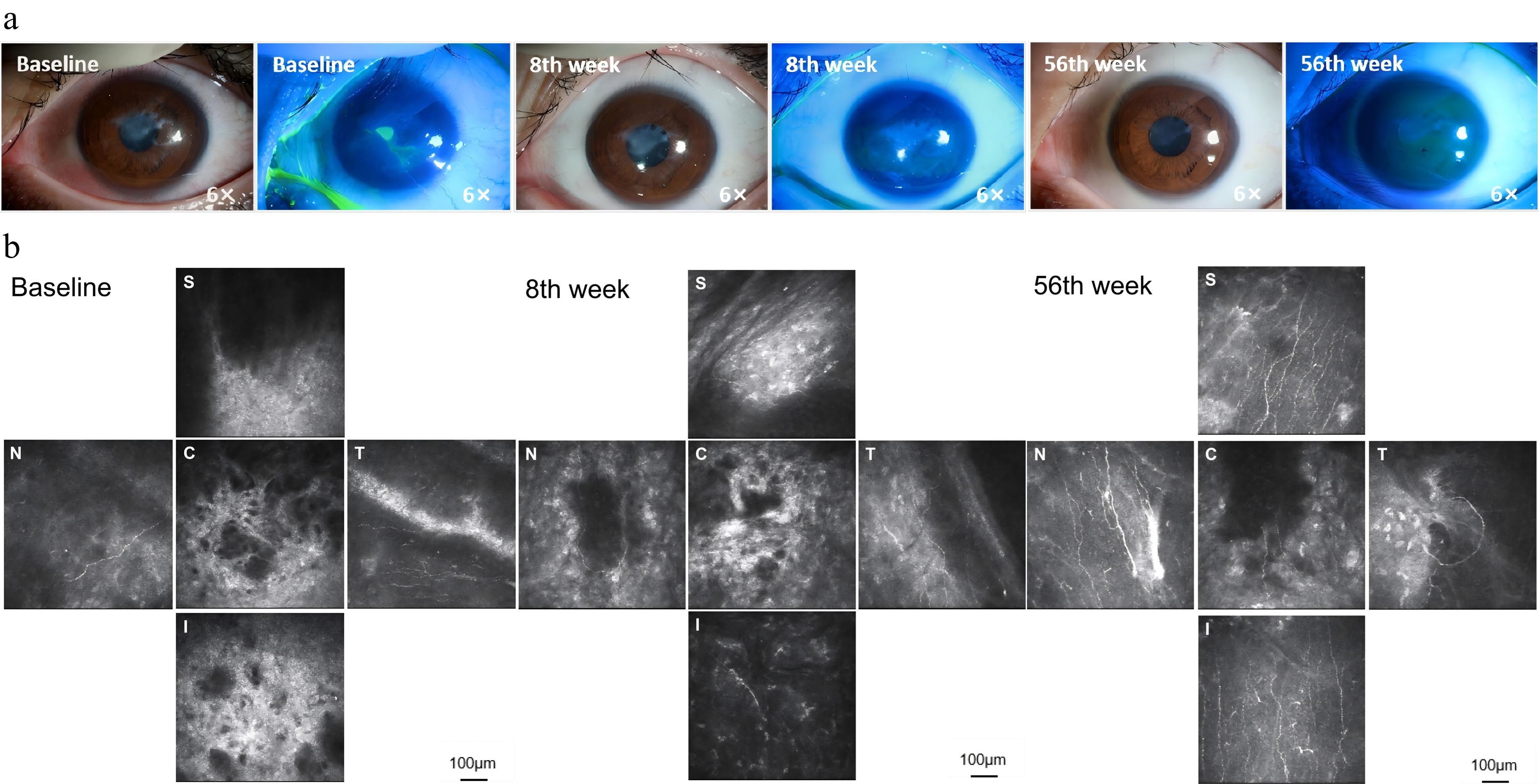
Figure 2.
Representative images of corneal epithelial healing and nerve regeneration in a patient with a history of LASIK refractive surgery. (a) External eye photographs at baseline, Week 8, and Week 56 (magnification: 6×). (b) In vivo confocal microscopy (IVCM) images at baseline, Week 8, and Week 56, showing corneal nerves' distribution in different regions. C: central cornea; S: superior cornea; I: inferior cornea; N: nasal cornea; T: temporal cornea. Scale bar: 100 μm.
