










-
Papilledema, characterized by swelling of the optic disc due to increased intracranial pressure, is a critical clinical finding that often signals severe neurological disorders[1−3]. While traditional causes of papilledema are well-documented, including brain tumors, intracranial hemorrhages, and idiopathic intracranial hypertension (IIH)[4]. Emerging evidence suggests that certain pharmacological agents may contribute to its development.
The recognition of drug-associated papilledema is critical for timely diagnosis and management. Certain medications, such as amiodarone[5] and mitotane[6], have been implicated in raising intracranial pressure, leading to papilledema. However, most existing knowledge is derived from isolated case reports or small case series, limiting the ability to generalize findings and hindering comprehensive risk assessment.
The Food and Drug Administration's (FDA) Adverse Event Reporting System (FAERS) offers a valuable tool for pharmacovigilance, systematically collecting adverse events and medication errors reported from healthcare professionals, consumers, and manufacturers. Disproportionality analysis of the FAERS database enables the detection of potential safety signals by comparing the observed and expected frequencies of specific adverse events associated with drugs[7,8]. This method has been effective in identifying rare but serious adverse drug reactions, thereby informing clinical practice and regulatory decisions.
This study utilizes the FAERS database to assess the risk signals of drug-induced papilledema through disproportionality analysis from 2004 to 2023. We aimed to provide more evidence to support clinical practice and drug safety regulation through this research.
-
The data for this study were sourced from the FAERS database, covering the period from the first quarter (Q1) of 2004 to the fourth quarter (Q4) of 2023. The database comprises seven standardized tables: DEMO (demographic information, including patient age, sex, body weight, reporting country, and event date), DRUG (drug names, routes of administration, and role codes indicating whether the drug was the primary suspect [PS], secondary suspect [SS], concomitant [C], or interacting [I]), REAC (adverse event terms coded using MedDRA preferred terms), OUTC (clinical outcomes, such as death, hospitalization, disability, life-threatening events, and other serious conditions), THER (start and end dates of drug therapy), INDI (drug indications coded using MedDRA terms), and RPSR (report sources, such as healthcare professionals, consumers, or manufacturers). All data were imported into PostgreSQL for analysis. A detailed list of all extracted variables is provided in Supplementary Table S1.
Identification of adverse reactions
-
In this study, adverse drug events were identified based on the MedDRA. We used the preferred term Papilledema (PT code: 10033712) to identify relevant cases. Inclusion criteria were: (1) reports containing Papilledema as a coded adverse event; (2) the drug was listed as the primary suspect (PS). Exclusion criteria included: (1) duplicate reports, identified by retaining only the latest case report based on CASEID and FDA_DT fields; (2) drug-event combinations with fewer than three case reports; (3) drugs specifically indicated for the treatment of papilledema or its underlying conditions.
Statistical analysis
-
Consistent with a previous study, we conducted a disproportionality analysis to detect signals of drug-induced papilledema[9]. This analysis compared the reporting odds ratio (ROR), proportional reporting ratio (PRR), Bayesian Confidence Propagation Neural Network (BCPNN), and Multi-item Gamma Poisson Shrinker (MGPS) across various drugs. Following prior studies, positive signal identification criteria are established as outlined in Supplementary Tables S2 and S3. A potential signal for papilledema-inducing drugs was identified when any of the following criteria were met: (1) ROR: a ≥ 3 and 95% CI lower > 1; (2) PRR: a ≥ 3 and 95% CI lower > 1; (3) BCPNN: IC025 > 0; and (4) MGPS: EBGM05 > 2 and a > 0. These criteria were applied to ensure the reliable detection of potential papilledema-inducing drugs.
-
The study analyzed FAERS data spanning from January 2004 to December 2023, with a total of 20,629,811 raw reports. After removing duplicate values (n = 3,250,202), the remaining dataset comprised 17,379,609 FAERS reports. Among these, 9,459 adverse drug events (ADEs) were related to papilledema, reported by 3,777 unique patients. A total of 1,197 drug products were identified in relation to papilledema-related ADEs.
To refine the data, duplicate drugs and those with fewer than three reports were excluded, leaving 315 drugs associated with papilledema-related ADEs. A disproportionality analysis was conducted on these 315 drugs, resulting in preliminary findings that identified 81 drugs with a positive signal for an association with papilledema (Supplementary Fig. S1).
In this study, the participants had an average age of 37.4 ± 22.0 years, a weight of 66.7 ± 28.0 kg, with 2,148 females, 1,323 males, and 306 with unknown gender (Supplementary Table S4). The number of drug-induced papilledema-related ADEs reported was higher among females, primarily within the 20–30 age range (Fig. 1a). Temporal trends from 2004 to 2023 showed a gradual increase in reported papilledema cases, with notable peaks in 2017 and 2018. The number of cases reported of females was consistently higher each year than that of males (Fig. 1b). In terms of clinical outcomes, 61% of papilledema cases were classified as Other serious conditions, and 26% as Hospitalization (Fig. 1c). Most reports (1,380 cases) were submitted by healthcare professionals (Fig. 1d). Geographically, the highest numbers of reported cases were from the United States (Fig. 1e). Regarding the routes of drug administration, there were 1,090 cases associated with oral administration and 1,531 cases involving other routes (Fig. 1f).
