









-
Implantable collamer lens (ICL) implantation has become one of the most effective refractive surgery for high myopia[1−3]. Most of the high myopic patients who undergo refractive surgery have high satisfaction and improved quality of life after the operation. However, some visual complaints, such as visual fatigue, blurred vision, or diplopia at near range, might reduce satisfaction after refractive surgery, especially in the early stage[4].
An ideal refractive surgery should be not only safe, with good visual acuity and visual quality, but also coordinative binocular visual functions and comfortable vision. The accommodative and vergence functions, which control the ocular focus, alignment, and fixation, may be affected by refractive surgery. Alterations in accommodative and vergence functions are one of the most common causes of visual fatigue. Moreover, accommodation and vergence are correlated with wide regions of the brain[5]. Accommodative and vergence anomalies, such as convergence insufficiency, are commonly observed following cerebral injury[6]. Previous studies have demonstrated that laser refractive surgery can lead to decreased amplitude of accommodation (AMP), reduced accommodative facility (AF), receded near point of convergence (NPC), decreased accommodative convergence/accommodation (AC/A) ratio, and diminished fusional vergence amplitudes[7−11]. In contrast, Chen[12] found that accommodative function improved after ICL implantation and stabilized within 1 month. Li[13] reported no significant differences in either AMP or accommodative lag. Kamiya[14] and Wan[15] observed that AMP was temporarily impaired in the early postoperative periods but recovered gradually. Most previous research measured some of the parameters of accommodation or vergence, and there were inconsistencies in various outcomes from different studies. Howevver, previous studies about ICL implantation have rarely focused on phoria or vergence function.
The purpose of this study was to comprehensively evaluate the time course of accommodative and vergence functions in high myopic patients following ICL implantation. A broad spectrum of parameters was assessed, including AMP, negative and positive relative accommodation (NRA/PRA), AF, distance and near lateral phoria (DLP/NLP), negative and positive fusional vergence (NFV/PFV), NPC, and vergence facility (VF). This investigation holds significant implications for optimizing patient selection criteria and refining postoperative management strategies in ICL surgery.
-
This was a prospective observational study. Thirty-five patients were enrolled at Zhongshan Ophthalmic Center between October 2022 and October 2024. This study followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, China (No. 2022KYPJ198). Written informed consent was obtained from all participants.
The inclusion criteria were as follows: (1) age 18–35 years old; (2) high myopia with –15.00 D < spherical equivalent ≤ –6.00 D, astigmatism ≥ –2.00 D, anisometropia ≥ –2.00 D, and refraction that had remained stable for 2 years at least; and (3) best corrected visual acuity (BCVA) was better than 20/25 in both eyes.
The exclusion criteria were as follows: (1) a history of strabismus, amblyopia, nystagmus, glaucoma, or retina or optic nerve disease; (2) previous ocular or brain trauma or surgery; (3) absence of binocular visual functions; (4) any systemic pathology or pharmacological side effects that could affect binocular visual functions; and (5) severe ocular surface disease which was inoperable.
Preoperative ocular assessment
-
All patients underwent routine preoperative examination, including uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA), manifest and cycloplegic refraction, slit-lamp and funduscopic examination, noncontact tonometry, axial length measurement (IOLMaster 700, Carl Zeiss Meditec AG), corneal endothelial cell density measurement (CEM-530, Nidek Co., Ltd.), Scheimpflug tomography with a Pentacam HR (Oculus Optikgeräte GmbH) for white-to-white (WTW), anterior chamber depth (ACD), and central corneal thickness (CCT).
Assessment of binocular visual functions
-
All examinations were conducted under standard indoor lighting by the same experienced examiner. Patients underwent manifest refraction to achieve maximum plus to maximum visual acuity (MPMVA). DLP and distance NFV were measured at 3 m, but the other parameters were assessed at 40 cm.
