









-
High myopia is an extreme form of myopia, typically defined as a condition in which the spherical equivalent (SE) refractive error of an eye is ≤ −6.00 D when ocular accommodation is relaxed[1]. High myopia accounts for around 10-20% of myopes and has a high incidence, exceeding 2% in junior high school[2,3]. In recent decades, the prevalence of myopia and high myopia among school-aged children has surged dramatically[3,4]. It is estimated that by 2050, nearly half of the global population will be affected by myopia, with a quarter of the population suffering from high myopia[4,5].
High myopia is closely associated with the risk of developing sight-threatening pathologies[6,7], including early-onset cataracts, glaucoma, retinal detachment, posterior staphyloma, and myopic maculopathy[8−12]. Studies have shown that high myopia is a major risk factor for glaucoma, with a 7.3-fold increase in risk compared to emmetropic eyes[13]. The risk accelerates starting at −6.00 D and increases more sharply beyond −8.00 D[14]. However, while high myopia and glaucoma both cause optic nerve damage, optic nerve changes associated with high myopia have been less thoroughly investigated in the literature. Advances in imaging technologies, such as optical coherence tomography (OCT) and optical coherence tomographic angiography (OCTA), have facilitated the study of progressive changes in eyes with high myopia, including alterations in the optic nerve head (ONH) and thinning of the retinal nerve fiber layer (RNFL)[15]. Standardized definitions and consensus regarding the morphological and functional changes of the optic nerve in highly myopic eyes are urgently required with these technological advancements.
Therefore, this paper summarizes optic neuropathy associated with high myopia, including the morphological changes in the optic disc, peripapillary region, and retinal layers, as well as the functional changes associated with myopic optic neuropathy (MON). Furthermore, artificial intelligence (AI)-driven research on MON is reviewed, with a discussion of the challenges and future directions. By deepening the understanding of MON, this work aims to pave the way for more effective diagnostic and management strategies.
-
The optic disc, defined as the entirety encompassing the lamina cribrosa (LC) at its base, can be characterized morphologically by its size and shape[16].
Optic disc size, when observed in color fundus photography (CFP), refers to the visible part of the neuroretinal rim and optic cup, while in OCT, the optic disc margin is defined by the end of the LC, specifically the peripapillary Elschnig border tissue of the peripapillary scleral flange (Fig. 1)[17,18]. Compared to normal ONHs, high myopic eyes (myopic refraction of less than −8.00 D) typically have larger discs[19]. However, some studies have reported a reduction in CFP disc size in high myopia, with a prevalence rate of 33.7%[18]. This difference may be related to changes in Bruch's membrane opening (BMO) during axial elongation: in high myopic eyes, BMO shifts toward the fovea, causing Bruch's membrane (BM) to overhang into the nasal intrapapillary region, obstructing the visibility of the optic cup in the nasal area and making the optic disc appear smaller. As axial elongation progresses, BMO not only shifts but also recedes, exposing the LC, which leads to an increase in the CFP-visible part of the optic disc. Another factor contributing to optic disc enlargement is the elongation and thinning of the LC itself[16]. These changes can reduce the distance between intraocular pressure (IOP) and retrobulbar pressure, steepening the pressure gradient and increasing the risk of glaucoma-like optic neuropathy[17].