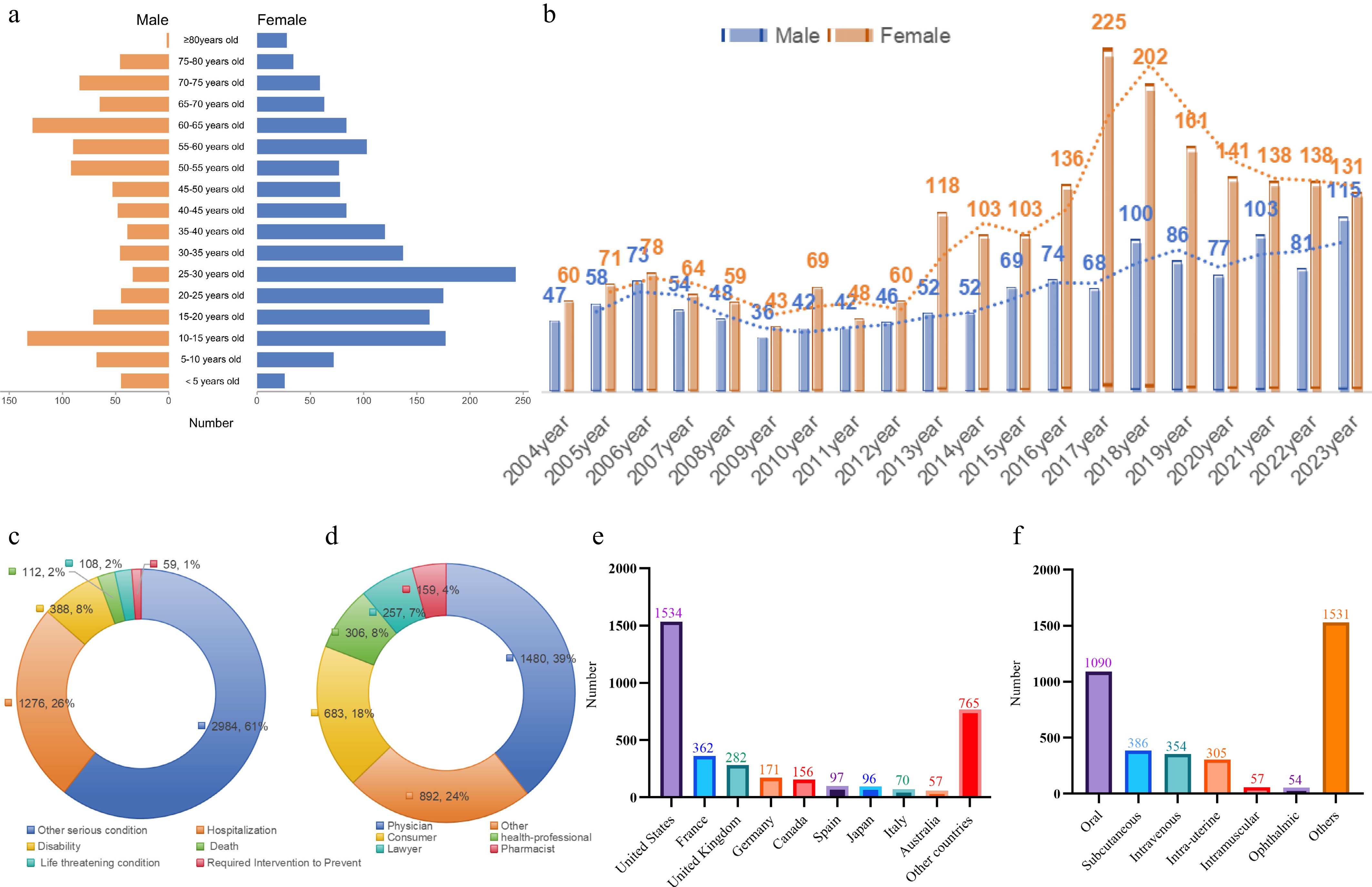
Figure 1.
Baseline characteristics of drug-induced papilledema cases. (a) Age and gender distribution of papilledema-related ADEs. (b) Annual trend of papilledema cases reported from 2004 to 2023. (c) Distribution of clinical outcomes for papilledema cases. (d) Distribution of report sources. (e) Distribution of reporting countries. (f) Distribution of routes of administration among papilledema-related reports.
Positive drugs identified through disproportionality analysis and ATC classification
-
After removing duplicate data and excluding drugs specifically used for the treatment of papilledema, a total of 51 drugs were selected for subsequent classification analysis.
To further evaluate and categorize these drugs, we used the Anatomical Therapeutic Chemical (ATC) classification system to group them according to their action categories (Fig. 2a). These drugs cover ten categories: Antineoplastic and immunomodulating agents (n = 20), Anti-infectives for systemic use (n = 7), Genito urinary system and sex hormones (n = 7), Nervous system (n = 4), Respiratory system (n = 3), Systemic hormonal preparations (n = 3), Cardiovascular system (n = 2), other medication (n = 2), Sensory organs (n = 2), and Dermatologicals (n = 1). Additional statistical values and the distribution of drug-induced papilledema can be found in Supplementary Table S5.
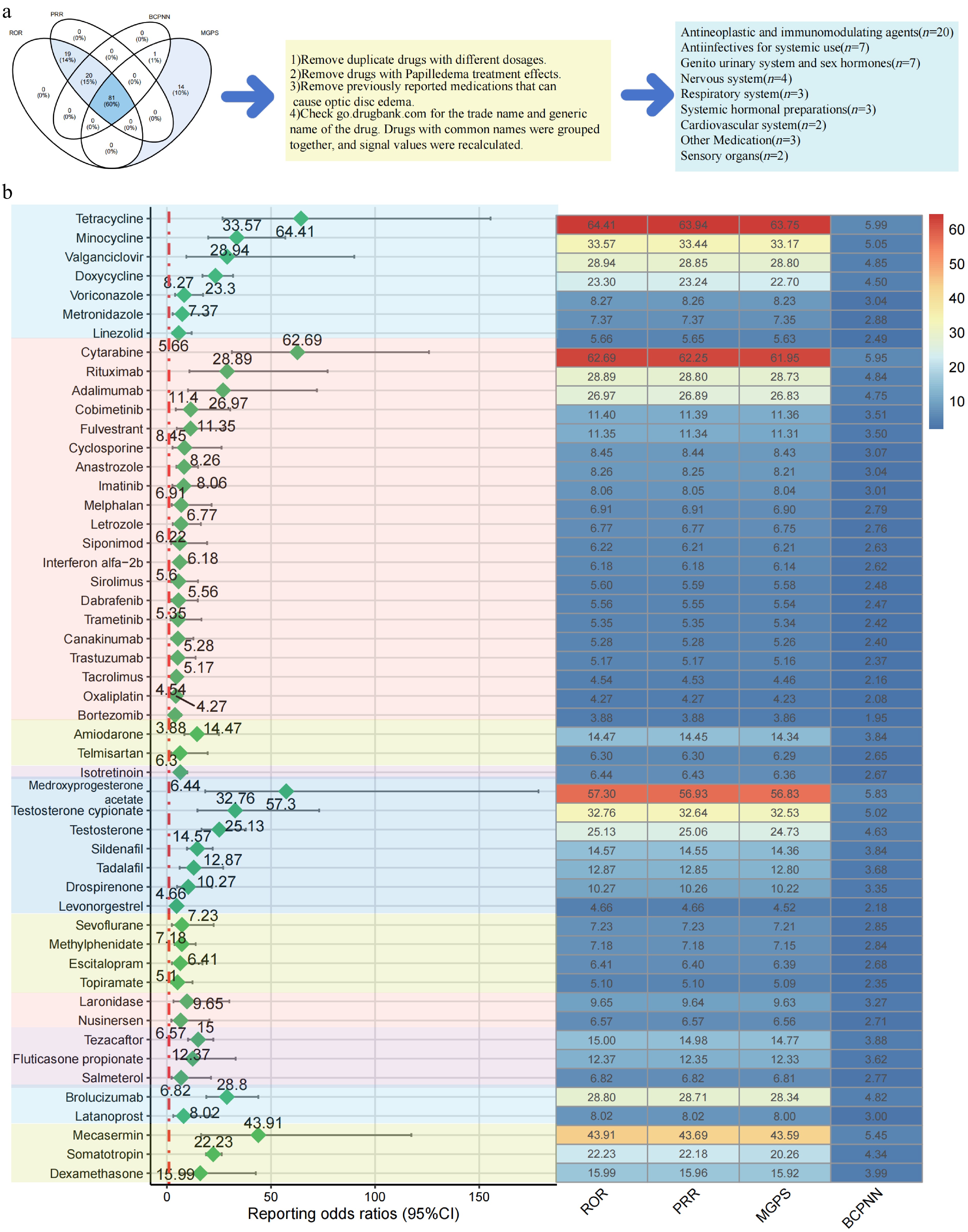
Figure 2.