Corneal nerve fiber growth
-
At baseline, IVCM revealed no detectable nerve fibers in 19 of 21 patients (90.5%). At Week 8, 14 of 21 patients (66.7%) showed sparse, low-density subepithelial corneal nerve fibers and sparse stromal nerve fibers. By Week 56, 20 of 21 patients (95.2%) had sparse, scattered nerve fibers in the affected area, although nerve fibers remained undetectable in 1 patient (4.8%).
Nonparametric analysis revealed significant changes in corneal nerve parameters over time. For corneal nerve fiber density, Friedman's test showed a significant overall difference across time points (χ2 = 33.342, degrees of freedom [df] = 2, p < 0.001, Kendall's W = 0.794). The median nerve density increased from 0.00 (IQR: 0.00) mm/mm2 at baseline to 2.44 (IQR: 8.39) mm/mm2 at Week 8 (Z = −3.296, p = 0.001, r = 0.72), and further increased to 14.60 (IQR: 11.10) mm/mm2 at Week 56 (Z = −3.920, p < 0.001, r = 0.86). A significant difference was also observed between Week 8 and Week 56 (Z = −3.250, p = 0.001, r = 0.71) (Fig. 3a).
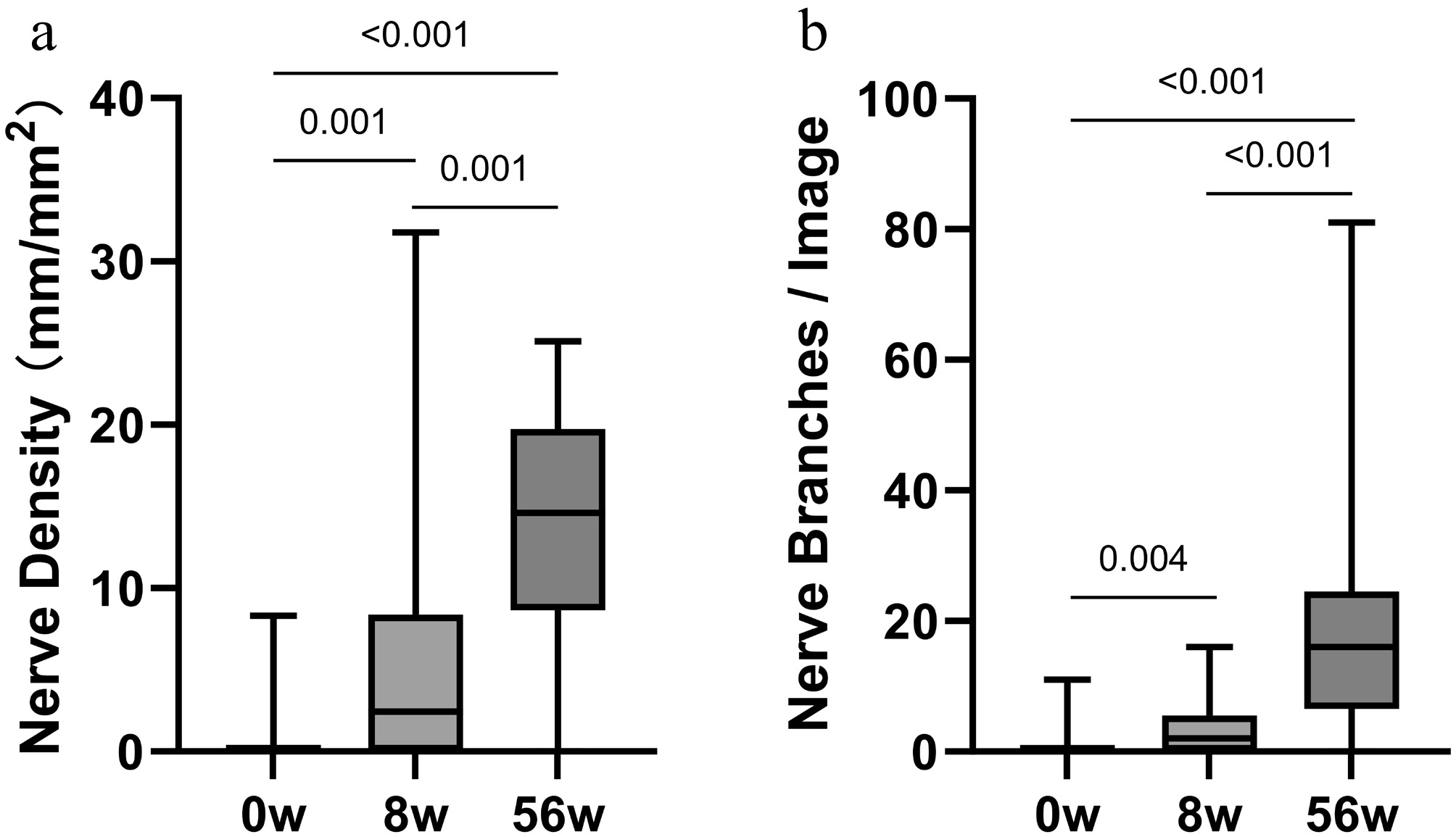
Figure 3.