(1) DLP and NLP: These were measured using the von Graefe technique. For DLP, a single 20/30 letter on the distance chart (3 m) was used as the target. Risley prisms were placed before both eyes: 6∆ base-down (BD) before the right eye to induce vertical dissociation, and 12∆ base-in (BI) before the left eye. Patients were instructed to fixate on the upper target. The horizontal prism before the left eye was reduced at a rate of 2∆ per second until the patient reported that the two targets were vertically aligned. For NLP, the same procedure was repeated using an isolated 20/30 letter on the near chart at 40 cm.
(2) NFV and PFV: A vertical line of 20/30 letters was used as the fixation target. Risley prisms were set at zero before both eyes. Patients were instructed to keep the target "single and clear." To measure NFV, BI prisms were introduced at a rate of 2∆/s until the patient reported diplopia (the break point). For PFV, BO prisms were introduced in the same manner. This procedure was performed at both 3 m (distance) and 40 cm (near).
(3) NRA/PRA: Using a line of 20/30 letters on the near chart, patients were instructed to maintain a single and clear image. Plus lenses (for NRA) were added in +0.25 D increments until the patient reported the first sustained blur. After removing the plus lenses and allowing for recovery, minus lenses (for PRA) were added in –0.25 D increments until the first sustained blur was reported. The total added power for each was recorded.
(4) AMP: This was measured monocularly (right eye) using the push-up method. Patients fixated on a 20/30 letter on a fixation stick held at 40 cm. The target was slowly moved toward the patient until the first sustained blur was reported. The distance from the target to the spectacle plane was measured. The reciprocal of this distance (in meters) was defined as the AMP.
(5) NPC: This was measured binocularly using the push-up method. Patients were instructed to fixate on an isolated 20/30 letter and keep it single for as long as possible. The target was moved toward the patient's midline until they reported diplopia or the examiner observed an objective break characterized by one eye drifting outward. The distance from the target to the lateral canthus plane was then recorded.
(6) VF: Measured at 40 cm using a 3∆ BI/12∆ BO flipper. Patients fixated on a 20/30 letter and were instructed to make the target clear and single as quickly as possible. Once clarity was achieved, the flipper was immediately flipped. The number of completed cycles per minute (cpm) was recorded.
(7) AF: This was measured at 40 cm using a ±2.00 D flipper. Using a line of 20/30 letters, patients were instructed to get the target clear as rapidly as possible. The flipper was flipped immediately upon the patient's report of clarity. The total number of cycles completed in one minute (cpm) was recorded[16].
Surgical procedure and postoperative follow-up
-
The parameters of the V4c ICLs were determined according to the STAAR Online Calculation and Ordering System (STAAR OCOS) website (
https://evo-ocos.staarag.ch ). All ICL implantations were performed by the same experienced surgeon under topical anesthesia after pupil dilation. The V4c ICL was inserted through a 3.0-mm temporal clear corneal incision using an injector cartridge (STAAR Surgical Co.). After filling of the anterior chamber with ophthalmic viscosurgical device material, the ICL was implanted into the posterior chamber and adjusted to the desired cylinder axis. Any remaining ophthalmic viscosurgical device material was washed and replaced with a balanced salt solution.Postoperative follow-up was conducted at 1 day, 1 week, 1 month, 3 months and 6 months. UDVA, noncontact tonometry, slit-lamp examination, manifest refraction, and binocular visual functions assessment were performed at each follow-up visit.
Statistical analysis
-
A priori sample size calculation was performed using G*Power software (version 3.1.9.7). According to a pilot study, to detect a significant difference in the primary outcome (AMP) with an effect size (dz) of 0.60, a minimum sample size of 32 patients was required to achieve a statistical power of 90% (1 – β = 0.90) at a significance level of 5% (α = 0.05), assuming a nonparametric Wilcoxon matched-pairs signed-rank test. Finally, 35 patients were enrolled to account for a potential 10% dropout rate.