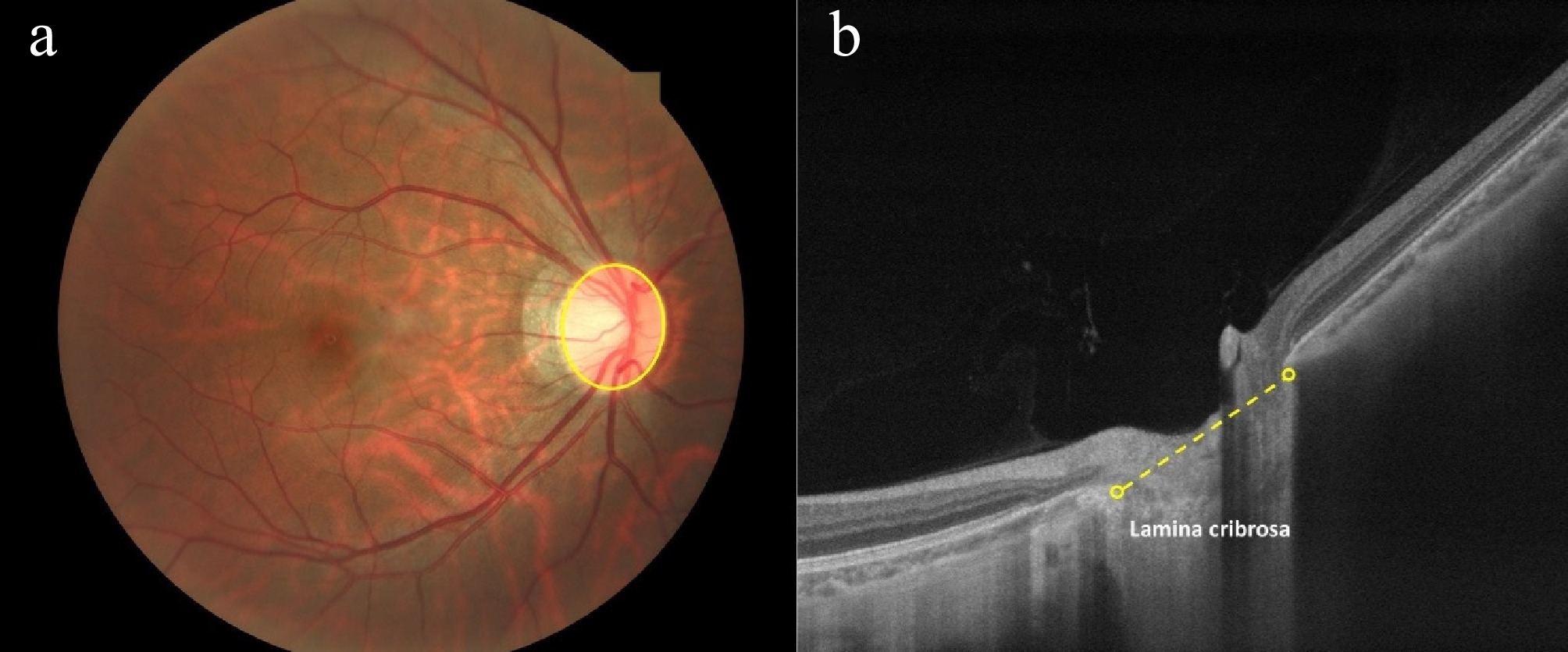
Figure 1.
Optic disc size definitions in different ophthalmic modalities. (a) Color fundus photography: The optic disc is outlined by the visible part of the neuroretinal rim and optic cup (yellow oval). (b) Optical coherence tomography: The optic disc size is measured at the end of the lamina cribrosa, specifically the peripapillary Elschnig border tissue of the peripapillary scleral flange (yellow dashed line). (Source: Personal fundus images provided by Mr. Jinze Zhang, Sun Yat-sen University).
Changes in optic disc shape are primarily characterized by tilting (or ovality) and rotation (or torsion). Due to axial elongation-induced tension on the sclera, the optic disc may tilt, often accompanied by rotation. This rotation misaligns the vertical or horizontal axis of the disc, making it appear oval rather than the typical round shape[20]. The definition of optic disc tilting varies across studies. Early criteria included Fuchs' coloboma, inverse-type vessels, or subjective elevation of one disc margin over the opposite margin[21−23]. A commonly used criterion is the ratio between the longest and shortest diameters of the disc[24−26]. Patients with a tilting ratio exceeding 1.30 are typically classified as having tilted discs[27]. Temporal and superotemporal tilt are the two main directions of disc tilt[28]. The rate of optic disc tilting in high myopic eyes may vary by ethnicity. For example, 81.2% of Chinese patients with high myopia exhibit optic disc tilting, while 57.4% was observed in Singaporean patients using the same criteria[20,24]. However, the age groups in these two studies were not identical, and both populations were Asian, suggesting the need for more diverse population data to support the conclusion. The degree of disc tilt also varies among different ethnicities, with Asian eyes showing the greatest tilt and White eyes showing the least[29]. The degree of disc tilting has been shown to correlate with longer axial length (AL), higher SE, and the presence of posterior staphyloma in high myopia[30,31]. The definition of optic disc rotation lacks strict standardization and is typically defined by the angle between the long axis of the disc and the vertical meridian. Some studies consider a rotation greater than 0° as rotated and a rotation exceeding 15° as 'significant'[27,32]. However, more commonly, a rotation with > 15° indicates rotation. A positive value denotes clockwise rotation, while a negative value indicates counterclockwise rotation in the right eye[33]. Li et al.[20] reported that 48.3% of Chinese patients with high myopia had rotated optic discs, with inferior rotation being the most common (85.5%). Greater absolute cylindrical power was identified as a risk factor for a higher degree of rotation. Another study indicated that the torsional direction of the optic disc was associated with variations in RNFL measurements[34]. For instance, a more temporally directed optic disc torsion angle was correlated with thicker temporal RNFL and thinner superior RNFL, suggesting a redistribution effect rather than an overall loss.