Changes in corneal subbasal nerve parameters during follow-up. (a) Corneal nerve fiber density (mm/mm2) at baseline, Week 8, and Week 56. (b) Corneal nerve branch count per image at baseline, Week 8, and Week 56. Data are presented as the median and IQR. Friedman's test was used for overall comparison, followed by Wilcoxon's signed-rank test for pairwise comparisons; n = 21.
For corneal nerve branch count, Friedman's test also demonstrated a significant overall difference (χ2 = 32.350, df = 2, p < 0.001, Kendall’s W = 0.770). The median branch count increased from 0.00 (IQR: 0.00) per image at baseline to 2.00 (IQR: 6.00) per image at Week 8 (Z = −2.913, p = 0.004, r = 0.64), and further increased to 16.00 (IQR: 18.00) per image at Week 56 (Z = −3.921, p < 0.001, r = 0.86). A significant difference was also observed between Week 8 and Week 56 (Z = −3.547, p < 0.001, r = 0.77) (Fig. 3b).
According to the median values, the average growth rate of nerve fiber density was 1.22 mm/(mm2·month) during the first 8 weeks (0–8 weeks) and 1.01 mm/(mm2·month) from Week 8 to Week 56.
At baseline, the IVCM of one patient revealed central corneal scarring with no detectable nerve fibers within the lesion area. However, sparse subepithelial nerve fibers were observed in the nasal and temporal quadrants, peripheral to the lesion. Slender nerve fibers were observed in the superior and inferior cornea at Week 8. By Week 56, IVCM imaging showed the nerve fibers' distribution across the cornea (Fig. 2b). The central scar remained persistent. In the central, superior, and nasal regions, the nerve fibers appeared slender and exhibited low density. In contrast, regeneration from the temporal quadrant seemed to be impeded. The fibers failed to penetrate the central scar and instead formed meandering, loop-like structures at the periphery.
Corneal sensitivity
-
Figure 4a presents the results of corneal sensitivity measurements in the central, inferior, nasal, superior, and temporal regions of cornea. At baseline, the mean (± standard deviation [SD]) corneal sensitivity across all regions was 0.52 ± 1.12 cm.
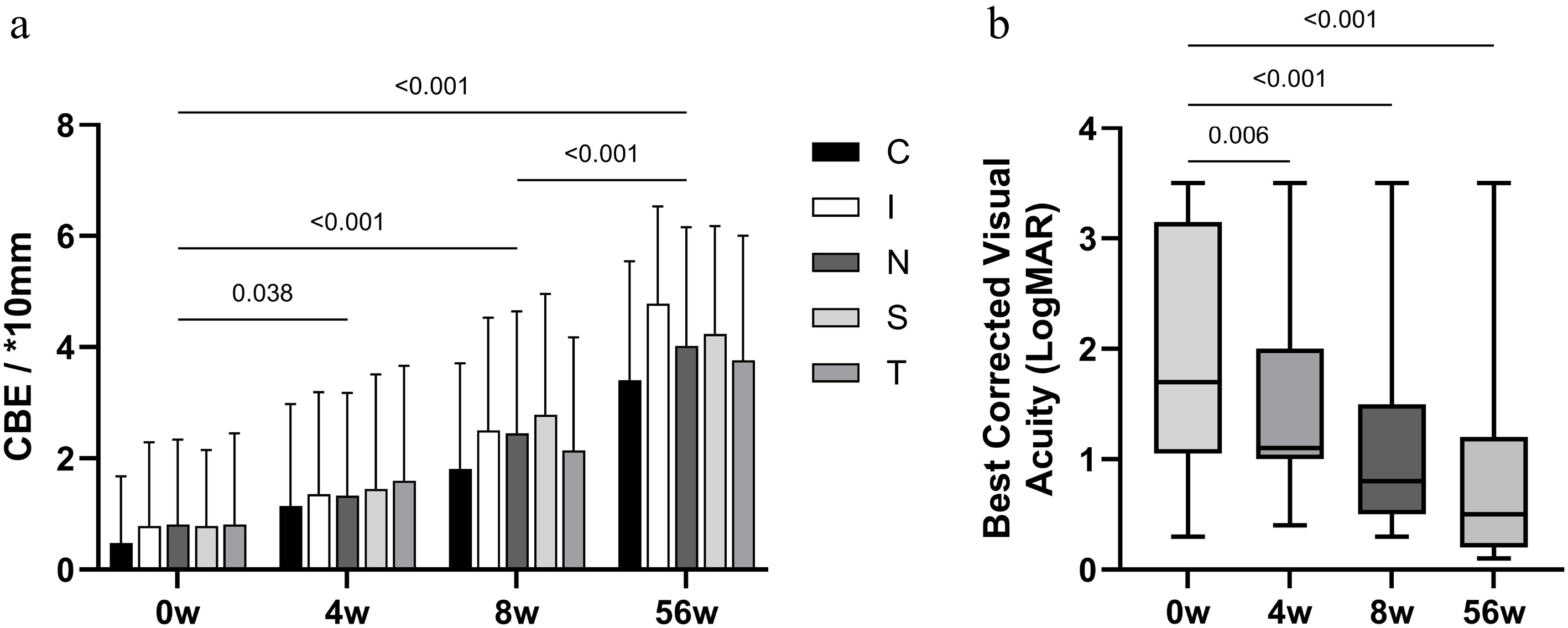
Figure 4.