Statistical analysis was performed using SPSS Statistics software (version 27.0, IBM Corp.). For the monocular variables (spherical equivalent and AMP), only the data of the right eyes were included in the analysis[17]. Data were presented as the median and interquartile range (IQR). Normality was tested using Shapiro–Wilk tests. A generalized estimating equation (GEE) was used to analyze repeated measurements data, with the age and preoperative spherical equivalent as the covariates. The Wilcoxon matched-pairs signed rank test was used to identify differences between preoperative and postoperative follow-up. Bonferroni correction was applied for multiple comparison adjustments. p-values < 0.05 were considered to be statistically significant.
-
Thirty-five patients with high myopia (8 males and 27 females) were enrolled in this study. The mean age of the patients was 26.74 ± 2.09 years (range: 21–31). The median of preoperative spherical equivalent was –8.63 D (IQR, –9.75 to –7.88 D), and the median of postoperative spherical equivalent was 0.25 D (IQR, 0.00 to 0.50 D) at 1 week, 0.38 D (IQR, 0.25 to 0.63 D) at 1 month, 0.38 D (IQR, 0.13 to 0.56 D) at 3 months, and 0.25 D (IQR, 0.00 to 0.38 D) at 6 months postoperatively. No severe complications occurred during the follow-up.
Accommodative outcomes
-
The time course of accommodative function is presented in Table 1 and Fig. 1. The AMP decreased significantly from 13.33 D (IQR, 11.11 to 15.38 D) at baseline to 10.00 D (IQR, 9.09 to 12.50 D) at 1 week (p < 0.001) and remained at this reduced level through to 6 months postoperatively. No statistically significant differences were observed in NRA between preoperative and any of the postoperative visits. The PRA decreased from –2.50 D (IQR, –3.75 to –2.50 D) at baseline to –2.25 D (IQR, –2.75 to –1.75 D) at 1 week (p = 0.003) and recovered to baseline levels by 1 month. The AF decreased significantly from 9 cpm (IQR, 6 to 11 cpm) preoperatively to 7 cpm (IQR, 4 to 9 cpm) at 1 week (p = 0.039) after surgery, recovered to baseline at 1 month, and slightly increased at 3 months (p = 0.006) and 6 months (p = 0.018).
Table 1. Time course of accommodative parameters.
Preoperative Postoperative Wald χ2 pa 1 Week 1 Month 3 Months 6 Months AMP 13.33 (11.11, 15.38) 10.00 (9.09, 12.50) 10.53 (9.09, 11.76) 11.11 (10.00, 12.50) 11.11 (10.00, 12.50) 48.120 < 0.001 pb < 0.001 < 0.001 0.003 0.007 NRA 2.50 (2.25, 2.50) 2.25 (2.25, 2.50) 2.50 (2.25, 2.50) 2.25 (2.25, 2.50) 2.50 (2.25, 2.50) 4.039 0.401 pb 1.000 0.645 1.000 0.615 PRA −2.50 (−3.75, −2.50) −2.25 (−2.75, −1.75) −2.50 (−3.25, −2.00) −3.00 (−3.50, −2.50) −3.00 (−3.50, −2.50) 29.771 < 0.001 pb 0.003 0.163 1.000 1.000 AF 9 (6, 11) 7 (4, 9) 7 (6, 10) 9 (7, 12) 9 (6, 12) 62.624 < 0.001 pb 0.039 1.000 0.006 0.018 Data are expressed as the median (Quantile 1, Quantile 3). AMP, amplitude of accommodation; NRA, negative relative accommodation; PRA, positive relative accommodation; AF, accommodative facility. pa-values represent the overall significance across all time points (GEE). pb-values represent the differences between the baseline and each postoperative follow-up visit, respectively. 
Figure 1.
Time course of accommodative parameters. AMP, amplitude of accommodation; NRA: negative relative accommodation; PRA, positive relative accommodation; AF, accommodative facility; cpm, cycles per minute.