Parapapillary changes
-
Parapapillary zones, previously described as peripapillary atrophy (PPA), are commonly seen in myopia but are not exclusive to myopic optic neuropathy (MON); they can also occur in myopia-associated glaucoma (MAG)[16]. The significance of different types of parapapillary zones, including beta, gamma, and delta zones, is key to understanding the pathology of both conditions (Fig. 2). The beta zone, characterized by the presence of BM and absence of retinal pigment epithelium (RPE), is linked to an increased risk of glaucomatous damage[35]. Studies show that myopic glaucoma patients exhibit significantly larger beta zones compared to myopic controls[36]. This may be due to mechanical stress at the optic disc border, associated with changes in IOP, leading to RPE cell loss and beta zone formation.[37] The gamma zone, defined as the area around the optic disc where BM and RPE are absent, is strongly associated with myopia, particularly with axial elongation of the eye[38]. An epidemiological study in Tokyo found detection rates of 71.5% for gamma zones in individuals aged 13−90 with high myopia[39]. The gamma zone increases significantly with AL, and this relationship is nonlinear, with a sharp rise in prevalence once AL reaches about 26.5 mm[40]. Research indicates that myopic glaucoma patients tend to have smaller gamma zones than myopic controls[36]. Although there are differences in the size and distribution of the beta and gamma zones between MON and MAG, these features do not significantly aid in distinguishing the two conditions, at least in Caucasian populations[36]. Further studies in different ethnic groups may provide more insights. The delta zone, considered part of the gamma zone, refers to the thinning and elongation of the peripapillary scleral flange[17]. This zone may affect the biomechanical stability of the LC, increasing glaucoma susceptibility in high myopia[38].
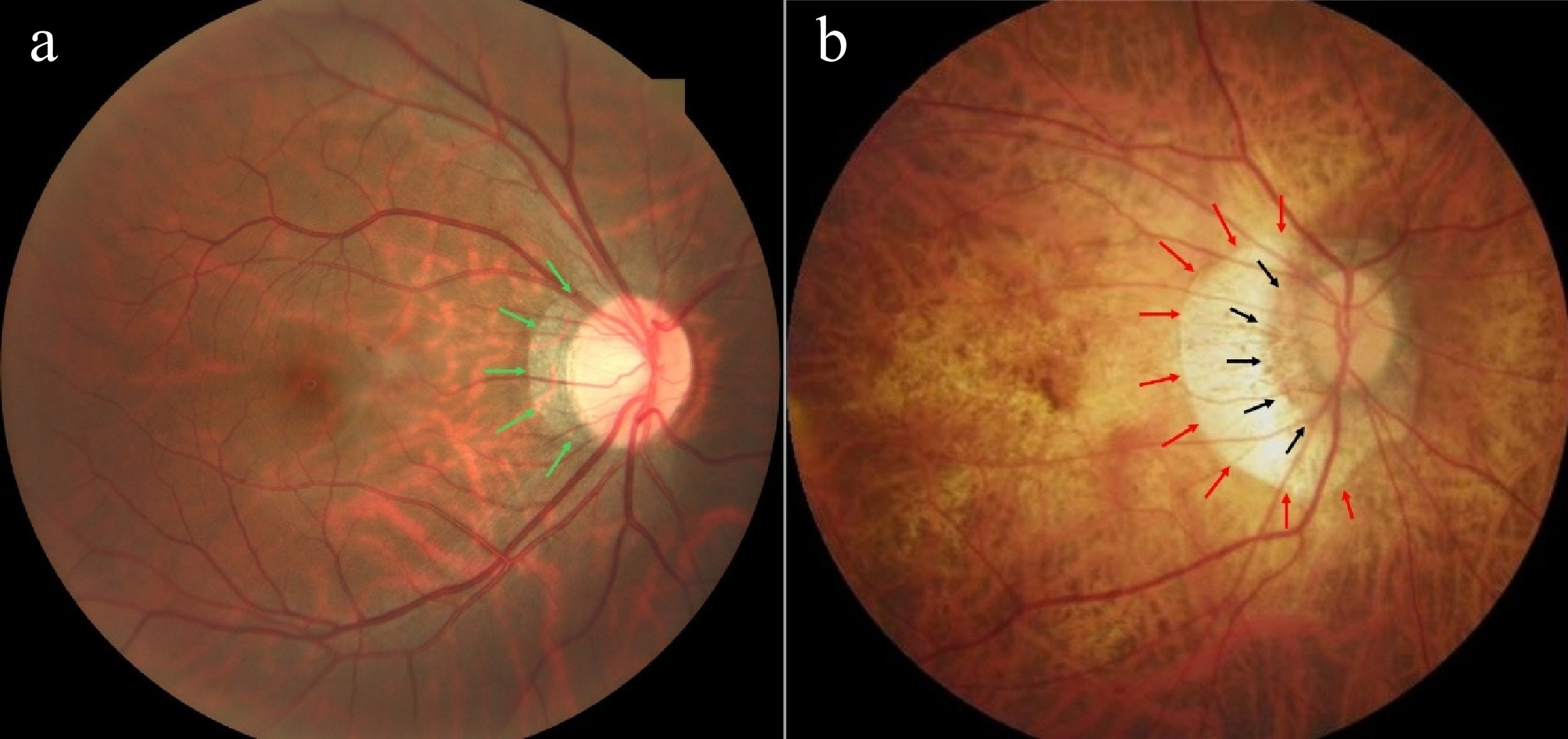
Figure 2.