Changes in corneal sensory and visual function during follow-up. (a) Corneal sensitivity (measured by Cochet–Bonnet esthesiometry, CBE) in the central, superior, inferior, nasal, and temporal cornea at baseline, Week 4, Week 8, and Week 56. C: central; S: superior; I: inferior; N: nasal; T: temporal. (b) Best corrected visual acuity (BCVA, LogMAR) at baseline, Week 4, Week 8, and Week 56. Data are presented as the mean ± SD or median and IQR. Statistical analysis was performed using repeated-measures ANOVA or Friedman's test with post hoc correction; n = 21.
By Week 8, corneal sensitivity increased to a mean of 2.03 ± 1.98 cm, which was significantly higher than baseline (Z = −3.296, p < 0.001, r = 0.72); at this time point, 16 of 21 patients (76.2%) showed an improvement in sensitivity in at least one region.
By Week 56, corneal sensitivity further increased to a mean of 3.33 ± 1.86 cm, remaining significantly elevated compared with the baseline (Z = −3.920, p < 0.001, r = 0.86). Twenty patients (95.2%) demonstrated an improvement in corneal sensitivity across one or more regions. Moreover, at Week 56, corneal sensitivity showed a further significant improvement compared with Week 8 (Z = −3.250, p = 0.001, r = 0.71), with 19 of 21 patients (90.5%) demonstrating higher sensitivity than at Week 8.
Best corrected visual acuity
-
At baseline, the median BCVA (LogMAR) was 1.70 (IQR: 2.10). By Week 4, it improved to 1.10 (1.00) (Z = −2.737, p = 0.006, r = 0.60) (Fig. 4b). At Week 8, the BCVA further improved to 0.80 (1.00) (Z = −3.442, p < 0.001, r = 0.75); at this time point, 18 of 21 patients (85.7%) showed improved visual acuity compared with the baseline. By Week 56, the BCVA improved to 0.50 (1.00) (Z = −3.928, p < 0.001, r = 0.86), with 20 of 21 patients (95.2%) demonstrating improved visual acuity compared with the baseline.
Eye pain and ocular hyperemia
-
During the treatment period (0−8 weeks), eight patients (38.1%) experienced mild to moderate eye pain or itching. The symptoms were tolerable and did not interfere with daily activities (VAS score: 1−4). During Weeks 8−56, all of the symptoms resolved or subsided after treatment discontinuation.