Drugs associated with papilledema identified by disproportionality analysis. (a) Flowchart of drug screening and categorization. (b) Reporting odds ratios (ROR) of identified drugs grouped by ATC classification.
As shown in Fig. 2b, among the drugs within the Antiinfectives for Systemic Use category, tetracycline exhibited the highest ROR (64.41), followed by minocycline (33.57), valganciclovir (28.94), and doxycycline (23.30). In the Antineoplastic and Immunomodulating Agents category, cytarabine displayed the strongest association with papilledema (62.69), followed by rituximab (28.89), adalimumab (26.97), and cobimetinib (11.40). For the Cardiovascular System, amiodarone showed a substantial ROR (14.47), while telmisartan exhibited a moderate signal (6.30). In the Dermatologicals category, isotretinoin was the only drug with a positive signal (6.44). Within the Genito Urinary System and Sex Hormones, medroxyprogesterone acetate displayed the highest ROR (57.30), followed by testosterone cypionate (32.76), testosterone (25.13), and sildenafil (14.57). In the Nervous System category, sevoflurane (7.23) and methylphenidate (7.18) had the strongest signals, with escitalopram (6.41) and topiramate (5.10) showing moderate associations. For Respiratory System drugs, tezacaftor exhibited the highest signal (15.00), followed by fluticasone propionate (12.37) and salmeterol (6.82). In the Sensory Organs category, brolucizumab had a significant ROR (28.80), while latanoprost displayed a lower but still noteworthy signal (8.02). In the Systemic Hormonal Preparations group, mecasermin (43.91) and somatotropin (22.23) exhibited high ROR values, with dexamethasone also showing a notable signal (15.99). Lastly, in the Other Medications category, laronidase (9.65) and nusinersen (6.57) were identified with positive signals.
Classification of medications based on literature reports with papilledema
-
Through a comprehensive literature review in Pubmed, Google Scholar and Embase, we identified drugs that were either previously reported to be associated with drug-related papilledema or had not been reported in this context. Among them, 21 drugs were previously reported, while 30 drugs had not previously been linked to papilledema. Previously known drugs mainly (Fig. 3) focus on medications used for anti-infection and anti-tumor treatments. The detailed information on the reported medications can be found in Table 1 and Supplementary Table S6.
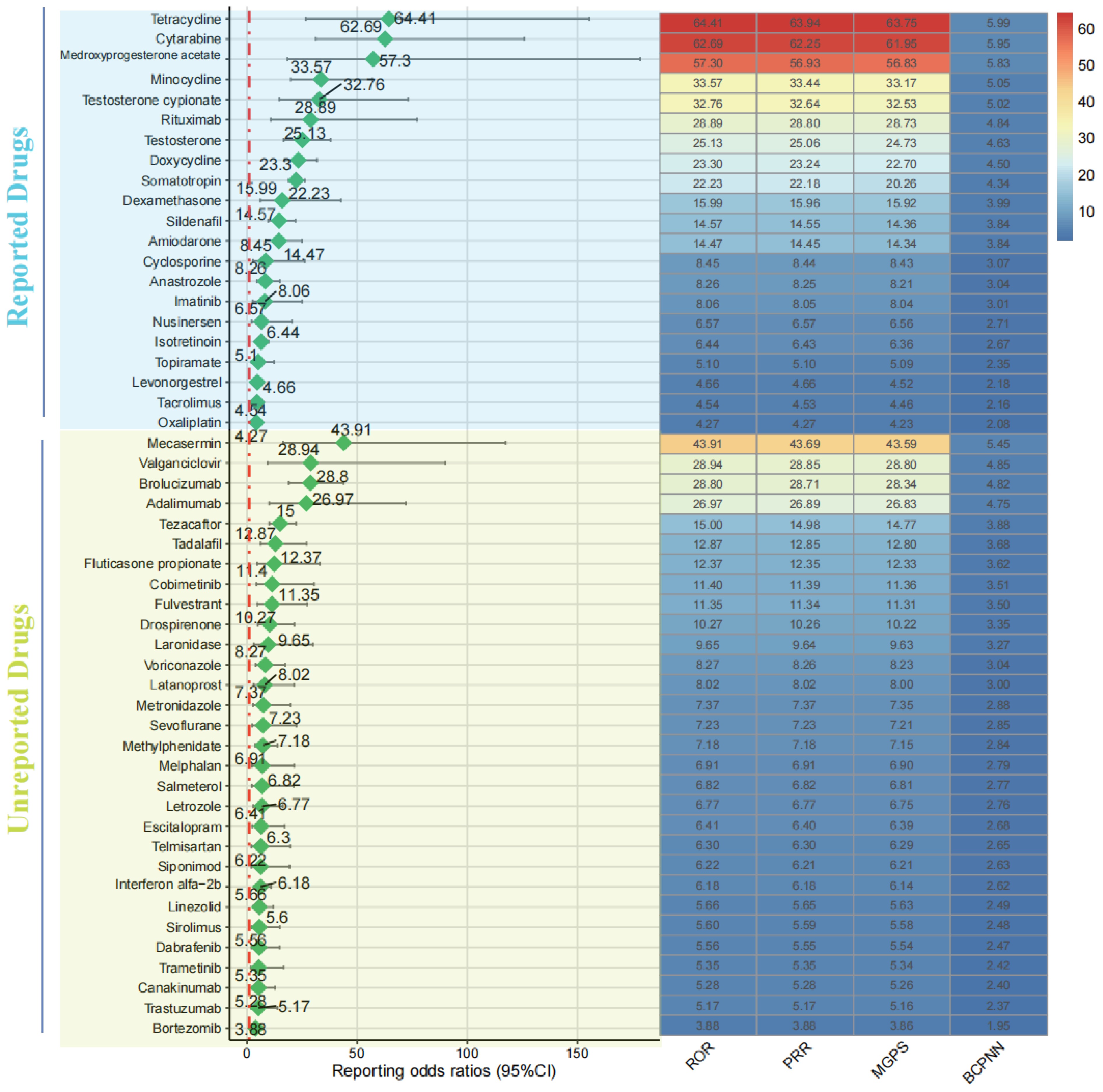
Figure 3.
Classification of medications based on literature reports with papilledema.
Table 1. Overview of reported cases of drug-induced papilledema.