Illustration of different parapapillary zones in color fundus photography. (a) Beta zone (green arrows) refers to the presence of Bruch's membrane (BM) and the absence of retinal pigment epithelium (RPE). (b) Gamma zone (red arrows) refers to the area around the optic disc where BM and RPE are absent; Delta zone (black arrows) refers to the thinning and elongation of peripapillary scleral flange. (Source: HPMI database,
https://doi.org/10.6084/m9.figshare.24800232.v1 ).In addition to parapapillary zones, several studies have investigated ultrastructural changes related to BM in high myopia, including Bruch's membrane opening distance (BMOD), border length (BL), border tissue angle (BTA), focal LC defects, and peripapillary intrachoroidal cavitation (PICC) (Fig. 3). The BMOD is defined as the distance between the two points of the BMO on a horizontal B-scan, taken across the midpoint of the optic disc's longest axis. The BL refers to the straight-line distance from the temporal BMO point to the border tissue and the scleral termination. The BTA is defined as the angle formed between the reference plane of the BMO and the border tissue[33]. Hu et al.[41] found that in young adults aged 16−28 years with high myopia, BMOD and BL were longer, while BTA was smaller. Axial length (AL) was positively correlated with BMOD and BL and negatively correlated with BTA. As myopia progresses, the increase in BMOD and the decrease in BTA precede the expansion of the PPA area and subsequent globe deformation. This suggests that, compared to the PPA, BMOD and BTA were considered earlier indicators of fundus changes in high myopia. In contrast, a study by Kim et al.[42] in children aged 6.7−12.5 years found that during changes in the ONH and PPA, BL increased nasally, and BTA decreased, whereas BMOD remained relatively stable. They suggested that in children, physiological growth might counterbalance rapid axial elongation, and structural changes in BMOD may not be as pronounced at this stage.
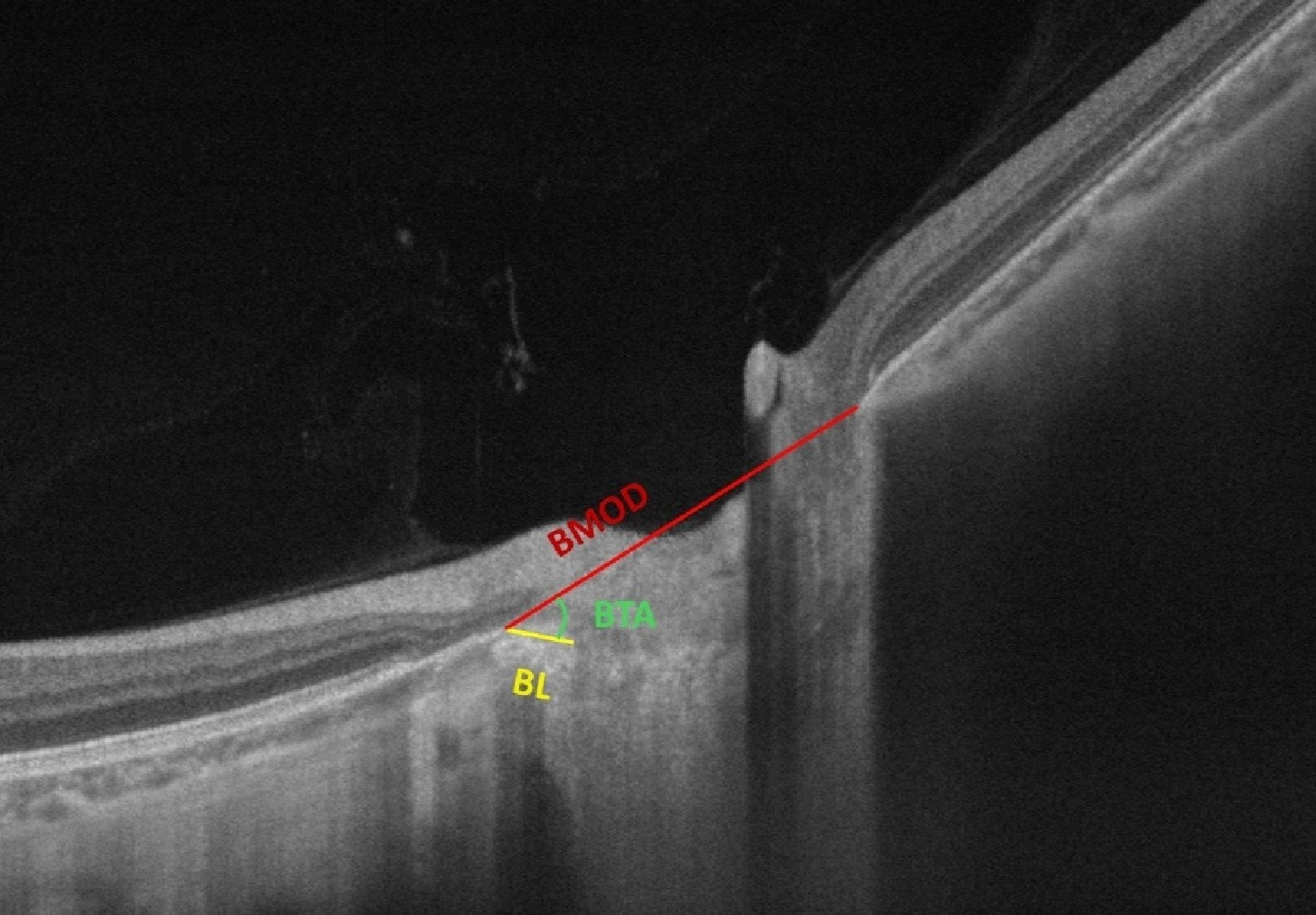
Figure 3.