Conjunctival hyperemia was graded using the Efron grading scale on external eye photographs captured at each visit, and the changes over time are illustrated in Fig. 5a. The mean (± SD) Efron grade was 2.32 ± 0.96 at baseline. One-way ANOVA revealed a significant difference among the four time points (F = 6.422, p = 0.0006, η2 = 0.194). Dunnett's multiple comparisons test showed that the grade at Week 56 (1.10 ± 0.71) was significantly lower than at the baseline (mean difference = 1.226, 95% confidence interval [CI] = 0.4735–1.979, p = 0.0006), whereas the differences at Week 4 (2.25 ± 1.14) and Week 8 (1.96 ± 1.07) were not statistically significant compared with the baseline (both p > 0.05). In terms of individual changes, conjunctival hyperemia was transiently increased in nine patients (42.9%) at Week 4 and seven patients (33.3%) at Week 8 relative to the baseline. By Week 56, 17 patients (81.0%) showed a lower Efron grade than at the baseline, indicating the resolution of hyperemia after treatment completion.
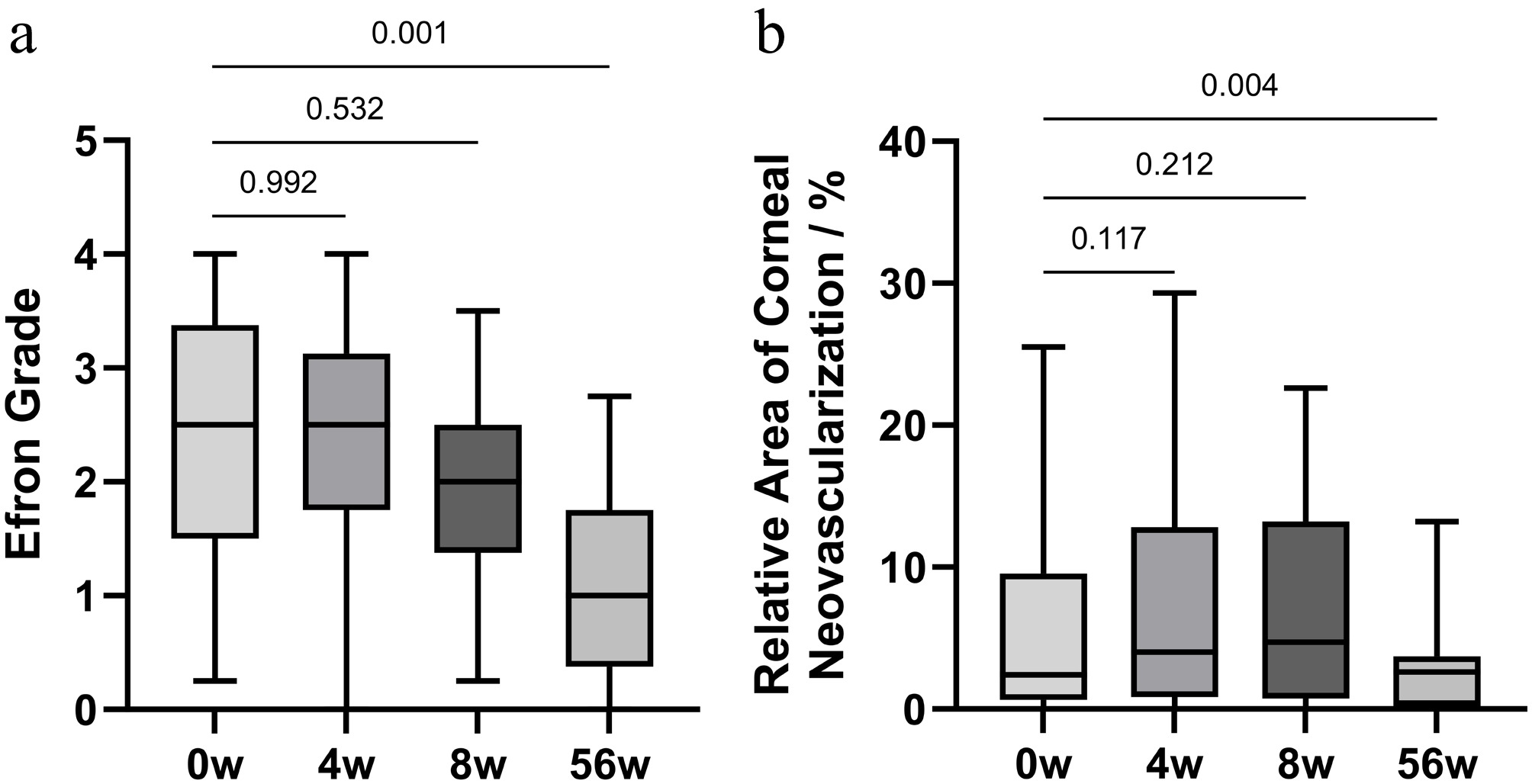
Figure 5.