Generic names of drugs Primary actions of drugs Ref. Levonorgestrel Hormone replacement therapy [10] Doxycycline
SomatotropinAntibacterial activity
Promotion of growth[11]
[12]Tetracycline Antibacterial activity [13] Minocycline Antibacterial activity [14,15] Cytarabine Antitumor actions [16] Medroxyprogesterone acetate Hormone replacement therapy [17] Testosterone cypionate Hormone replacement therapy [18] Rituximab Antitumor actions [19] Testosterone Hormone replacement therapy [20] Amiodarone Management of ventricular and atrial arrhythmias [21,22] Sildenafil
Dexamethasone
Anastrozole
IsotretinoinTreatment of erectile dysfunction
Anti-inflammatory effects
Antitumor actions
Long-term acne control[23]
[24]
[25]
[26]Cyclosporine Immunosuppressive activity [27] Imatinib Antitumor actions [28] Nusinersen Treat spinal muscular atrophy [29] Tacrolimus Prevention of organ transplant rejection [30] Topiramate Anticonvulsant activity [31] Oxaliplatin Antitumor actions [32] Drugs with papilledema classification by risk degree and duration
-
We further used BCPNN values to assess the risk ranking of drugs and analyzed the median induction time for adverse events associated with each drug (Fig. 4). The BCPNN values were classified as follows: values between 0 and 1.5 indicated a weak risk of drug-related papilledema; values between 1.5 and 3 suggested a moderate risk; and values above 3 indicated a high risk. The drugs identified as high risk included Tetracycline, Cytarabine, Medroxyprogesterone acetate, Mecasermin, Minocycline, Testosterone cypionate, Valganciclovir, Rituximab, Brolucizumab, and Adalimumab. Based on the classification of drug-related ocular adverse events by duration of use, further analysis using overall drug quartiles was conducted. The drugs that induce ocular adverse events for the shortest duration include Fulvestrant, Medroxyprogesterone acetate, and Sevoflurane. In addition, according to the Kaplan-Meier curve analysis based on the ATC classification, the induction time for 'Anti-infectives for systemic use' was the shortest, while drugs in the 'Other medications' category had the longest induction time (p < 0.001) (Fig. 5).
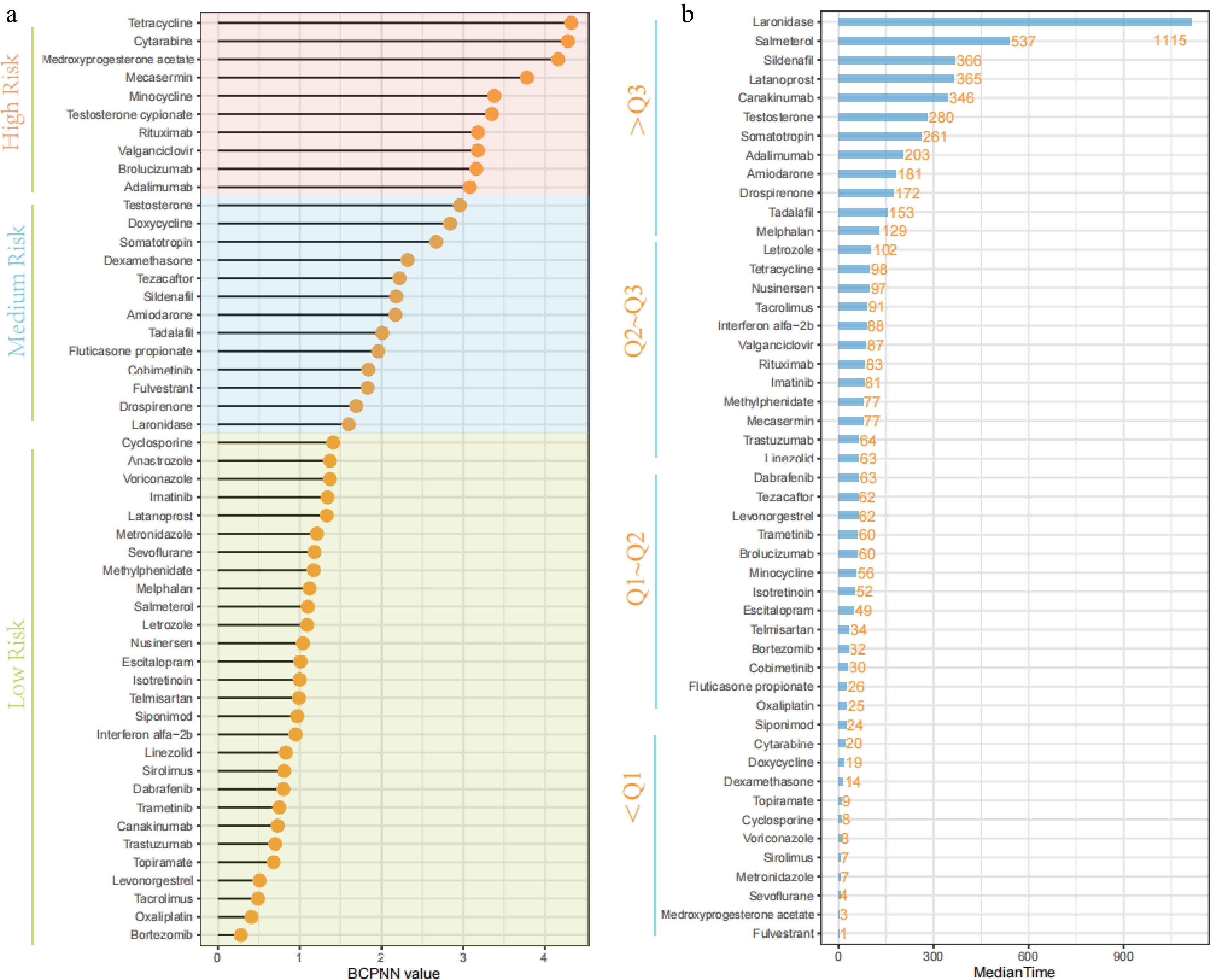
Figure 4.
Ranking of drugs associated with Pppilledema by BCPNN values and induction time. (a) Drugs sorted by BCPNN values. (b) Median induction time for ocular adverse events related to each drug.