Illustration of Bruch's membrane opening distance (BMOD), border length (BL), and border tissue angle (BTA) in optical coherence tomography. BMOD refers to the distance between the two points of the Bruch's membrane opening (BMO) on a horizontal B-scan; BL refers to the straight-line distance from the temporal BMO point to the border tissue and the scleral termination; BTA refers to the angle formed between the BMOD line and the BL line. (Source: Personal fundus images provided by Mr. Jinze Zhang, Sun Yat-sen University).
Focal LC defects are defined as irregularities in the anterior laminar surface that disrupt the normal smooth, curvilinear contour, with a maximal diameter greater than 100 µm and a depth greater than 30 µm, visible in at least two neighboring line scans[43]. Previous studies have shown that such defects play a key role in the development and progression of glaucomatous optic neuropathy, typically associated with increased IOP and optic disc remodeling, reflecting the neurodegenerative pathological features of glaucoma[43,44]. Notably, LC defects can also occur in myopic eyes independent of glaucoma, potentially caused by axial elongation and increased pressure on the ONH. While myopia itself may not worsen LC defects in glaucoma patients, it could indirectly increase glaucoma risk by enhancing the optic disc's sensitivity to IOP[45].
Peripapillary intrachoroidal cavitation (PICC), originally described as peripapillary detachment in pathologic myopia, refers to cavitated spaces within the peripapillary choroid[46,47]. In Chinese high myopia cohorts, PICC prevalence is 3.6%, predominantly inferior to the optic disc (87.5%). The underlying mechanism may involve progressive scleral stretching secondary to axial elongation. Multiple factors demonstrate associations with PICC presence, including advanced age, longer AL, greater SE, higher stages of myopic maculopathy, and the existence of posterior staphyloma[48].
Retinal nerve fiber layer changes
-
Change in RNFL is a key feature of high myopia, occurring both in the peripapillary region and the macular area[49,50]. Several studies have demonstrated that the peripapillary RNFL (pRNFL) is thinner in myopic eyes compared to healthy controls[51,52]. This thinning exhibits sectoral variations, with the inferior, superior, and nasal quadrants being thinner, while the temporal quadrant often shows increased thickness. Regarding the macular RNFL, studies suggest that its thickness may increase. This increase is likely due to the temporary displacement of the RNFL toward the macula during axial elongation[53,54]. Sezgin et al.[55] explained that the papillomacular bundles are located in the temporal quadrant, and as myopia progresses, the superotemporal and inferotemporal RNFL bundles converge temporally, which helps preserve temporal RNFL thickness despite axial elongation. Additionally, the reduction in mean pRNFL thickness in high myopia is notably more pronounced within a two-year period compared to normal eyes[49], indicating that pRNFL thickness may be more sensitive to temporal changes in high myopia. As for the correlation between RNFL and other myopia parameters, studies show that RNFL thickness decreases with increasing AL and higher myopia[56,57]. Abdolrahimzadeh et al. demonstrated that in high myopia patients without myopic maculopathy, overall pRNFL thickness is an independent predictor of best-corrected visual acuity[58], further emphasizing the clinical relevance of pRNFL changes in high myopia. It is worth noting that the elongation of the AL can lead to a reverse magnification effect in OCT image measurements, which may result in deviations in the RNFL thickness[51]. This could be one reason why some early studies found no change in RNFL thickness in patients with high myopia[59,60]. Littmann or Bennett's formulas, by quantifying the relationship between AL and optical parameters, can partially correct measurement errors[61,62]. However, since the Bennett-Littmann method primarily accounts for AL alone, the incorporation of additional optical elements of the eye (e.g., corneal curvature, lens thickness) may further improve the estimation of magnification effects[63]. Future standardization should involve establishing stratified normative databases across AL intervals to optimize correction coefficients, ultimately enabling precise evaluation of authentic RNFL changes in high myopia populations.