Phoria and vergence outcomes
-
The time course of vergence function is presented in Table 2 and Fig. 2. The NLP was –5∆ (IQR, –8 to 0∆) preoperatively and changed to –1∆ (IQR, –5 to 3∆) at 1 week and –3∆ (IQR, –6 to 3∆) at 1 month postoperatively, these values differed significantly from baseline (p = 0.001 and p = 0.008, respectively). The NLP recovered to baseline at 3 months. The distance NFV decreased significantly from 8∆ (IQR, 6 to 10∆) at baseline to 7∆ (IQR, 6 to 8∆) at 1 week (p = 0.007), whereas the near NFV decreased significantly from 21∆ (IQR, 15 to 24∆) at baseline to 16∆ (IQR, 13 to 19∆) at 1 week (p<0.001). Both distance and near NFV remained at the reduced level through to 6 months postoperatively. The VF was 9 cpm (IQR, 7 to 12 cpm) at baseline and increased to 10 cpm (IQR, 9 to 16 cpm) at 3 months (p = 0.004) and 12 cpm (IQR, 9 to 15 cpm) at 6 months (p = 0.003) postoperatively. No statistically significant differences were observed in DLP, distance PFV, near PFV, or NPC between preoperative and postoperative visits.
Table 2. Time course of phoria and vergence parameters.
Preoperative Postoperative Wald χ2 pa 1 Week 1 Month 3 Months 6 Months DLP −1 (−3, 1) 0 (−2, 1) 0 (−2, 2) −1 (−1, 2) −1 (−2, 2) 8.961 0.062 pb 0.554 0.107 1.000 1.000 NLP −5 (−8, 0) −1 (−5, 3) −3 (−6, 3) −3 (−8, −1) −3 (−7, −1) 54.819 <0.001 pb 0.001 0.008 0.432 1.000 NFV (distance) 8 (6, 10) 7 (6, 8) 7 (6, 8) 7 (5, 8) 6 (5, 7) 28.413 < 0.001 pb 0.007 0.010 0.009 0.001 PFV (distance) 18 (12, 24) 19 (16, 24) 20 (16, 26) 19 (13, 23) 16 (9, 22) 2.349 0.672 pb 1.000 1.000 1.000 1.000 NFV (near) 20 (15, 24) 16 (13, 19) 17 (12, 20) 16 (14, 20) 16 (13, 21) 66.526 < 0.001 pb < 0.001 < 0.001 < 0.001 < 0.001 PFV (near) 33 (22, 36) 32 (24, 36) 30 (24, 35) 31 (22, 36) 30 (25, 36) 4.902 0.298 pb 1.000 1.000 1.000 1.000 NPC 6.0 (6.0, 7.0) 6.0 (6.0, 8.0) 6.5 (6.0, 8.0) 6.0 (6.0, 8.0) 6.5 (6.0, 8.0) 4.156 0.385 pb 0.297 0.798 1.000 0.920 VF 9 (7, 12) 10 (8, 14) 11 (8, 14) 10 (9, 16) 12 (9, 15) 23.065 < 0.001 pb 0.086 0.092 0.004 0.003 Data are expressed as the median (Quantile 1, Quantile 3). DLP, distance lateral phoria; NLP, near lateral phoria; NFV, negative fusional vergence; PFV, positive fusional vergence; NPC, near point of convergence; VF, vergence facility. pa-values represent the overall significance across all time points (GEE). pb-values represent the differences between the baseline and each postoperative follow-up visit, respectively. 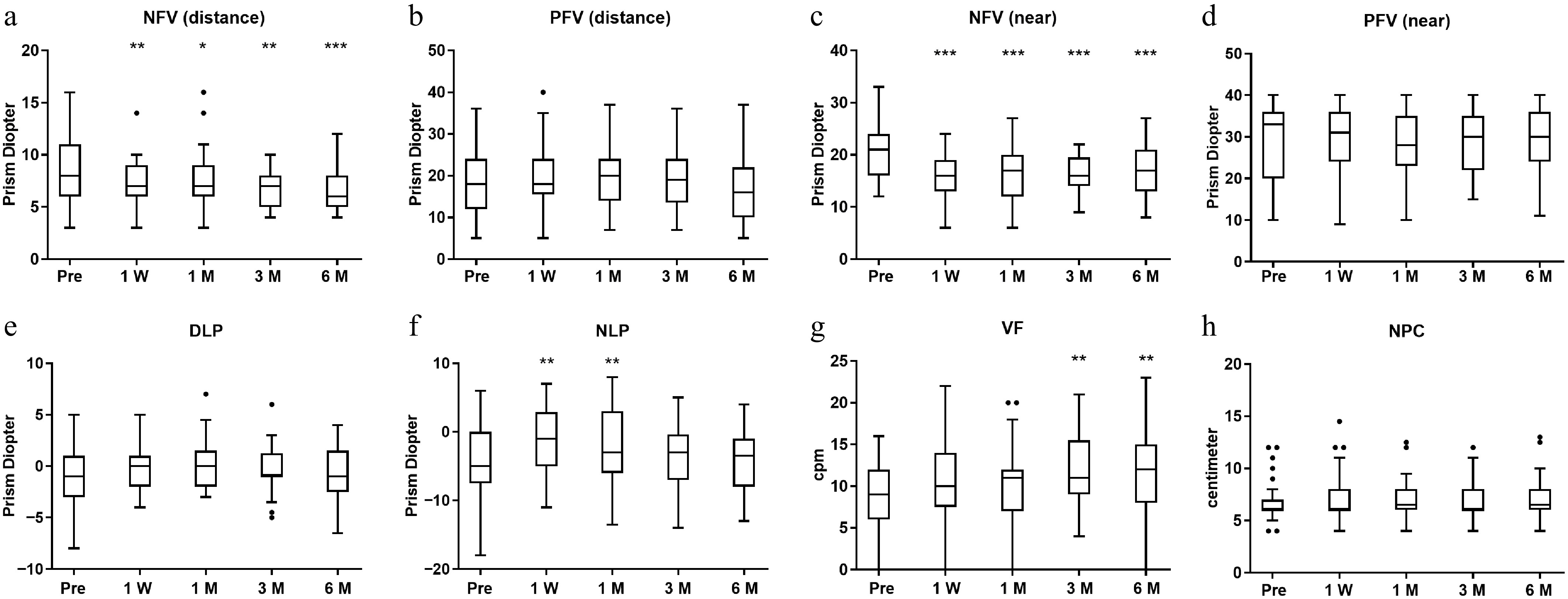