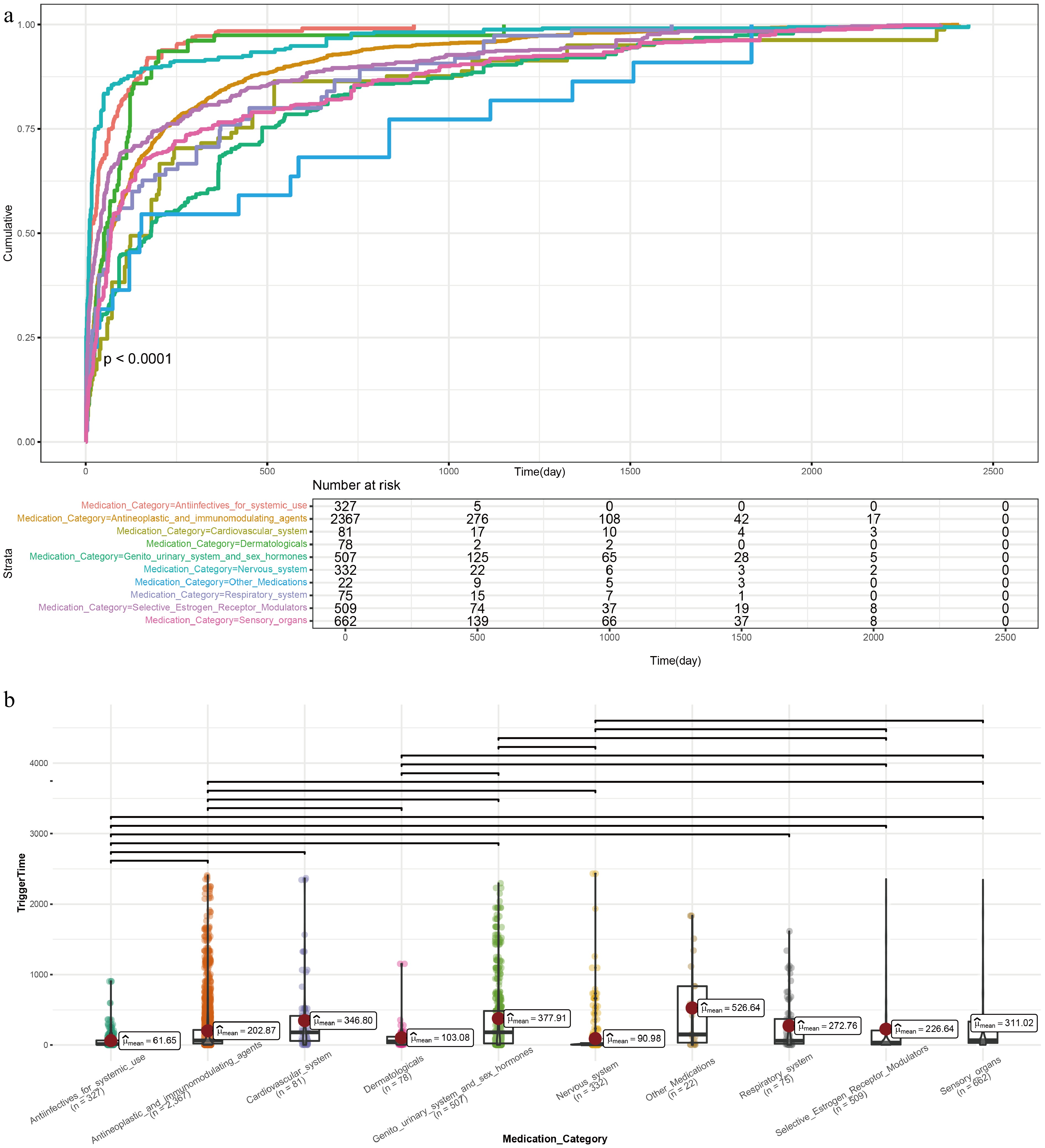
Figure 5.
Time-to-onset analysis of drug-induced papilledema. (a) Kaplan-Meier curves of time to adverse event onset stratified by ATC drug category. (b) Median induction time by ATC drug category. Brackets indicate pairwise comparisons with p < 0.05.
Subgroup and sensitivity analyses
-
To further evaluate the robustness and clinical relevance of the identified signals, we performed subgroup analyses stratified by age (0–18, 18–64, and ≥ 65 years), sex (male vs female), and drug insdication (on-label vs off-label use), as well as a sensitivity analysis restricted to physician-reported cases. The results are presented as a heatmap of ROR values (Fig. 6 and Supplementary Table S7).
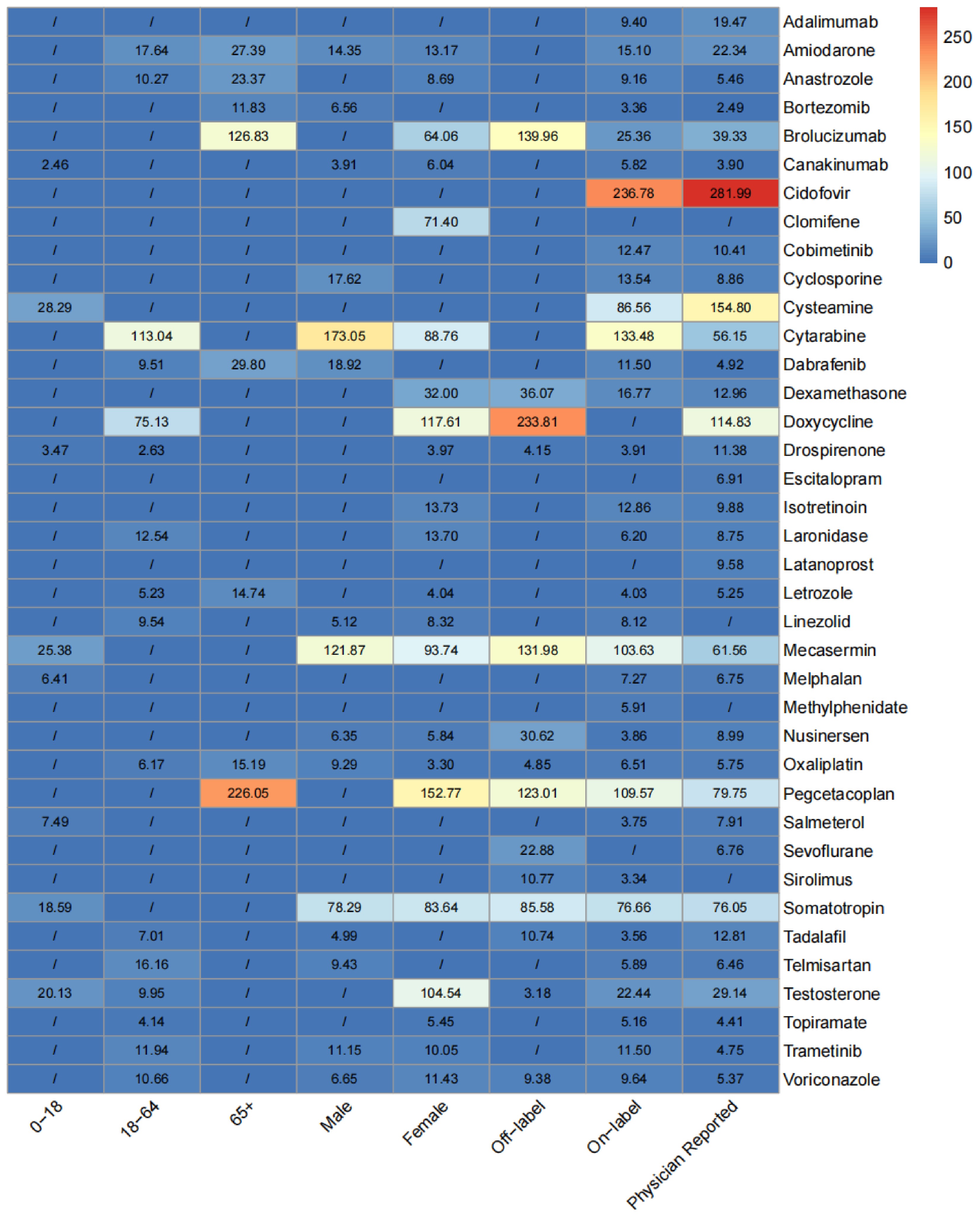
Figure 6.
Subgroup and sensitivity analyses of drug-associated papilledema signals.