Ganglion cell layer and inner plexiform layer changes
-
High myopia also affects the ganglion cell-inner plexiform layer (GC-IPL), which consists of ganglion cell bodies and dendrites[55]. High myopic eyes tend to have thinner GC-IPL and a significantly greater reduction in GC-IPL over a 3-year period when compared with normal eyes[64]. This thinning is uneven across quadrants. Seo et al.[65] found that the GC-IPL in the temporal region was thinner than in the nasal region in myopic eyes, suggesting that the temporal region may be more affected by axial elongation. Changes in macular GC-IPL thickness in high myopia may offer greater diagnostic and glaucoma progression-monitoring potential than peripapillary RNFL thickness[66]. For instance, studies have identified inferotemporal macular GC-IPL thickness as the best parameter for the detection of preperimetric glaucoma in myopic eyes, distinguishing glaucoma in myopia[67]
Other studies combined the GC-IPL and the RNFL into the ganglion cell complex (GCC) for analysis, using parameters including GCC values, focal loss volume (FLV) and global loss volume (GLV). GCC values refer to the distance from the internal limiting membrane to the inner plexiform layer; FLV represents the percentage of significant GCC loss within the mapped area, while GLV indicates the overall tissue loss in the region[55,68]. Compared to moderate and low myopia, high myopia exhibits significantly lower average, superior, and inferior GCC values, along with FLV and GLV[55]. Zhao et al.[68] explored the relationship between GCC parameters and AL and found that the average and inferior GCC thicknesses were significantly correlated with AL. This relationship between GCC and AL is similar to that observed between RNFL thickness and AL, likely due to axial elongation and thinning of the ocular wall, leading to a relatively thinner GCC in high myopia[55].
-
Studies have focused on changes in ocular blood flow in myopia, using OCTA to automatically identify and record key metrics of retinal and choroidal vascular circulation, such as vessel density (VD) and microvascular dropout (MvD)[69−72]. Radial peripapillary capillary vessel density (RPC-VD) is a common parameter of retinal blood flow, with VD representing the length of vessels per unit area and reflecting the number of blood vessels. Studies have shown that RPC-VD is reduced in high myopic adults and negatively correlated with AL[69]. Similar findings have been observed in children. Lin et al.[71] reported that RPC-VD was lower in high myopic children than in emmetropic children, except in the temporal region. Furthermore, RPC-VD in the nasal inferior, nasal superior and superior nasal regions adjacent to the optic disc was negatively associated with AL. Two main hypotheses have been proposed to explain the mechanism of reduced retinal VD: one suggests that excessive axial elongation leads to retinal thinning, which in turn reduces oxygen demand and decreases blood circulation; the other argues that axial elongation simultaneously causes retinal thinning and a reduction in VD. Despite the lower peripapillary VD, high myopia patients show similar values for inside disc vessel density (iVD) compared to normal controls[70]. This suggests that the reduction in VD is more closely related to axial elongation rather than a direct consequence of thinning of posterior pole structures (retina, sclera, and choroid). However, the causal relationship between these factors remains unclear—whether morphological changes precede microvascular alterations or occur simultaneously requires further investigation[72]. Notably, the elongated AL in high myopia poses inherent imaging challenges. Morphological changes, such as staphyloma, can disrupt segmentation algorithms, causing misalignment of retinal layers and subsequent distortion of VD measurements[73,74]. Fu et al.[75] proposed a magnification correction approach for macular VD quantification in high myopia. However, their findings from a small cohort (n = 47) need to be validated in larger, multicenter studies. Future protocols should integrate AL-adjusted OCTA calibration, high myopia-specific segmentation benchmarks, and advanced artefact correction algorithms to measure microvascular changes accurately.
In addition to retinal vascular changes, studies have also explored choroidal capillary circulation in high myopia. MvD refers to small dark areas in fundus blood vessels seen in OCTA images, representing gaps between capillaries and reflecting microvascular changes in the choroid of high myopic eyes. Lei et al.[70] found that MvD is more common in high myopia patients than in those with mild to moderate myopia, and this is associated with factors such as age, AL, SE, and PPA-beta area.