Figure 2.
Time course of phoria and vergence parameters. NFV, negative fusional vergence; PFV, positive fusional vergence; DLP, distance lateral phoria; NLP, near lateral phoria; NPC, near point of convergence; VF, vergence facility; cpm, cycles per minute.
-
In this study, we evaluated the parameters of accommodation and vergence in the high myopic patients who accepted ICL implantation. We found that AMP and NFV decreased after ICL implantation and remained reduced through 6 months. PRA, AF, and NLP decreased in the early postoperative period but recovered gradually. Notably, both AF and VF slightly increased at 3 months after the operation.
Accommodative function can be affected by different refractive corrective methods. Several previous studies have consistently reported that AMP decreased in the early stage following various refractive surgeries[8,11,18]. Interestingly, ICL implantation may result in lower postoperative AMP compared with patients undergoing corneal refractive surgery[19]. Kamiya[14] reported that AMP reduced from 1 to 6 months after ICL implantation, and recovered at 1 year postoperatively. Similarly, our study demonstrated that the AMP reduced from 1 week through to 6 months after surgery (Fig. 1a). Although the material of ICL is flexible, the haptics may exert lateral pressure on the ciliary body, subtly altering its morphology[20,21]. This mechanical constraint could potentially resist ciliary muscle contraction during accommodation. However, Li et al. found no significant change in AMP[13], possibly because their cohort comprised moderate myopic patients, whereas both Kamiya[14] and our research focused on high myopic patients. Different degrees of myopia may be associated with varying accommodative dysfunctions and differential recovery patterns following ICL implantation[15]. These findings suggested that accommodation should be taken into account both preoperatively and postoperatively, especially in high myopia.