Age-stratified analysis
-
Substantial age-dependent differences in the risk signals for drug-associated papilledema were observed across the identified drugs. In the 0–18 years subgroup, eight drugs showed positive signals. The strongest signals were detected for cysteamine (ROR = 28.29, 95% CI: 9.05–88.47), mecasermin (ROR = 25.38, 95% CI: 15.43–41.74), testosterone (ROR = 20.13, 95% CI: 7.51–53.99), and somatotropin (ROR = 18.59, 95% CI: 12.15–28.45). Other drugs with positive pediatric signals included salmeterol (ROR = 7.49, 95% CI: 2.41–23.32), melphalan (ROR = 6.41, 95% CI: 2.06–19.94), drospirenone (ROR = 3.47, 95% CI: 1.11–10.78), and canakinumab (ROR = 2.46, 95% CI: 1.23–4.94).
In the adult subgroup (18–64 years), the largest number of positive signals (16 drugs) was observed. The highest ROR values were detected for cytarabine (ROR = 113.04, 95% CI: 58.52–218.32) and doxycycline (ROR = 75.13, 95% CI: 24.11–234.06), followed by amiodarone (ROR = 17.64, 95% CI: 5.68–54.79), telmisartan (ROR = 16.16, 95% CI: 6.05–43.14), laronidase (ROR = 12.54, 95% CI: 4.04–38.95), trametinib (ROR = 11.94, 95% CI: 3.84–37.06), voriconazole (ROR = 10.66, 95% CI: 4.43–25.65), and anastrozole (ROR = 10.27, 95% CI: 5.68–18.59). Other drugs with moderate signals included testosterone (ROR = 9.95, 95% CI: 6.47–15.30), linezolid (ROR = 9.54, 95% CI: 5.12–17.76), dabrafenib (ROR = 9.51, 95% CI: 3.56–25.36), tadalafil (ROR = 7.01, 95% CI: 3.76–13.04), oxaliplatin (ROR = 6.17, 95% CI: 4.16–9.15), letrozole (ROR = 5.23, 95% CI: 1.69–16.25), topiramate (ROR = 4.14, 95% CI: 1.72–9.96), and drospirenone (ROR = 2.63, 95% CI: 1.41–4.90).
In the elderly subgroup (≥ 65 years), eight drugs showed positive signals with markedly different patterns compared to the younger age groups. Pegcetacoplan exhibited the highest ROR (226.05, 95% CI: 84.12–607.46), followed by brolucizumab (ROR = 126.83, 95% CI: 47.28–340.22), dabrafenib (ROR = 29.80, 95% CI: 9.57–92.81), amiodarone (ROR = 27.39, 95% CI: 13.61–55.15), anastrozole (ROR = 23.37, 95% CI: 11.61–47.04), oxaliplatin (ROR = 15.19, 95% CI: 9.70–23.79), letrozole (ROR = 14.74, 95% CI: 4.73–45.91), and bortezomib (ROR = 11.83, 95% CI: 5.88–23.82).
Sex-stratified analysis
-
Notable sex-specific differences were observed for several drugs. In male patients, 15 drugs showed positive signals. The highest signal was observed for cytarabine (ROR = 173.05, 95% CI: 85.98–348.31), followed by mecasermin (ROR = 121.87, 95% CI: 68.86–215.67) and somatotropin (ROR = 78.29, 95% CI: 48.46–126.49). Other drugs with notable signals in males included dabrafenib (ROR = 18.92, 95% CI: 9.00–39.78), cyclosporine (ROR = 17.62, 95% CI: 7.32–42.44), amiodarone (ROR = 14.35, 95% CI: 6.83–30.17), trametinib (ROR = 11.15, 95% CI: 3.59–34.64), telmisartan (ROR = 9.43, 95% CI: 3.04–29.29), oxaliplatin (ROR = 9.29, 95% CI: 6.64–12.99), voriconazole (ROR = 6.65, 95% CI: 2.49–17.74), bortezomib (ROR = 6.56, 95% CI: 3.71–11.57), nusinersen (ROR = 6.35, 95% CI: 2.05–19.72), linezolid (ROR = 5.12, 95% CI: 2.13–12.33), tadalafil (ROR = 4.99, 95% CI: 2.89–8.62), and canakinumab (ROR = 3.91, 95% CI: 1.26–12.14). In female patients, 22 drugs showed positive signals, representing a broader spectrum of drug-associated papilledema risk. The highest signals were observed for pegcetacoplan (ROR = 152.77, 95% CI: 68.24–341.98), doxycycline (ROR = 117.61, 95% CI: 43.91–315.01), and testosterone (ROR = 104.54, 95% CI: 68.58–159.34). Notably, testosterone showed a strong signal in the female subgroup with no significant signal in males. This finding likely reflects the use of exogenous testosterone in female-to-male transgender patients, a population previously reported to be at increased risk for intracranial hypertension. Similarly, doxycycline showed a positive signal exclusively in females (ROR = 117.61), consistent with the known female predominance of tetracycline-induced pseudotumor cerebri. Other drugs with female-predominant or female-exclusive signals included dexamethasone (ROR = 32.00, 95% CI: 11.99–85.44; female only), clomifene (ROR = 71.40, 95% CI: 22.94–222.25; female only), isotretinoin (ROR = 13.73, 95% CI: 5.15–36.62; female only), and topiramate (ROR = 5.45, 95% CI: 2.83–10.49; female only). Mecasermin (ROR = 93.74, 95% CI: 38.86–226.15), cytarabine (ROR = 88.76, 95% CI: 36.80–214.09), somatotropin (ROR = 83.64, 95% CI: 51.82–134.97), and brolucizumab (ROR = 64.06, 95% CI: 26.58–154.39) also showed strong signals in female patients.
On-label vs off-label use analysis
-
A total of 14 drugs showed significant signals when used off-label. Doxycycline demonstrated the highest off-label signal (ROR = 233.81, 95% CI: 74.76–731.20). Other drugs with notable off-label signals included brolucizumab (ROR = 139.96, 95% CI: 44.87–436.53), mecasermin (ROR = 131.98, 95% CI: 49.26–353.60), pegcetacoplan (ROR = 123.01, 95% CI: 45.92–329.48), somatotropin (ROR = 85.58, 95% CI: 38.28–191.36), dexamethasone (ROR = 36.07, 95% CI: 11.60–112.16), nusinersen (ROR = 30.62, 95% CI: 9.85–95.21), and sevoflurane (ROR = 22.88, 95% CI: 7.36–71.11). Sevoflurane and sirolimus (ROR = 10.77, 95% CI: 3.47–33.47) showed signals exclusively in off-label use.
For on-label use, 33 drugs showed positive signals. The highest on-label signals were observed for cidofovir (ROR = 236.78, 95% CI: 75.44–743.16), cytarabine (ROR = 133.48, 95% CI: 77.18–230.86), pegcetacoplan (ROR = 109.57, 95% CI: 52.01–230.84), mecasermin (ROR = 103.63, 95% CI: 59.96–179.11), and cysteamine (ROR = 86.56, 95% CI: 32.35–231.63). Other drugs with strong on-label signals included somatotropin (ROR = 76.66, 95% CI: 52.78–111.34), testosterone (ROR = 22.44, 95% CI: 16.08–31.33), dexamethasone (ROR = 16.77, 95% CI: 6.29–44.75), amiodarone (ROR = 15.10, 95% CI: 8.35–27.30), cyclosporine (ROR = 13.54, 95% CI: 6.07–30.17), isotretinoin (ROR = 12.86, 95% CI: 5.35–30.93), and cobimetinib (ROR = 12.47, 95% CI: 4.68–33.27).