-
Morphological changes in high myopia often correspond to functional changes, and visual field defect (VFD) is an important functional indicator for assessing optic nerve damage[76]. The prevalence of VFD in high myopic individuals may vary by region. For example, in Denmark, 42% of high myopic individuals exhibited VFD over a 10-year period[77]. Another 8-year study in China found that 49.4% of non-pathological high myopic eyes developed VFD.[78] The Glaucoma Suspects with High Myopia Study Group proposed a novel classification system to describe VFD patterns in non-pathologic high myopia[79]. The VFD patterns are categorized into three types: glaucoma-like defects (paracentral defect, nasal step, partial arcuate defect, arcuate defect), high myopia-related defects (enlarged blind spot, vertical step, partial peripheral rim, nonspecific defect), and combined defects (nasal step with enlarged blind spot). Furthermore, Li et al.[78] reported the long-term patterns of VFD development in individuals with non-pathological high myopia using the same classification system. They found that enlarged blind spots and nonspecific defects were the most common visual field abnormalities, followed by nasal step defects, partial arcuate defects, paracentral defects, and other types of VFD. Enlarged blind spots may be attributed to parapapillary zones and/or optic disc tilting[80], causing the optic disc margin to extend beyond the normal blind spot in static visual field testing. Nonspecific defects may result from the irregular stretching and distortion of the RNFL during the progression of high myopia[81]. Nasal step, partial arcuate defects, and paracentral defects are also commonly observed in glaucoma patients. Some studies suggest that the progression of high myopia and glaucoma may not be independent, but may interact with each other[82], although this relationship requires further investigation. Regarding the relationship between VFD and high myopia morphological parameters, longer AL, thinner central corneal thickness, worse mean deviation of the visual field, and the presence of peripapillary gamma-zone at baseline were identified as major predictors for VFD development[78]. ONH changes, such as LC defects, may promote axonal damage and visual field impairment[83]. However, there was no significant difference in visual field parameters between high myopic patients with or without tilted discs[84].
Other functional changes
-
In addition to VFD, several studies have explored other functional indicators of high myopia, such as electroretinogram (ERG) and contrast sensitivity function (CSF) changes[85,86]. ERG studies report that the b-wave implicit time is prolonged in high myopic patients[87], and further research has shown that b-wave amplitude is negatively correlated with AL[88]. Liu et al. found reduced CSF in high myopic individuals, and it was associated with outer retinal thickness and retinal deep vascular density[86]. However, research on these functional changes is still limited and needs further investigation.
-
The rapid development of multimodal ocular imaging technologies has led to a substantial increase in high myopia data, presenting new opportunities for MON analysis. Deep learning, particularly convolutional neural networks (CNNs) and Transformer models has demonstrated significant advantages in predicting high myopia progression and identifying associated complications, especially in detecting and grading myopic maculopathy[89−92]. Foundational progress has been made in MON-related morphological and functional investigations. Early studies commonly employed deep learning algorithms for automated segmentation and parameter extraction of key anatomical structures in high myopia, including optic disc, PPA, and RNFL[93−95]. For example, Cho et al.[96] developed an AI-based system for detecting optic disc tilt, effectively addressing the limitations of time-consuming analysis and inter-observer variability in traditional clinical practice. Additionally, AI systems excel at detecting subtle morphological features that may be overlooked in routine clinical examinations. A study using CNNs established a three-dimensional (3D) OCT diagnostic model for detecting LC defects[97], enabling more precise characterization of defect morphology and spatial localization. Regarding functional changes in high myopia, Li et al.[78] have developed prediction models to differentiate the development of VFD.
A key challenge in current AI research on MON is the lack of standardized diagnostic criteria and specialized datasets, which hinders large-scale labeling efforts. Additionally, phenotypic overlap with glaucoma-related optic neuropathy (GON) often leads to the misclassification of MON as false-positive glaucoma in existing studies. However, methodological insights from AI research on glaucoma and other optic neuropathies could inform AI applications in MON[98,99]. For instance, existing techniques for ONH identification, localization, and extraction could be adapted through transfer learning to detect myopic optic discs, with algorithmic optimizations tailored to the characteristic tilt and morphological variations in high myopia to enhance detection accuracy[100]. Moreover, methodological frameworks for modeling RNFL abnormalities could provide valuable insights into AL-related changes in high myopia[101].
-
Myopic optic neuropathy (MON) is a crucial area requiring further research. Currently, no unified definition exists for optic nerve damage associated with high myopia. The International Myopia Institute (IMI) Clinical Summary defines myopia-associated glaucoma (MAG)-like optic neuropathy as optic neuropathy characterized by a loss of neuroretinal rim and enlargement of the optic cup, occurring in highly myopic eyes with a secondary macro disc or peripapillary delta zone at normal IOP[1]. However, MON is not limited to glaucoma-like optic nerve damage. More recently, Shin et al.[102] defined MON as myopic eyes with nonglaucomatous RNFL and visual field (VF) damage, characterized by superonasal or nasal RNFL thinning and corresponding inferotemporal VF defects. However, the above definition does not include additional morphological changes such as ONH size and shape, gamma zone, ganglion cell changes, and microvascular changes. To better understand and manage MON, it is crucial to establish a population-based database of morphological and functional parameters for high myopia, and to develop a standardized grading and classification system.