Changes in ocular safety indicators during follow-up. (a) Efron ocular hyperemia grade at baseline, Week 4, Week 8, and Week 56. (b) Relative area of corneal neovascularization at baseline, Week 4, Week 8, and Week 56. Data are presented as the mean ± SD or median and IQR. Statistical analysis was performed using one-way ANOVA or Wilcoxon's signed-rank test; n = 21.
Corneal neovascularization
-
The median relative area of corneal neovascularization was 2.40% (IQR: 8.90%) at baseline, 4.00% (IQR: 11.95%) at Week 4, 4.70% (IQR: 12.45%) at Week 8, and 2.60% (IQR: 3.50%) at Week 56. Wilcoxon's signed-rank tests revealed a significant difference between Week 56 and the baseline (Z = −2.913, p = 0.004), though no significant differences were observed between Week 4 and the baseline (Z = −1.569, p = 0.117) or between Week 8 and the baseline (Z = −1.248, p = 0.212). In terms of individual changes, compared with the baseline, 14 patients (66.7%) showed increased neovascularization at Week 4, 12 patients (57.1%) at Week 8, and two patients (9.5%) at Week 56. By Week 56, 15 patients (71.4%) had a smaller neovascular area than at baseline, indicating regression after treatment completion (Fig. 5b).
-
In this retrospective analysis, the observed long-term corneal structural and functional recovery aligns with the known mechanisms of rh-NGF. It promotes the growth of corneal nerves and supports the differentiation, proliferation, and migration of corneal epithelial cells. It also enhances communication between corneal nerves and epithelial cells. In addition, it aids in regenerating the damaged extracellular matrix and facilitates cell migration. Together, these actions promote the structural repair of the cornea. By improving the corneal microenvironment, it creates favorable conditions for nerve regeneration. These benefits are achieved through increased nutrient supply, reduced inflammation and edema, and protection of corneal limbus stem cells[12].
The overall improvement in corneal sensitivity paralleled the observed increases in nerve density and branch number in this cohort, which aligns with the positive correlation between corneal sensation and subbasal nerve morphology reported in the literature[13,14]. Although there is currently no clearly defined threshold for corneal sensitivity that definitively represents successful healing or neural rehabilitation, the observations in this study offer preliminary insights. After 8 weeks of rh-NGF treatment, corneal sensation had recovered to approximately 2.44 mm/mm2, and 76.2% of patients achieved clinical healing of their corneal epithelial defects. In previous studies, the 8-week healing rate of corneal epithelial defects ranged from approximately 69.6% to 84.8%, with some studies combining rh-NGF with other medications. These healing rates are generally consistent with the findings of our study[5,7,15]. Concurrently, corneal nerve density and branch number also showed significant improvement compared with the baseline. However, as revealed by IVCM, subbasal nerve fibers were not initially evident in some patients, suggesting that nerve growth may have lagged behind, indicating that the recovery of sensation and nerve regeneration were not entirely synchronous. This finding is consistent with Pedrotti et al.[16]. The nerve regeneration rate at 8 and 56 weeks is consistent with this observation. Following drug cessation, nerve density was maintained, but the regeneration rate slowed. This may indicate that the healing of the corneal epithelium serves as the foundation for improving corneal sensation, but the growth of nerve fibers may proceed more slowly than the recovery of corneal sensation. It is important to note that this interpretation requires further validation, as early sensory improvement could involve mechanisms beyond the regrowth of nerves visible by IVCM[16].