Sensitivity analysis: physician-reported analysis
-
To assess the robustness of the observed signals and mitigate potential reporting bias from consumer-reported cases, a sensitivity analysis was performed, restricting the dataset to reports submitted by physicians. A total of 33 drugs retained positive signals in this restricted analysis, confirming the overall robustness of the primary findings. The highest signals were observed for cidofovir (ROR = 281.99, 95% CI: 88.94–894.07), cysteamine (ROR = 154.80, 95% CI: 57.44–417.15), doxycycline (ROR = 114.83, 95% CI: 36.68–359.53), pegcetacoplan (ROR = 79.75, 95% CI: 42.69–149.00), somatotropin (ROR = 76.05, 95% CI: 44.82–129.04), mecasermin (ROR = 61.56, 95% CI: 27.53–137.69), and cytarabine (ROR = 56.15, 95% CI: 26.65–118.29). Several drugs that had limited or no significant signals in the age- or sex-stratified analyses still showed robust signals in the physician-reported analysis, including adalimumab (ROR = 19.47, 95% CI: 7.29–52.02), cobimetinib (ROR = 10.41, 95% CI: 3.90–27.79), latanoprost (ROR = 9.58, 95% CI: 3.59–25.58), escitalopram (ROR = 6.91, 95% CI: 2.59–18.45), and sevoflurane (ROR = 6.76, 95% CI: 2.18–20.99).
-
Papilledema is an important clinical signal that prompts neuro-ophthalmologists to conduct further evaluations to identify potential underlying causes and implement appropriate treatment measures[1,33,34]. For drug-induced papilledema, understanding the associated medications and their potential risks is crucial for improving patient management and outcomes.
This study provides a comprehensive and systematic evaluation of drugs associated with papilledema through analysis of the FAERS database spanning nearly two decades. By applying multiple disproportionality measures, we identified 51 drugs that showed statistically robust signals suggestive of a potential association with papilledema. We evaluated these medications based on their intended use, literature reports, risk level, and induction time, with the aim of providing a reference for clinical practice. Our findings reveal a broad spectrum of pharmaceutical agents potentially associated with this serious ocular adverse event.
By applying the ATC classification system, we identified 51 drugs across multiple therapeutic categories, including anti-infectives for systemic use, antineoplastic and immunomodulating agents, genitourinary system and sex hormones, and others. Our study found that antineoplastic and immunomodulating agents are relatively more associated with papilledema. These drugs target rapidly dividing cells to suppress tumor growth or modulate immune responses[35]. However, their effects are not limited to the targeted cells. They can induce various systemic side effects, including immune-mediated responses, infections, or inflammatory reactions[36,37], which may indirectly lead to papilledema by increasing intracranial pressure or altering the permeability of the peripapillary vasculature. Other drug categories also present notable risks, such as anti-infectives for systemic use and genitourinary system and sex hormones. Clinically, anti-infective drugs such as minocycline and doxycycline have been widely recognized as being associated with the development of pseudotumor cerebri, which can lead to papilledema[38,39]. This is consistent with our findings. Furthermore, our study revealed that anti-infective drugs for systemic use have the shortest median induction time, at just 61.25 d, providing new insights into this association. Similarly, genitourinary system and sex hormone drugs may promote papilledema by affecting fluid balance, increasing intracranial pressure, or influencing vascular function[40,41]. This association suggests that patients receiving these treatments, especially those with high-risk factors, should be closely monitored for early signs of papilledema, with treatment adjustments made to prevent vision loss and intracranial hypertension.
Another key finding of this study is that we identified 30 drugs previously unreported to be associated with papilledema. Disproportionality analysis of the FAERS database revealed a significant association between these drugs and the occurrence of papilledema. These drugs, which include commonly used medications such as Brolucizumab, Interferon alfa-2b, and Bortezomib, have not been widely recognized as potential causes of papilledema. Our findings expand the existing literature on drug-induced papilledema and raise awareness for clinicians to be vigilant when prescribing these drugs. Further studies are needed to investigate the causal relationship between these drugs and papilledema and explore the underlying mechanisms, thus guiding clinicians in the rational use of these medications to minimize adverse reactions.
Given that the BCPNN method offers better sensitivity and specificity compared to PRR and ROR[42], we used this method to rank the identified positive drugs. Drug risk ranking not only helps us identify high-risk medications but also serves as a reference for clinicians in drug selection. For instance, in the treatment of specific diseases, multiple therapeutic options may be available, and drug safety becomes an important consideration when choosing a treatment plan. By using the BCPNN ranking, physicians can prioritize drugs with lower BCPNN values, which are associated with a lower risk of inducing papilledema, thereby enhancing treatment safety. For high-risk drugs that must be used, clinicians can implement stricter monitoring measures based on the ranking results to ensure patient safety.
Furthermore, we provided the median induction time for ocular adverse events associated with these drugs. Clinicians can adjust the monitoring frequency based on individual patient conditions. For drugs with a short induction time, closer monitoring should be performed in the early stages of treatment to detect and manage adverse events promptly. For drugs with a longer induction time, regular ocular assessments should be conducted throughout the treatment, especially after prolonged use.
The subgroup analyses revealed population-specific risk profiles that extend the clinical utility of our findings. In the age-stratified analysis, the pediatric subgroup was characterized by strong signals for growth factor–related agents, including cysteamine, mecasermin, and somatotropin, consistent with the known vulnerability of the developing central nervous system to IGF-1-mediated intracranial hypertension[12]. Notably, cysteamine showed a positive signal exclusively in young, likely reflecting both its primary pediatric indication and the greater susceptibility of this population to altered Cerebrospinal Fluid dynamics. A recent study demonstrated that prolonged glucocorticoid use in children with systemic lupus erythematosus was significantly associated with steroid-induced ocular hypertension[43], further supporting the need for routine ophthalmic monitoring in young patients receiving systemic corticosteroid therapy. The adult subgroup (18–64 years) exhibited the broadest spectrum of signals (16 drugs), dominated by cytarabine and doxycycline, while the elderly subgroup (≥ 65 years) showed a distinct pattern driven by pegcetacoplan and brolucizumab, both recently approved agents whose association with papilledema has not been widely recognized.
The sex-stratified analysis revealed that females had a broader spectrum of positive signals (22 drugs) compared to males (15 drugs), consistent with the known female predominance of idiopathic intracranial hypertension. A notable finding was that testosterone showed a strong signal in females with no significant signal in males. This likely reflects exogenous testosterone use in female-to-male transgender patients, a population in which intracranial hypertension has been previously reported[18,20,40]. Doxycycline, dexamethasone, clomifene, and isotretinoin also showed female-exclusive signals, reinforcing the established association between these agents and pseudotumor cerebri in women[11,38,39]. Conversely, cyclosporine, dabrafenib, and telmisartan showed male-exclusive signals, suggesting that the traditional female-focused monitoring paradigm for intracranial hypertension may not capture all at-risk populations.