Myopic optic nerve damage often coexists with glaucoma, complicating the disease research and clinical differential diagnosis[9]. For example, glaucoma diagnosis typically involves measuring retinal layer thickness, but the elongated shape of high myopic eyes interferes with OCT scanning, leading to image distortion that may mask or mimic glaucomatous degeneration[101]. Clinically, MON in high myopia and glaucoma-related optic neuropathy (GON) share similarities. Yet, subtle differences in fundus imaging and functional changes may serve as diagnostic markers to distinguish GON from MON[9]. However, the relationship between varying degrees of high myopia and GON progression remains unclear, and further research is needed to address this issue. In terms of treatment, IOP reduction has proven effective in highly myopic eyes with glaucomatous or glaucoma-like optic nerve damage. However, treatment strategies for nonglaucomatous, eye elongation-related, or mechanically induced optic nerve damage remain unclear and require further exploration[103]. One study has suggested that retrobulbar and systemic glucocorticoid therapy may benefit patients with acute-onset MON[104], although controlled clinical trials are needed to validate these findings. Future research integrating multimodal imaging and comparing therapeutic interventions may advance MON management strategies.
For experimental research, further investigation into the mechanisms underlying high myopia-induced fundus changes is essential, particularly the vascular and tractional mechanisms associated with optic nerve damage[105,106]. Whether these changes occur simultaneously or if one leads to the other is still uncertain. A deeper understanding of these mechanisms will provide valuable insights for future prevention and treatment strategies.
To achieve transformative progress of MON AI development, future research should integrate multiple parameters, including morphological, functional, and vascular features into AI-driven analysis, potentially uncovering novel correlations and enabling more effective detection and monitoring of MON[107,108]. Crucially, leveraging multimodal correlation analysis capabilities of AI to develop refined differentiation models between myopic and glaucomatous optic neuropathies will be essential to overcome their anatomical similarities[109,110].
In summary, with the increasing global prevalence of high myopia, it is crucial to address these knowledge gaps as a public health priority. This will help alleviate the burden of optic nerve damage and visual impairment, paving the way for more effective clinical management strategies.
-
Not applicable.
The study was supported by the Start-up Fund for RAPs under the Strategic Hiring Scheme (Grant No. P0048638) from the Hong Kong Polytechnic University, PolyU - Rohto Centre of Research Excellence for Eye Care (Grant No. P0046333), and Henry G. Leong Endowed Professorship in Elderly Vision Health. We thank the InnoHK HKSAR Government for providing valuable support. The research work described in this paper was conducted in the JC STEM Lab of Innovative Light Therapy for Eye Diseases, funded by The Hong Kong Jockey Club Charities Trust. We also extend our appreciation to Jinze Zhang, a PhD candidate from Sun Yat-sen University, for kindly providing the personal fundus images. Data in (Fig. 2b) were obtained from the HPMI database (Huang, Shenghai; Li, Zhongwen; Lin, Bing; Zhang, Shaodan; Yi, Quanyong; Wang, Lei. HPMI: A retinal fundus image dataset for the identification of high and pathological myopia based on deep learning. Figshare dataset:
https://doi.org/10.6084/m9.figshare.24800232.v1 ).-
The authors confirm the contribution to the paper as follows: study conception and design: He M; data collection: Chen X; analysis and interpretation of results: Chen X, Chen Y; writing - original draft preparation: Chen X, Chen Y; writing - review and editing: Ding X, Wang Y, Shi D, He M. All authors reviewed the results and approved the final version of the manuscript.
-
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
-
The authors declare that they have no conflict of interest.
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Chen X, Chen Y, Ding X, Wang Y, Shi D, et al. 2025. Optic neuropathy in high myopia. Visual Neuroscience 42: e008 doi: 10.48130/vns-0025-0007 

Optic neuropathy in high myopia
- Received: 30 December 2024
- Revised: 27 March 2025
- Accepted: 31 March 2025
- Published online: 13 June 2025
Abstract: Myopia, particularly high myopia, has become a significant global public health issue due to its increasing prevalence. High myopia is associated with various ocular complications, including early-onset cataracts, glaucoma, retinal detachment, and myopic maculopathy, yet optic nerve damage is often overlooked. This article reviews the morphological changes in the optic disc, peripapillary region, and retinal layers, along with the relevant functional defects. Additionally, recent advancements in artificial intelligence (AI)-related research in this field are summarized. The article also highlights the need for developing a standardized grading and classification system for high-myopic optic neuropathy, supported by large-scale, high-quality longitudinal cohort studies to explore the relationships between myopic optic neuropathy and other complications, experimental research to uncover the underlying mechanisms of optic nerve damage, and the integration of AI - all of which are essential for improving diagnostic accuracy, monitoring, and treatment strategies for high myopia patients at risk of progressive vision loss.
-
Key words:
- High myopia /
- Myopia /
- Optic neuropathy /
- Optic nerve head /
- Retinal nerve fiber layer /
- Ganglion cell /
- Visual field defect /
- Retina /
- Artificial intelligence