During the 8- to 56-week follow-up period, although the corneal epithelial defects had clinically healed in most patients, corneal fluorescein punctate staining (Oxford score > 0) persisted. This may reflect an unstable ocular surface microenvironment. Therefore, the continued use of preservative-free artificial tears, such as sodium hyaluronate eye drops, may be beneficial. Consistent with previous studies, at Week 8, IVCM revealed corneal nerve regeneration. In our study, nerve fibers had regenerated in 66.7% of patients, appearing sparse and thin, but not yet reaching a density comparable with that of healthy eyes[7,14,16]. The study by Saricay et al. further provided key dynamic evidence, reporting a nerve regeneration rate of 1.87 mm/mm2 per month in patients with Stage 1 NK. In our study, the nerve regeneration rate was 1.22 mm/mm2 per month during the first 8 weeks and 1.01 mm/mm2 per month from Week 8 to Week 56, suggesting that nerve regeneration was more rapid in the early phase of treatment[17]. Moreover, scar formation after lesion healing may impede nerve growth, preventing regeneration into the center of the original defect. In one patient, no subepithelial nerve fibers were detected in the lesion area at baseline. By Week 8, a small number of subepithelial nerve fibers were observed, though no stromal nerves were visible. However, by Week 56, the IVCM examination showed that the previously regenerated subepithelial nerve fibers were no longer detectable, suggesting the regression of nerve regeneration. Previous studies have indicated that following penetrating keratoplasty, the regeneration of corneal subepithelial nerve fibers can lead to complications such as graft rejection, secondary glaucoma, wound leakage, suture loosening, and recurrence of the original disease. The regenerated subepithelial nerve fibers often exhibit regression, characterized by shortened length, reduced density, and altered morphology, including increased tortuosity and fragmentation. Notably, these changes have not been observed in corneal stromal nerve fibers. Throughout the observation period, the regeneration of subepithelial nerve fibers occurred earlier than that of stromal nerves. Stromal nerve regeneration appeared to be hindered by scar tissue within the lesion. Tervo et al.[18] reported that even three years after penetrating keratoplasty, corneal nerve density and architecture did not fully recover. Although subepithelial nerves demonstrated regenerative capacity, stromal nerves remained deficient. This lack of stromal regeneration may be attributed to the discontinuity of Schwann cells at the graft–host interface. In the NK cornea, this phenomenon requires further investigation.
One patient experienced a recurrence of an epithelial defect that persisted until the end of the 56-week follow-up. This patient had Type I diabetes as the underlying etiology. The association between diabetes and NK was first identified as early as 1977 and is attributed to trigeminal neuropathy resulting from microvascular damage to myelinated nerve fibers[19]. In diabetic patients, the severity and progression of NK are closely linked to peripheral neuropathy. Therefore, the corneal nerve plexus is considered to be a significant indicator of the progression and treatment response of peripheral neuropathy[20]. In particular, the corneal nerve plexus is considered to be a useful parameter for evaluating diabetic sensorimotor polyneuropathy[21]. Additionally, diabetes adversely affects the ocular surface by causing tear film instability and altering the ocular surface's microbiome, thereby increasing the risk of corneal erosion and infection. For patients with NK associated with Type I diabetes, strict glycemic control is especially critical.
The observed side effects, namely hyperemia, pain, and neovascularization, are consistent with previous reports[7,22]. These reactions may be related to the pharmacological activity of the drug as well as the inflammatory processes accompanying nerve regeneration and epithelial repair. Of note, eye pain tended to occur first during treatment. Studies have suggested that nerve growth factor may act through multiple pain-related pathways or be associated with increased sensitivity of the regenerating nerves[23], which may indicate the initiation of nerve repair.
This study has several limitations. Given that NK is a rare disease, the sample size was small and there was no control group, with patients serving as their own controls. The limited sample size may lead to an overestimation of the treatment effect in broader populations. Furthermore, the study was not powered to adequately assess the incidence of adverse events (such as hyperemia, eye pain, and corneal neovascularization) as well as the recurrence rate of epithelial defects. This is consistent with the common challenge faced by many investigative groups studying rare diseases, where achieving large cohorts is difficult[3]. The conclusions derived from this study should be considered to be preliminary and interpreted within the context of its methodological constraints. Generalization of the findings to broader NK populations requires caution and awaits validation from larger controlled studies, which are currently underway. Additionally, bilateral IVCM examinations were not performed at each follow-up visit, which limited detailed observations of the process of rh-NGF eye drops promoting corneal subepithelial nerve regeneration. For patients who showed suboptimal corneal nerve regeneration or incomplete sensory recovery, extended treatment duration or combined therapeutic strategies, such as adjunctive neurotrophic factors or surgical procedures, warrant further investigation. Future studies should also explore differences in neural recovery based on etiology and baseline disease severity, and investigate how treatment protocols can be optimized to enhance both corneal nerve regeneration and sensory restoration, ultimately improving clinical outcomes and quality of life for patients.