The on-label vs off-label analysis provided novel insights into how the clinical context of drug use influences papilledema risk. Doxycycline exhibited a high off-label signal with no on-label signal, suggesting that off-label prescribing scenarios may carry amplified risk, potentially due to differences in dosing or patient comorbidity profiles. Sevoflurane and sirolimus also showed exclusively off-label signals. In contrast, cidofovir and cysteamine showed high signals exclusively in on-label use, indicating an inherent pharmacological association at approved indications. These discordant patterns highlight the importance of considering prescribing context when evaluating papilledema risk.
The sensitivity analysis restricted to physician-reported cases confirmed the robustness of our primary findings, with 33 drugs retaining positive signals. The highest signals were observed for cidofovir, cysteamine, and doxycycline. Several newly identified drugs with limited subgroup signals, including adalimumab, cobimetinib, and escitalopram, demonstrated robust signals in physician-reported cases, supporting the clinical plausibility of these associations.
These subgroup analyses provide a framework for individualized monitoring: pediatric patients on growth factor therapy or cysteamine warrant routine fundoscopic evaluation; transgender men on testosterone therapy should be monitored for signs of intracranial hypertension; elderly patients receiving pegcetacoplan or brolucizumab should have optic disc assessment incorporated into regular follow-up; and off-label prescribing of doxycycline and sevoflurane should prompt heightened vigilance for papilledema.
This study has some limitations. First, the FAERS database is based on spontaneous reports, which may lead to reporting bias. Second, the disproportionality analysis used in this study, although effective in revealing associations between drugs and adverse events, cannot establish causality. Additionally, since the risk of drug-induced papilledema may vary with individual patient factors (e.g., comorbidities, immune status, lifestyle factors), this study did not account for these variables. Future studies could build upon this framework to develop clinical prediction models that incorporate patient demographics, drug characteristics, and baseline ophthalmic findings to quantify individualized papilledema risk[44]. An important consideration in interpreting our findings is the potential for confounding by indication, whereby the underlying disease rather than the drug itself may contribute to the observed association with papilledema. To partially mitigate this concern, we restricted our analysis to drugs coded as the primary suspect in FAERS reports, which indicates that the reporting clinician or patient considered the drug to be the most likely cause of the adverse event. Additionally, we excluded drugs used specifically for the treatment of papilledema or its known underlying conditions. Nevertheless, we acknowledge that disproportionality analysis cannot fully control for confounding by indication, and the observed associations should be interpreted as hypothesis-generating signals that warrant further investigation through controlled clinical studies.
-
This study comprehensively identified drugs potentially associated with papilledema through disproportionality analysis, providing key insights into the drug risk intensity and induction time. These findings offer valuable guidance for clinicians when prescribing these medications to high-risk patients, helping to optimize drug safety management. Future research should further explore the mechanisms by which these drugs induce papilledema to develop more precise clinical monitoring and intervention strategies, ultimately reducing the occurrence of adverse events related to papilledema.
-
The study analyzed only publicly available, de-identified reports from the FAERS. Because no human subjects were directly involved and no identifiable private information was collected, review by an institutional ethics committee and written informed consent were not required.
-
The authors confirm contributions to the paper as follows: study conception and design: Xiao K, Chen X; statistical analysis: Chen X, Wu S; administrative, technical and material support: Huang Y, Qi Z, Chen R, Wang Y; draft manuscript preparation: Xiao K; manuscript revision: Lu W, Liu J; supervision: Li L. All authors reviewed the results and approved the final version of the manuscript.
-
The data for this study can be accessed from the FAERS database (www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers-database).
-
The work was supported by the Fujian Provincial Health System Young and Middle-Aged Key Talent Development Program (Grant No. 2025GGA002) the Natural Science Foundation of Fujian Province, China (Grant No. 2024J011019) and Fujian Provincial Science and Technology Innovation Joint Fund Project (Grant No. 2025Y9036) approved by the Fujian Provincial Department of Science and Technology, Fujian, China. Li Li acknowledges support from the China Scholarship Council–the University of Melbourne PhD Scholarship for living expenses.
-
The authors declare that the research was conducted in the absence of any commercial relationships that could be construed as a potential conflict of interest.
-
accompanies this paper online at: https://doi.org/10.48130/vns-0026-0028.
-
# Authors contributed equally: Kunhong Xiao, Xiaodong Chen
- Supplementary Table S1 Variables Extracted from the FAERS Database (Q1 2004 – Q4 2023).
- Supplementary Table S2 Four-grid table of disproportionality analysis method.
- Supplementary Table S3 Principle of dis-proportionality measure and standard of signal detection.
- Supplementary Table S4 Baseline data of papilledema patients reported in the FAERS database.
- Supplementary Table S5 Statistical values and distribution of drug-induced papilledema.
- Supplementary Table S6 Overview of reported drugs associated with papilledema: mechanism classification.
- Supplementary Table S7 Reporting odds ratio (ROR) and 95% confidence interval (95%CI) for different subgroups of drug-related papilledema.
- Supplementary Fig. S1 Flowchart of data extraction for identifying drugs associated with adverse drug events (ADEs) of papilledema.
- Copyright: © 2026 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Xiao K, Chen X, Wu S, Lu W, Chen R, et al. 2026. Large-scale real-world evaluation of drug-associated papilledema. Visual Neuroscience 43: e031 doi: 10.48130/vns-0026-0028 

Large-scale real-world evaluation of drug-associated papilledema
- Received: 18 December 2025
- Revised: 19 March 2026
- Accepted: 08 April 2026
- Published online: 30 June 2026
Abstract: Although drug-papilledema associations have been reported in numerous case reports and small case series, a large-scale pharmacovigilance evaluation across multiple drug categories remains lacking. This study aimed to identify drugs associated with papilledema using disproportionality analysis of the FDA Adverse Event Reporting System (FAERS) database covering the first quarter of 2004 to the fourth quarter of 2023. The term papilledema from the Medical Dictionary for Regulatory Activities (MedDRA) was used to identify relevant cases, and four disproportionality methods (ROR, PRR, BCPNN, and MGPS) were applied to detect positive signals. A total of 51 drugs were identified, of which 21 had been previously reported, and 30 were newly identified. Antineoplastic and immunomodulating agents were the most frequently implicated category, followed by anti-infectives for systemic use, genitourinary system, and sex hormones. The highest-risk drugs by BCPNN ranking were tetracycline, cytarabine, and medroxyprogesterone acetate, while fulvestrant, medroxyprogesterone acetate, and sevoflurane exhibited the shortest onset times. Subgroup analyses revealed distinct population-specific risk patterns: the pediatric population showed vulnerability to growth factor–related agents, testosterone showed a paradoxically stronger signal in females than in males, and doxycycline exhibited a high signal exclusively in off-label use. A sensitivity analysis restricted to physician-reported cases confirmed the robustness of the findings, with 33 drugs retaining positive signals. This study offers clinicians actionable guidance for individualized monitoring and drug safety management in patients at risk of drug-induced papilledema.