There have been few studies about the change in vergence function after refractive surgery. In the present study, we found both distance and near NFV decreased after the operation (Fig. 2a, c), although distance and near PFV did not change (Fig. 2b, d). These findings were partially consistent with previous reports. Lopez-Artero[22] found no statistically significant changes in near convergence amplitude after ICL implantation. Han et al.[7] found that near convergence amplitude decreased during early postoperative period and recovered at 3 months in moderate myopia after laser refractive surgery. The amplitude of vergence could be affected by the convergence demand and the prismatic effect of the lens. The prismatic effect of the minus lens could reduce the convergence demand when looking through spectacles at near range. This effect disappeared, since the patients do not wear spectacles after surgery, followed by the recovery of convergence demand. Thus, the increasing convergence demand led to reduced NFV, with the near NFV reducing more than the distance NFV in our findings. In contrast, PFV remained stable, likely because the patients had adequate baseline convergence reserves preoperatively, allowing them to compensate for increased convergence demands after surgery.
PRA, AF, and NLP decreased in the early stage after surgery in our study (Figs. 1c, d, 2f). Similar temporary changes in accommodative and vergence function have been reported in previous studies. Li et al.[23] found that patients with near vision fatigue had lower preoperative PRA and AF; these functions further declined 1 week postsurgery but improved after 1 month of training. Haiting[4] found that AF decreased 1 week postoperatively and returned to the baseline at 1 month, and AF correlated with asthenopia symptoms. Zhou[11] found that AF and horizontal phoria reduced at 1 week after femtosecond laser-assisted laser in situ keratomileusis (FS-LASIK), and returned to the baseline after 1 month. These early postoperative changes may be attributed to increased accommodative demand following full refractive correction. Many high myopic patients habitually undercorrect with spectacles, which reduce accommodative effort during near tasks. After refractive surgery, accommodative demand increases abruptly, leading to temporary reductions in accommodative and vergence performance. In addition, sudden changes in accommodative and convergence demands may induce vergence–accommodation conflict, which has been identified as a contributor to visual fatigue[24,25]. However, this conflict is usually resolved through neural adaptation in short term[26], which is consistent with the transient functional changes observed in our study.
Interestingly, AF and VF improved at 3 months postoperatively (Figs. 1d, 2g). Chen[12] found that both monocular and binocular accommodative facility improved after ICL implantation. Various responses of AF have previously been reported in laser refractive surgery[9,27]. In the present study, the AF reduced at 1 week postoperatively, recovered at 1 month, and increased after 3 months, whereas the VF increased after 3 months. The increase in AF and VF might because of improvement in visual quality and change in magnification change. A minus lens has a minification effect on the visual image. High myopia patients with spectacles might have a smaller visual image and less visual information. With elimination of the spectacles-related minification effect, better visual information and stereo perception led to the faster response of accommodation and vergence[28,29].
The accommodative and vergence functions are correlated with the neural system. Lv et al. reported that patients with accommodative asthenopia had regional brain dysfunction, including in the cerebellum, brainstem, frontal lobe, postcentral gyrus, caudate nucleus, median cingulate, paracingulate gyri, and precentral gyrus[30]. Accommodative and vergence therapy can improve the convergence insufficiency patients' PFV and NPC, which are correlated with the region of interest pair of right-supplementary eye fields–right-parietal eye fields[31]. Similarly, visual training improved NPC, PFV, and VF in patients with concussion-related convergence insufficiency, whereas functional activity increased in the vergence oculomotor network, visual cortex, and cerebellar vermis[6]. In our study, transient and sustained alternations were observed in accommodative and vergence functions. However, whether these alternations correlated with neural adaptation or changes in the brain's functional activity is still unclear. Further studies that connect binocular visual functions and the neural system in high myopic patients undergoing ICL implantation are needed.