-
The findings indicate that rh-NGF treatment promotes the rapid healing of corneal epithelial defects and the recovery of corneal sensitivity. In contrast, corneal nerve regeneration follows a longer-term course. Some of these therapeutic effects were sustained for an extended period after treatment cessation. However, given the limited sample size and the absence of a control group in this study, these findings require further validation in larger-scale controlled trials to confirm the treatment's efficacy and long-term benefits.
-
Approved by the Beijing Tongren Hospital Ethics Committee (TREC2026-KY115, March 15, 2026), this study followed the Declaration of Helsinki, and all participants provided written informed consent. DeepSeek (2026) was used for language refinement in this manuscript. The authors reviewed and edited all content produced with the assistance of this tool, verified its accuracy, and take full responsibility for the integrity and originality of the final manuscript. This work represents the authors' own intellectual contribution, and no artificial intelligence tool is credited as an author.
-
The authors confirm contribution to the paper as follows: study conception and design: Li S, Jie Y; data collection: Sun X, Li S; analysis and interpretation of results: Sun X, Wei Y, Gu Y; draft manuscript preparation: Sun X, Li S, Li A. All authors reviewed the results and approved the final version of the manuscript.
-
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
-
This work is supported by the following fund projects: National Key R&D Program of China (2023YFC2410401); Yicheng Outstanding Talents in Beijing Economic–Technological Development Area; Beijing Nova Program (20240484600); Beijing Hospitals Authority's Ascent Plan (DFL20240202); Capital Health Research and Development of Special (Grant No. 2022-1-1081 to Dr Jie); the Youth Beijing Scholars' program (No. 022); High-Level Public Health Technical Talents Construction Project from Beijing (Ying Jie); and Beijing Municipal Public Welfare Development and Reform Pilot Project for Medical Research Institutes (PWD&RPP-MRI, JYY2023-6).
-
The authors declare that they have no conflict of interest.
-
Authors contributed equally: Shang Li, Xiuli Sun
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Li S, Sun X, Wei Y, Gu Y, Li A, et al. 2026. Recombinant human nerve growth factor eye drops for corneal sensation and nerve regeneration in neurotrophic keratitis. Visual Neuroscience 43: e025 doi: 10.48130/vns-0026-0024 

Recombinant human nerve growth factor eye drops for corneal sensation and nerve regeneration in neurotrophic keratitis
- Received: 25 March 2026
- Revised: 29 April 2026
- Accepted: 19 May 2026
- Published online: 23 June 2026
Abstract: This study retrospectively evaluated long-term nerve regeneration and corneal sensation in patients with neurotrophic keratitis following treatment with recombinant human nerve growth factor. This study analyzed 21 patients with neurotrophic keratitis who received recombinant human nerve growth factor eyedrops (20 μg/mL) six times daily for 8 weeks. Clinical data at baseline, Week 4, Week 8, and Week 56 included the relative area of corneal epithelial defects, Oxford score, corneal nerve fiber growth, corneal sensitivity, best corrected visual acuity, Efron ocular hyperemia grade, visual analog scale pain score, and the relative area of corneal neovascularization. Corneal epithelial defect area decreased progressively, with complete healing in 16/21 patients (76.2%) at Week 8 and 20/21 patients (95.2%) at Week 56. Corneal sensitivity recovered gradually, with 16/21 patients (76.2%) showing improvement at Week 8 and 20/21 patients (95.2%) at Week 56. During treatment, eight patients (38.1%) had mild to moderate ocular pain or itching, all resolving after treatment discontinuation. Quantitative in vivo confocal microscopy demonstrated significant corneal nerve regeneration, with marked increases in nerve fiber density and branch count over the study period. Corneal epithelial recovery precedes nerve regeneration, and regenerated nerves remain slender and structurally abnormal, indicating that corneal nerve repair is a prolonged process.
-
Key words:
- Neurotrophic keratitis /
- rh-NGF /
- Nerve regeneration /
- Corneal sensation