To provide a comprehensive perspective on the field, we summarized the longitudinal changes in binocular function across various refractive surgical platforms in Table 3. This comparative overview demonstrates that although LASIK, small incision lenticule extraction (SMILE), and ICL all aim to correct refractive error, they lead to diverse patterns of functional adaptation because of their distinct optical and anatomical impacts. Our findings align with several reports on ICL implantation regarding the reduction in accommodative amplitude[4,19], yet they contrast with certain corneal refractive studies where accommodative parameters may stabilize or improve postoperatively[9,19].
Table 3. Summary of binocular visual function changes across various refractive procedures.
Author (year) Surgery Key findings Proposed mechanisms Current study ICL Decreased AMP and NFV; improved AF and VF. Shift in the principal planes; change in retinal image magnification; neural adaptation. Li (2025) SMILE Decreased PRA and AF at 1 week. Related to the stimulation of corneal nerve function and acute refractive change. Haiting (2023) ICL Decreased AMP and AF at 1 week; improved at
3 months.Surgical trauma; inflammatory reactions; training-induced recovery. Long (2022) SMILE and ICL AMP decreased in the ICL group but remained stable in the SMILE group. Comparison of mechanical interaction between the haptics of the ICL and the ciliary muscle (ICL group) versus corneal remodeling (SMILE group). Sivaraman (2021) LASIK Decreased AMP; increased AF and NPC at
1 month.Improved accommodative accuracy and reduced depth of focus after correction. Karimian (2010) PRK Increased AMP and AF at 3 months. Influence of depth of focus, ocular aberrations, and ciliary body function. Prakash (2007) LASIK Decreased AC/A at 1 month; recovered by
3–9 months.Postoperative adjustment of accommodative effort to the new emmetropic state. AC/A, accommodative convergence/accommodation; AMP, amplitude of accommodation; AF, accommodative facility; NFV, negative fusional vergence; PRA, positive relative accommodation; NPC, near point of convergence. To our knowledge, this study is the first to report that NFV decreased and VF increased after ICL implantation in high myopic patients. Although the changes in accommodative and vergence were statistically significant, the parameters remained within the clinically normal ranges. In the present study, the alterations in AMP, PRA, AF, NLP, and both distance and near NFV primarily occurred during the early postoperative stage, a period that coincides with the typical onset of transient visual fatigue and difficulties in near-work adaptation. Although these parameters remained within clinically normal ranges, the suddenly significant reduction in factors associated with the near reflex triad (such as AMP, PRA, NLP, and near NFV) may diminish the accommodative and vergence reserves. Such changes could offer a potential physiological insight into the temporary visual discomfort reported by patients before full neuroadaptation is achieved. However, the alterations in AMP, NFV, AF, and VF need to be evaluated in the long term to determine their clinical effects. It is important to note that postoperative visual fatigue may also be influenced by factors unrelated to binocular visual functions, including dry eye, optical aberrations, and glare, which are common after refractive surgery[32]. Therefore, the contribution of changes in vergence to subjective symptoms requires further investigation.
Several limitations of this study should be acknowledged. First, although the sample size met the requirements of our a priori power analysis, it remains relatively small; larger multicenter studies would be beneficial to confirm these findings. Second, although we tracked patients for 6 months, a longer follow-up period is necessary to determine the long-term stability of these changes in binocular function. Third, as indicated by the clinical relevance, we did not used standardized subjective symptom questionnaires, such as the Convergence Insufficiency Symptom Score (CISS). The lack of patient-reported outcomes limits our ability to directly correlate objective functional shifts with the degree of subjective visual fatigue. Lastly, this was a prospective observational study without a control group. Consequently, we could not entirely isolate the mechanical effects of the ICL from the optical changes inherent in any refractive correction. Future research incorporating control groups and validated symptom scales is warranted to further clarify these mechanisms.
-
In summary, ICL implantation in high myopia induces sustained decreases in AMP and NFV; transient decreases in PRA, AF, and NLP; and subsequent improvement in AF and VF. Although these changes remained within the normal clinical ranges, long-term follow-up is required to evaluate their clinical effects. It is necessary to establish a binocular visual function evaluation criterion for high myopic patients undergoing refractive surgery, which might offer insights into the mechanisms of postoperative visual fatigue and guide the timing of individualized visual training.
-
This study was approved by the Ethics Committee of the Zhongshan Ophthalmic Center, Sun Yat-sen University (No.2022KYPJ198) on 30 October 2022, and followed the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants.
-
The authors confirm their contributions to the paper as follows: study conception and design: Lei L, Hou F, Zhuo Y; data collection: Lin J, Zhan J; analysis and interpretation of results: Lin J, Chen J; draft manuscript preparation: Lin J, Li Z, Xie R, Zhang Y; project administration: Zhu Y. All authors reviewed the results and approved the final version of the manuscript.
-
The data that support the findings of this study are available on request from the corresponding author (Zhuo Y).
-
This study was supported by the National Natural Science Foundation of China (82471074), the Guangdong Basic and Applied Basic Research Foundation (2024A1515013058), the Guangdong Basic Research Center of Excellence for Major Blinding Eye Diseases Prevention and Treatment (2024-PIZC-022), the Science and Technology Program of Guangzhou, China (202206080005), and the Major Science and Technology Project of Zhongshan City (2022A1007). The funding bodies had no role in the design of the study; in the collection, analysis or interpretation of the data; or in writing the manuscript.
-
The authors declare that they have no conflict of interest.
-
Authors contributed equally: Junxiong Lin, Zhidong Li
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Lin J, Li Z, Zhan J, Xie R, Zhang Y, et al. 2026. Accommodation and vergence changes after implantable collamer lens implantation in high myopia. Visual Neuroscience 43: e026 doi: 10.48130/vns-0026-0025 

Accommodation and vergence changes after implantable collamer lens implantation in high myopia
- Received: 30 March 2026
- Revised: 06 May 2026
- Accepted: 22 May 2026
- Published online: 29 June 2026
Abstract: The ocular motor functions, including accommodation and vergence, are correlated with extensive brain regions. These functions may change after refractive surgery, but this is unclear in implantable collamer lens (ICL) implantation. To assess the accommodative and vergence functions after ICL implantation, 35 high myopic patients were enrolled. Accommodative and vergence functions were assessed preoperatively and 1 week, 1 month, 3 months, and 6 months postoperatively. The amplitude of accommodation reduced from 13.33 D (interquartile range [IQR], 11.11 to 15.38 D) preoperatively to 10.00 D (IQR, 9.09 to 12.50 D) at 1 week (p < 0.001). The distance negative fusional vergence reduced from 8∆ (IQR, 6 to 10∆) preoperatively to 7∆ (IQR, 6 to 8∆) at 1 week (p = 0.007). The near negative fusional vergence reduced from 21∆ (IQR, 15 to 24∆) preoperatively to 16∆ (IQR, 13 to 19∆) at 1 week (p < 0.001). These parameters remained at the reduced level through 6 months. The positive relative accommodation reduced from –2.50 D (IQR, –3.75 to –2.50 D) preoperatively to –2.25 D (IQR, –2.75 to –1.75 D) at 1 week (p = 0.003) and recovered at 1 month. The accommodative facility reduced from 9 cpm (IQR, 6 to 11 cpm) preoperatively to 7 cpm (IQR, 4 to 9 cpm) at 1 week (p = 0.039), but increased to 9 cpm (IQR, 7 to 12 cpm) at 3 months (p = 0.006). The near phoria reduced from –5∆ (IQR, –8 to 0∆) preoperatively to –1∆ (IQR, –5 to 3∆) at 1 week (p = 0.008) and recovered at 3 months. The vergence facility increased from 9 cpm (IQR, 7 to 12 cpm) preoperatively to 10 cpm (IQR, 9 to 16 cpm) at 3 months (p = 0.004). ICL implantation in high myopia induces alterations in binocular visual functions. It suggests the requirement to establish a binocular visual function evaluation criterion for high myopic patients undergoing refractive surgery, which may provide a potential physiological basis for understanding postoperative visual fatigue.
-
Key words:
- Accommodation /
- Vergence /
- Implantable collamer lens /
- High myopia